The goals of dysphagia management are to minimise the risk of aspiration and to prevent and treat dehydration and malnutrition. Effective management of dysphagia requires a multidisciplinary approach, led by the speech and language therapist (SLT). The SLT assesses the patient’s swallowing function using videofluoroscopy or flexible endoscopic evaluation and may recommend swallow rehabilitation, compensation strategies and dietary adjustments.
Compensation strategies
Swallow rehab involves exercises to train muscles or muscle groups, eg. the tongue muscles. As a result of these exercises, the patient should be able to make a better bolus in the mouth prior to swallowing.
Compensation strategies help patients to avoid problems during eating and drinking (such as choking and coughing) by turning or tilting the head to the affected side, which helps to protect the airway.
Examples of compensation strategies include chin tuck movements, good positioning during and immediately after meals and postural compensation to accommodate any unilateral weakness.
However, effective management also requires input from a range of stakeholders outside of the SLT; these include dietitians, doctors, nurses, occupational therapists, pharmacists, catering staff, carers and the patient themselves.
SLTs work particularly closely with dietitians, who assess the nutritional status of patients, their nutrition and hydration requirements and their ability to meet these requirements safely. The dietitian then advises on food and fluid choices to best meet the patient’s requirements.
In reality, nutritional management of dysphagia is an ongoing journey of multidisciplinary buy-in; a delicate balancing act of evidence-based policies, competing priorities and the busy reality of day-to-day healthcare.
Texture modified foods and fluids
Dietary adjustments, unlike swallow rehab and the compensation exercises mentioned above, invariably generate more discussion among healthcare professionals and patients alike as foods and fluids are such central aspects to everyday life.
Thickening fluids and modifying the texture of food are valid management strategies for dysphagia.1 They make swallowing foods and fluids easier because they have a delayed transit time from the mouth through the pharynx and into the oesophagus, allowing time for the epiglottis to protect the pathway to the lungs in order to avoid aspiration.
Conversely, some patients have trouble clearing fluids (in some cases due to weakened oesophageal peristalsis), so over-thickening can result in pharyngeal residue and a delayed aspiration of thickened fluids into the airway. This is particularly worrying if a patient silently aspirates, showing no signs of airway penetration.
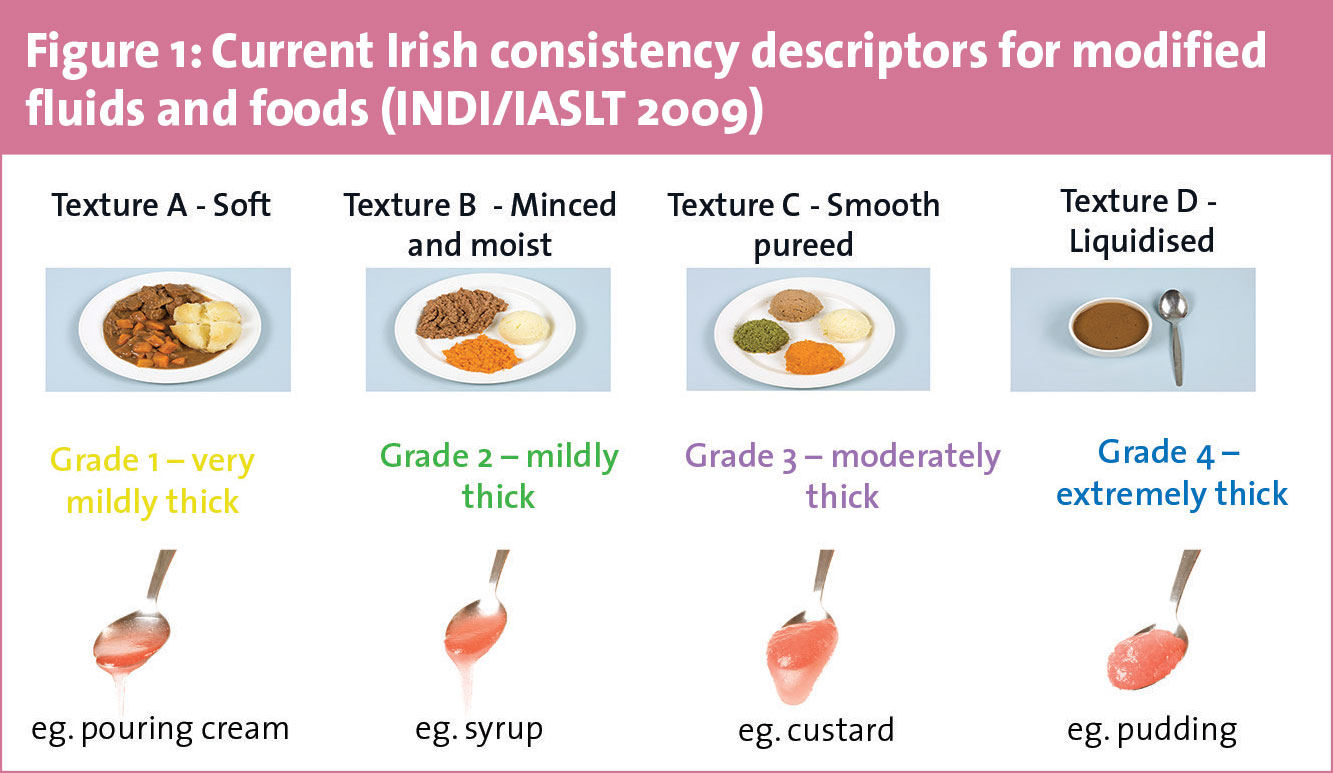
In the Republic of Ireland, foods and fluids are modified according to the Irish Consistency Descriptors for Modified Fluids and Food,2 which were developed in 2009 by the Irish Association of Speech and Language Therapy and the Irish Nutrition and Dietetic Institute (see Figure 1).
(click to enlarge)
Food textures range from least modified (texture A) to most modified (texture D), while fluids vary from naturally thick consistencies (grade 1) to extremely thick consistencies (grade 4).
Some fluids naturally meet the criteria to be grades 1, 2, 3 or 4. Many fluids need to be thickened to the prescribed grade by the manual addition of thickening powders. Texture C (smooth purée) foods may also require addition of a thickening powder to prevent leakage of free fluid after puréeing.
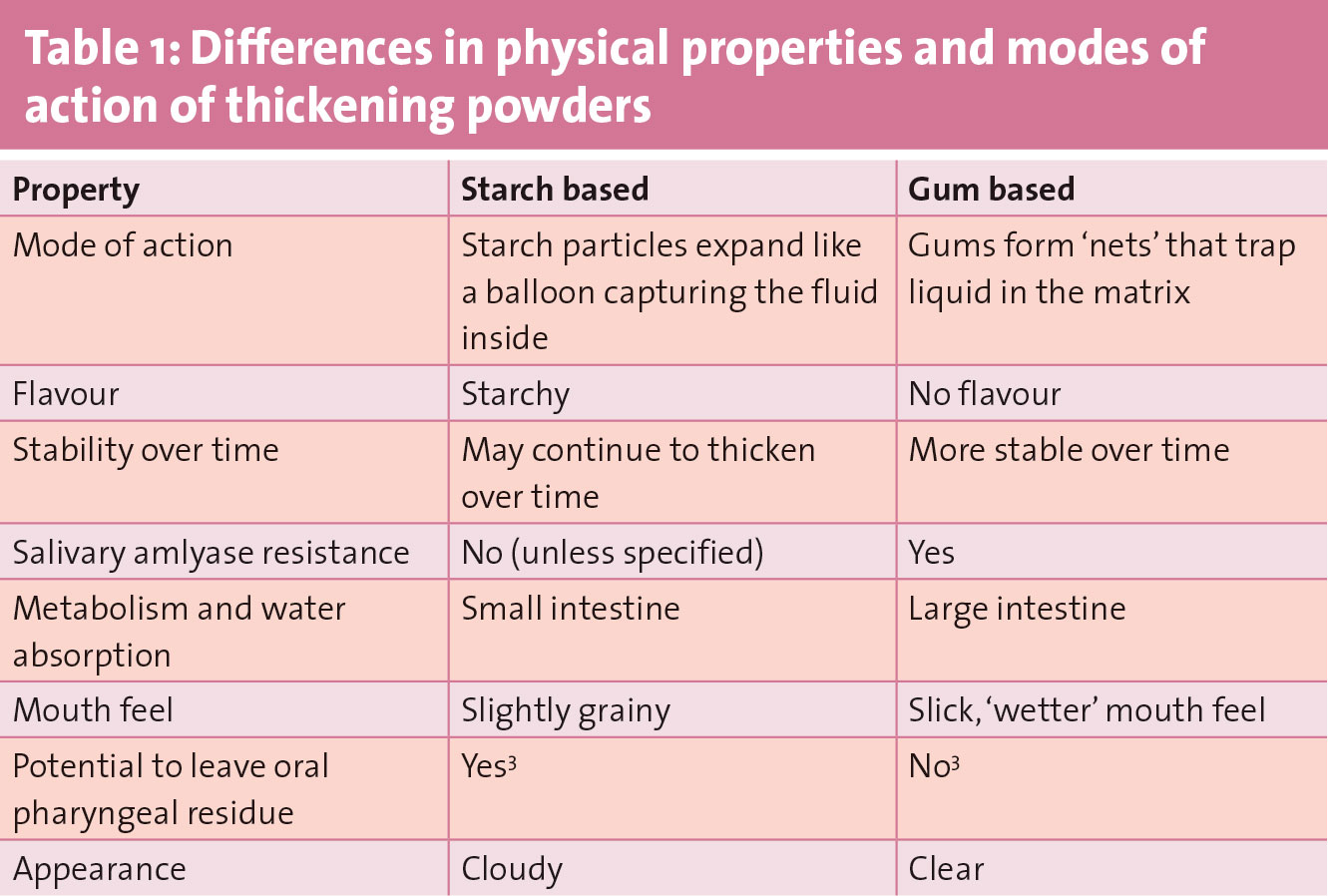
In Ireland, both gum-based thickeners and starch-based thickeners are available. Both types of thickening agents have different physical properties and modes of action (see Table 1). Thickeners are not interchangeable; scoop size and thickening guidelines differ according to the brand of thickening powder used, so it is important to follow the recommendation of the SLT and the manufacturer’s directions for use.
(click to enlarge)
The national descriptors also highlight and provide guidance on potentially high-risk foods, such as jelly and ice cream. At a local level, creating a list of practical alternatives for these high-risk foods is a simple strategy which can be immensely impactful, particularly for popular foods choices. For example, ice cream melts when we eat it and becomes as thin as free fluids in the mouth. Therefore this would not be suitable for people on thickened fluids.
Whipped cream flavoured with vanilla essence could be suggested as a safer alternative. Jelly particulates if not swallowed promptly and is therefore not suitable for people who require thickened fluids. However, offering the patient chilled fruit cordial dilute thickened to a grade 4 consistency is a safer alternative with just as much flavour.
Think about your own place of work – what foods do your patients miss most on a texture modified diet? What ‘safe swaps’ could you make? Do your catering and SLT colleagues have any suggestions?
A thirst for good hydration practice
Strategies to improve the hydration status of patients with dysphagia ultimately need to start with establishing if there is a problem in the first place. Auditing the measures taken to support patient hydration locally can help you identify good practices and areas for improvement. The following questions can be useful to ask both to the patient themselves and to nursing staff and carers:
• Are patients drinking the recommended equivalent of six to eight glasses of fluid every day? (unless advised otherwise by a healthcare professional)
• Are drinking aids available if appropriate?
• Are patients assisted with drinking if needed?
• Are drinks presented in an attractive manner?
• Are drinks always within reach of the patient?
• Are drinks always offered at an appropriate temperature, eg. hot tea, chilled juice?
•Are fluids always thickened correctly to the prescribed grade?
• How often is refresher training provided to staff and carers on correct thickening procedure?
Strategies to combat dehydration really depend on the answers to the questions above, and any changes you make should be pragmatic and realistic. Here are some ideas:
• Offer patients a variety of temperature
• Variations between sweet and savoury options may also support hydration; evidence indicates that this variation provides greater sensory stimulation, and may actually support a stronger swallow in healthy volunteers,4 however, the jury is still out as to whether this has any effect on patients with dysphagia5
• Carbonated drinks can offer a refreshing alternative, provided they are prepared and thickened correctly
• The use of ‘clear’ thickeners for clear drinks may improve adherence and hydration status of patients6
• For patients who also have impaired cognition or reduced awareness of thirst, eg. patients with dementia, reminders and prompts can be a useful strategy, eg. leave fruit drinks and milk in clear glasses, rather than cups or mugs, so the patient can see what is in them
• Enteral or parenteral hydration may be necessary for some patients when hydration requirements cannot be met by oral intake alone.
The dietitian may recommend oral nutritional supplements for malnourished patients with dysphagia if they fail to meet their nutritional needs through diet alone. These should be a safe consistency for the patients. They should not be used as a sole treatment and should always be given in combination with dietary advice and advice on food fortification.
It is difficult to thicken oral nutritional supplements to a safe, uniform consistency with the manual addition of a powder thickener,7 and in practice there is a wide variation and inconsistency in how drinks are thickened by patients, staff and carers.8,9 Pre-thickened oral nutritional supplements are available in a ready-to-use format at a guaranteed prescribed consistency. Alternatively, SLTs and dietitians can agree local guidelines for the manual addition of thickening powders to oral nutritional supplements.
Strategies to combat malnutrition
Early identification and management of malnutrition is essential. The Department of Health and Children10 and the Heath Information Quality Authority (HIQA)11 recommend that all patients should be screened for risk of malnutrition using a validated tool, eg. Malnutrition Universal Screening Tool.
Similar to tackling dehydration, every care centre has a different structure and caters for different patient needs, so auditing the current nutritional offering your dysphagia patients receive can help identify good nutritional practices and areas for improvement.
From a policy perspective, best practice guidance in the hospital setting stipulates that texture-modified menus providing at least 40% energy from fat should be available for patients with dysphagia.12 Guidance from HIQA11 for the community setting is less prescriptive but should be adhered to with the same diligence. Consider what is possible in your local setting, start with small changes and view it as an ongoing journey of service improvement.
Small portion sizes
The ‘little and often’ strategy is an obvious but effective strategy. People with dysphagia often take longer to eat and therefore their food is more likely to go cold. Serving half portions and keeping the remainder warm until the first portion has been eaten, or offering small frequent meals and snacks throughout the day, may increase patients’ nutritional intake more effectively than offering three larger meals.
Food fortification
Liquids of poor nutritional value, eg. water or gravy, are often added to foods during texture modification, resulting in nutrient dilution. This means that even if patients eat all of their meals, they are often reliant on food fortification and high-energy, high-protein snacks. Practical ideas for food fortification in dysphagia can be found in the members section of the INDI website (www.indi.ie/special-interest-groups/older-person-and-dementia.html)
Sense-ational food
Patients with dysphagia are often denied the variations in food textures – crumbly, crunchy, flaky, chewy – that make food so enjoyable. We eat with all of our senses, sight, touch, smell, taste and hearing, so every time we remove texture, we must replace this loss by adding extra detail in the appearance and flavour of the food.
Appearance
Good meal presentation is essential to nourishing patients with dysphagia, but is often challenging, particularly for textures B (minced and moist) and C (smooth purée). Food moulds are often seen as the gold standard for texture C as they most closely represent ‘real’ foods. They make meals more attractive, increase patient satisfaction, and can be adapted to many catering systems and menu cycles. However, do not be disheartened if food moulds cannot be used in your healthcare facility, creative presentation using piping, layering, scooping and rolling techniques can give attractive results and should not be underestimated, especially when techniques are used in combination by trained chefs.
Bright and colourful meals are more appealing; contrasting colours on a plate help people to decipher one food from another and can enhance the patient’s anticipation of flavour.
Flavour
Patients with dysphagia can get taste fatigue, particularly elderly patients as our perception of taste and smell significantly diminishes with age. In many cases, strong, sharp, sour or spicy tastes can help to stimulate the swallow, for example:
• Citrus drinks or desserts
• Spices like ginger through a rhubarb fool
• Jam or stewed fruit in porridge
• Herbs like basil in pasta sauce
• Seasoning with salt and pepper
• Vinegar
• Strongly flavoured sauces like tartar on fish or curry, chilli, or sweet and sour on meat
• Strong tasting foods like tuna.
Offering preferred flavours can also encourage intake, for example, a lot of dysphagic patients with dementia prefer sweet flavours. Foods like bread or biscuits, which require a soaking solution, should be soaked in flavoursome liquids like fruit juice, coffee or stock, rather than plain water. Close partnership with and buy-in from catering staff is essential here, as they bring a wealth of expertise to the table in terms of flavour pairings, meal presentation and practicalities of meal preparation.
Enhancing the mealtime experience
Positioning at mealtimes
Good positioning at mealtimes is essential to both the safety and comfort of the patient. This may include positioning the patient in an upright position, certain head positioning (if advised by the SLT), supporting the impaired side of the body if needed, and placing food in the stronger side of the mouth.
Visual field deficits should be noted and food should be within arms’ reach and visible to the patient. Modified cutlery and crockery may be recommended by the occupational therapist, eg. non-slip mats, cutlery with built up handles, cups that are weighted with handles, or shaped to give room for the nose.
Mealtime assistance
Effective mealtime assistance relies on two factors; successful identification of patients who need assistance,and sensitivity from those providing the assistance.
Patients requiring assistance at mealtimes can be identified by using discreet ‘flags’ such as red place mats or napkins. Good mealtime assistance often involves positioning of the person providing assistance at or below patient eye level, offering small mouthfuls, giving patients time to chew and swallow, and making positive comments about the meal.
For those providing assistance at mealtimes, a frequent impulse is to take over – to do ‘for’, rather than ‘with’. Independence can be supported by grading the support needed, ranging from showing and modelling, to cueing and guiding.
Mealtime environment
Space, traffic flow, lighting, sounds, temperature and décor are all factors that can affect one’s dining experience. A high traffic flow can cause unnecessary interruptions and can be disruptive to mealtimes. As a result, some hospitals and nursing homes have piloted fantastic initiatives like protected mealtimes. This initiative aims to create a calm mealtime atmosphere where the main focus is on serving appetising meals and providing patients with uninterrupted time to eat and enjoy a vital part of their treatment – their food.
This type of initiative involves a substantial amount of cross-functional partnership and stakeholder buy-in. It requires champions at all levels, including management and ward staff alike.
Implementation of initiatives like this is undoubtedly challenging and needs to be realistic and feasible. Consider the following: what wards could benefit most from the initiative? What particular mealtimes would work best? What are the local barriers to its implementation?
Breakfast and lunch clubs are another popular initiative because, not only do they help to promote independence and enhance social interaction, they also give patients a sense of normality at mealtimes.
Respecting patient autonomy
Food choice is a very personal thing and the individual likes and dislikes of patients should be respected. Knowing what and when a person likes to eat and drink makes it easier to ensure that they eat well. Some people eat better at certain times of the day; they may be less tired in the morning and able to eat a good breakfast, or they may prefer to have their main meal at midday. Be flexible and make the most of ‘good eating’ times.
Preservation of homelike rituals that the individual may have performed at home is a useful strategy that can work particularly well in nursing homes. For example, say grace or ask the resident to wash their hands before mealtime. If appropriate, something like helping to lay the table can remind a person that it is time to eat.
Ethnic, cultural and seasonal considerations are important too. Take a look at your menu cycle for texture modified diets; can you identify a mix of traditional meals as well as more ‘exotic’ alternatives (within reason)? Are seasonal options, eg. summer salads, autumnal stews or Christmas dinner offered at appropriate times?
Conclusion
All patients with dysphagia have the right to good nutritional care. They should have access to foods and fluids that are safe, appetising, nourishing and hydrating, and nutrition should be recognised as an integral part of their treatment.
Each healthcare centre is different, and nutritional management of dysphagia is certainly not ‘one size fits all’, especially within the busy reality of day-to-day healthcare. However, it is a dietitian’s responsibility, as a healthcare professional, to unlock the potential that their own place of work has – to lead by example with evidence-based policies and auditing of services, to work collaboratively with the multidisciplinary team and the patient themselves, and to advocate and search for ways in which dietitians can continue to improve the lives of people with dysphagia.
 (click to enlarge)
(click to enlarge)