Thromboembolic prophylaxis for hospitalised adult patients
An audit was conducted to assess the prescribing of appropriate thromboprophylaxis for hospitalised non-surgical patients
Dr Asiya Bello Suleiman, Clinical Medicine Lecturer; Medical Registrar, Connolly Hospital, Dublin and Dr Syed Irfan Shah, Medical Registrar in Respiratory Medicine, Connolly Hospital, Dublin
Venous thromboembolism (VTE), which includes deep vein thrombosis and pulmonary embolism (PE), is associated with significant morbidity and mortality.1 Hospitalised patients are 100 times more likely to have VTE than those in the community.2 Studies indicate that 5-10% of all in-hospital mortality is due to PE.1,3,4
It is perceived that VTE is a more common complication in surgical patients. However, post-mortem studies have revealed that nearly 70% of fatal PEs occurs in non-surgical patients.5 VTE prophylaxis is therefore very important in hospitalised patients and all medical patients should be assessed for VTE risk and prescribed accordingly. The aim of this audit is to ascertain if hospitalised non-surgical patients, 18 years and older, are prescribed appropriate thromboembolic prophylaxis.
Table 1. Bleeding risk factors(click to enlarge)
Figure 1. Thromboprophylaxis treatment(click to enlarge)
Figure 2. VTE risk factors(click to enlarge)
Figure 3. Contraindications to prophylaxis investigated(click to enlarge)
Table 2. Assessment of VTE risk(click to enlarge)
Table 3. Prophylaxis related to bleed risk(click to enlarge)
Method
In a tertiary Dublin teaching hospital, 30 in-patient charts and medication administration records were reviewed retrospectively. Data was collected regarding:
Demographics (age and sex)
Principal diagnosis
Expected length of stay of the patients
Risk factors
Contraindications to prophylaxis
VTE prophylaxis use, if any
The type, as well as the duration of the treatment.
The VTE risk factors and contraindications, and the type of prophylaxis, were as highlighted by the NICE guideline on VTE prophylaxis. It recommends that medical patients that are at risk of VTE should be offered prophylaxis.6 Patients considered at risk are:
Those who have had or are expected to have considerably reduced mobility for ≥ three days
Those who are expected to have continuing reduced mobility relative to their normal state and who have one or more risk factors. The risk factors collected were:
heart failure
respiratory failure/COPD
infection/sepsis
obesity
immobilised
cancer (previous or current)
surgery
previous DVT/PE
pregnancy
thrombophilia
varicose veins
hormone therapy
aged >75 years
dehydration
nephrotic syndrome.
All patients should be evaluated for any factors that increase the risk of bleeding (see Table 1) prior to commencement of medical VTE prophylaxis as these will influence the type of prophylaxis that can be safely used.6 We evaluated for contraindications to prophylaxis for the medical inpatients.
The different types of thromboprophylaxis evaluated were anti-thrombotic stockings and pharmacological therapy as recommended in the NICE guideline. The expected length of stay comprised ≤ 3, 4-7, 7-14 and > 14 days, with the duration of treatment of < 7, 7-14 and > 14 days.
Results
Some 60% of the patients in this audit were male and 43% were 75 years or older. Half of the patient group had an expected length of stay in hospital >14 days. Results showed that only 40% of patients were receiving thromboprophylaxis, despite most patients having at least one risk factor for VTE and only 10% with contraindications to prophylaxis:
Acute haemorrhagic stroke
Potentially bleeding lesion
Concurrent use of warfarin (see Figures 1, 2 and 3)
Some 13 of the 30 patients were on prophylaxis for more than 14 days.
The most commonly prescribed pharmacological drug was tinzaparin 3,500IU once daily subcutaneously with the second being enoxaparin 40mg once daily subcutaneously.
One patient was on enoxaparin 20mg due to severe renal impairment and one patient had anti-embolic stockings only (see Figure 1). Patients who were on antiplatelet (clopidogrel or aspirin) drugs for stroke/transient ischaemic attack or unstable angina/acute myocardial infarct were less likely to be on thromboprophylaxis even if they had VTE risk factors.
Conclusion
The results indicate that not all medical patients with increased risk of VTE are on prophylaxis. This was due to various factors; one concern was that there was no formal risk assessment model used to assess VTE risk for medical patients within 24 hours of hospitalisation. This would improve VTE prophylaxis for inpatients.
We propose that a validated risk assessment model (RAM), such as the Padua VTE Risk Assessment model, should be incorporated into the medication administration records to ensure appropriate VTE prophylaxis is offered and prescribed for medical inpatients.7
Points are allocated based on the presence of certain conditions with a RAM score of 4 or greater considered as high VTE risk (see Table 2). The decision to offer prophylaxis and the type to use is based on the RAM score and bleeding risk (see Table 3).
References
Qaseem A Chou R, Humphrey LL et al. Venous thromboembolism prophylaxis in hospitalized patients: A clinical practice guideline from the American College of Physicians. Ann Intern Med 2011; 155: 625-632
Heit JA, Melton LJ, Lohse CM et al. Incidence of venous thromboembolism in hospitalised patients vs community residents. Mayo Clin Proc 2001; 76: 1102-1110
Lindblad B, Sternby NH, Bergqvist D. Incidence of venous thromboembolism verified by necropsy over 30 years. BMJ 1991; 302: 709-11
Gibbs H, Fletcher J, Blombery P et al. Venous thromboembolism prophylaxis guideline implementation is improved by nurse directed feedback and audit. Thrombosis Journal 2011; 9:7
Nice clinical guideline 92. Venous thromboembolism: reducing the risk: Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital, January 2010
Jobin S, Kalliainen L, Adebayo L et al. Institute for Clinical Systems Improvement. Venous Thromboembolism Prophylaxis. http://bit.ly/VTEProphy1112. Updated November 2012
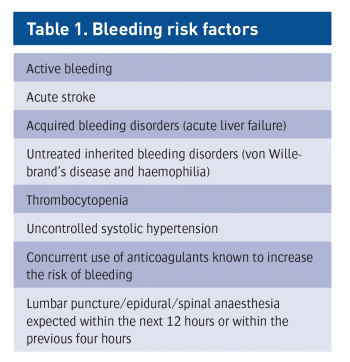 Table 1. Bleeding risk factors(click to enlarge)
Table 1. Bleeding risk factors(click to enlarge)




