There is an association between food allergy and other atopic conditions like allergic rhinitis, eczema, and asthma. Current thinking is that infants can benefit from early introduction of allergens in the diet
Dr Aisling Stafford, Paediatric Specialist Registrar, Our Lady's Children's Hospital, Crumlin and Dr Fiona Magee, GP and Author, ICGP Quick Reference Guide to Food Allergy in Children in Primary Care, Dublin
Food allergy is primarily a problem of infancy and early childhood. The prevalence of food allergy in children is approximately 4-6%.1,2,3 This condition is known to significantly impair quality of life in those living with food allergy and their families.4 The most common food allergens in Ireland are egg, peanut and milk. Irish data1 indicates that egg allergy occurs in 3% of children in Ireland, peanut allergy in 2%, and milk allergy in < 1%.
Many infants with food allergy will be allergic to more than one allergen, so significant overlap occurs. Allergy to both milk and egg are typically outgrown following infancy, as tolerance develops in the majority.5 However, peanut allergy persists as a lifelong allergy in the majority.6 At least 50% of those with peanut allergy will also have allergy to one or more tree nuts.
Atopy and food allergy
There is significant association between food allergy and other atopic conditions – eczema, asthma and allergic rhinitis. Individuals with one atopic condition will often have one or even several others. Eczema has a prevalence of approximately 20% in infants.7 The presence of eczema in infancy, especially if severe or early onset (before six months of age) is a risk factor for developing food allergy (and subsequently for other atopic conditions).
Eczema is a skin barrier defect that predisposes infants to the development of IgE-mediated food allergy, primarily by sensitisation via their altered skin barrier; ie. the eczema ‘causes’ the food allergy and not the other way around.
Introducing solids
Solid foods were traditionally introduced early in infancy (often from three months of age) in Irish households, typically based on advice from older generations in the absence of any cohesive public health guidance. In more recent decades, advice to start solids at around six months of age prevailed for a period, based primarily on WHO guidance which advises exclusive breastfeeding until six months.8
However, like most milestones in infancy, an age range rather than a single timepoint is often more appropriate. Current HSE weaning guidance9 suggests 17-26 weeks of age (approximately four to six months) as a suitable timeframe within which to introduce complementary solid foods, alongside either breastmilk or formula.
The best indicator of the right time is when the individual infant is showing signs of readiness for solid food– see www.hse.ieStarting your baby on solid foods (weaning) regarding these signs.
Allergy prevention
LEAP and EAT studies
For many years, the common food allergens, in particular peanut, were avoided in the weaning diet of infants, in the belief that avoiding them would reduce the risk of allergies. However, the opposite is now known to be true. The landmark LEAP study,10 published in 2015, found that early introduction of peanut from four months of age into the diet of infants with eczema or existing egg allergy reduced the risk of peanut allergy at age five by 81%, when compared to complete avoidance of peanut.
The subsequent EAT study11 looked at an exclusively breastfed population without specific risk factors for allergy. EAT demonstrated a significant reduction in relative risk of egg and other food allergies, again by early introduction of the allergens in the infants’ diets. The early allergen introduction was also found to be safe, and to have no negative impact on breastfeeding rates.
Tolerance versus allergy
The basis for allergy prevention is that in infancy and to some extent into early childhood, the immune system is still developing and somewhat malleable. During this period of malleability, before an allergy develops, it may be prevented, as tolerance to that allergen can be induced by early and regular exposure, ie. by eating the food. Conversely, during this time of developing immunity, new allergy can establish to a previously tolerated food, following a period of excluding that food. The timing or age range of opportunity to prevent allergy varies with different allergens. Once this window has closed, the chance to prevent allergy is lost – meaning time is of the essence.
While prevention is the goal, not all allergies can be prevented. Allergies to milk or egg are typically outgrown by early childhood, as tolerance develops. This can be aided by the use of ‘ladders’, ie. the Milk Ladder and IFAN Egg Ladder (see Table 1 and Figure 1 and 2). Peanut and tree nut allergies persist in the majority. However, resolution can occur in some.
Early feeding guidance
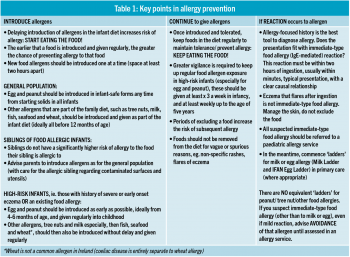
A better understanding of allergy prevention, especially that gleaned from the LEAP and EAT studies, revolutionised how food allergens are approached in the infant diet. Now the following advice should be given to parents and caregivers to optimise food allergy prevention:
• Start eating the food! Seize the ‘limited time only’ opportunity to prevent food allergy by introducing food allergens early into the infant diet12
• Continue to eat the food! Allergens need be given regularly until five years of age for some allergens (eg. peanut and tree nuts) to maintain tolerance.13
Do NOT avoid allergens in case of a possible reaction. Delayed introduction, or introduction that is not sustained (ie. a food is introduced but then followed by period of exclusion) increases the risk of allergy.
This preventative approach applies to the general population, who have a baseline risk of food allergy, but even more so to those at higher risk of food allergy (high-risk infants) ie. those with severe or early onset eczema or those with another food allergy.
The higher-risk population requires greater vigilance in terms of ongoing prevention, as outlined in Table 1.
(click to enlarge)
In recent years in Ireland, strides have been made as parents are introducing allergens earlier in the infant diet. However, the message about continuing to give the allergens needs to be made clearer to health professionals and caregivers. Below are listed the steps to take in trying to prevent cow’s milk, egg, peanut and tree nut allergies developing as per key points in Table 1.
Cow’s milk allergy prevention
Introduce
First exposure to cow’s milk depends on mode of feeding. Promote breastfeeding, but support whichever mode of feeding the mother chooses:
• If breastfed, first exposure is with dairy in solids or when formula is introduced (whichever is first). Exposure to cow’s milk protein via breastmilk is minimal (usually not significant)
• If formula-fed, exposure is with each formula feed. Aim to avoid unnecessary formula feeds in breastfed newborns,14 as this initial cow’s milk exposure followed by cow’s milk exclusion (exclusive breastfeeding) leads to increased risk of cow’s milk allergy when cow’s milk is later introduced.15
Dairy in solids include dried milk in many infant cereals, yoghurt, cheese, milk in sauces, lasagne etc.
Baked milk (in biscuits, muffins, etc) is tolerated in most milk-allergic infants, ie. most will not react to it.
Heat changes the nature of the milk protein rendering it much less allergenic. This is the basis for the Milk Ladder.
Continue
Keep cow’s milk in the diet where possible. Excluding cow’s milk on the basis of vague GI symptoms or eczema flares is not advised, and will increase subsequent risk of cow’s milk allergy.
Colic/reflux, etc. should be managed as for all infants, and eczema should be managed with appropriate skincare (adequate topical steroids and liberal emollients).
Cow’s milk should not be excluded unless genuine suspicion of cow’s milk allergy.
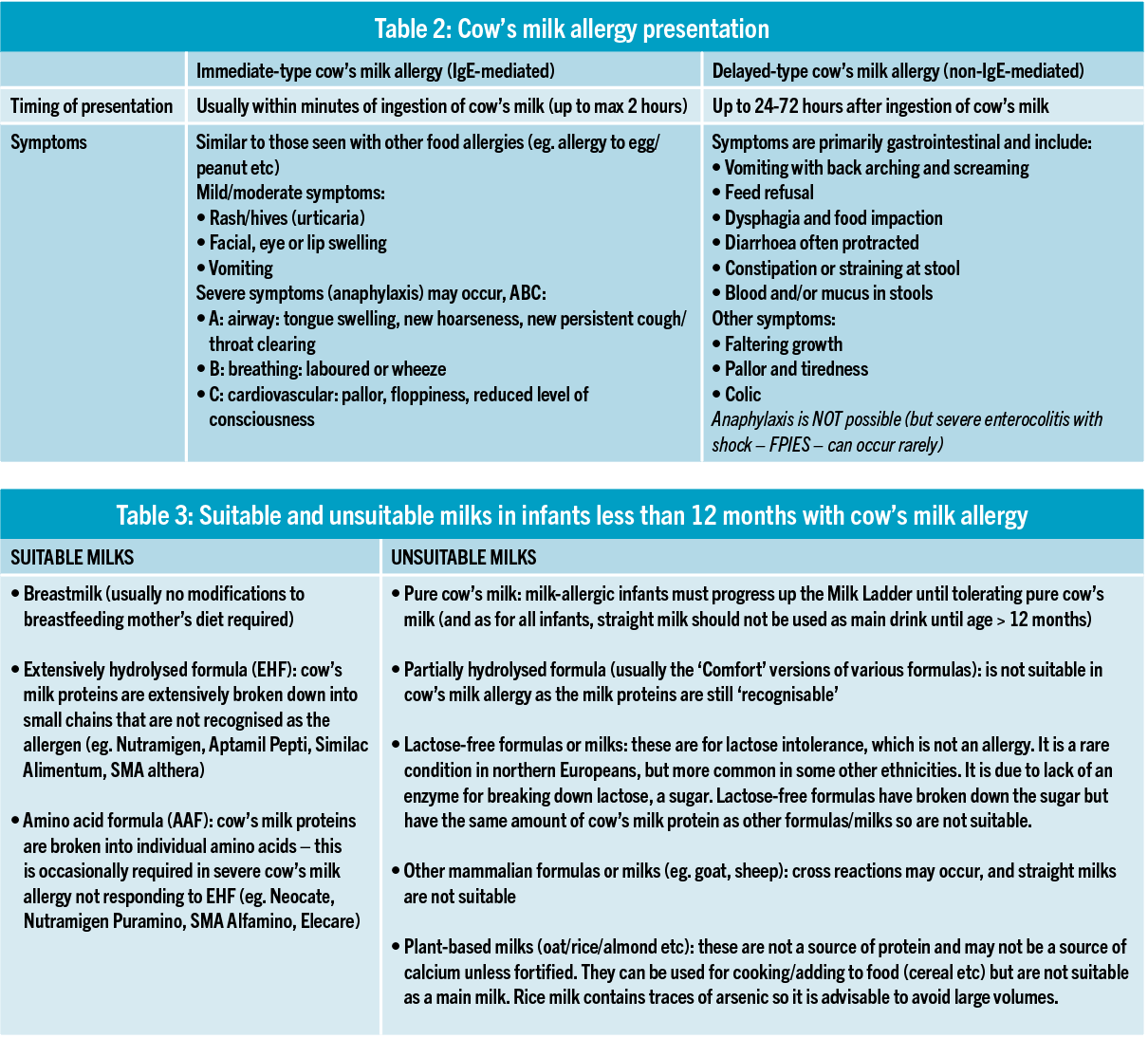
Even in cow’s milk allergy (immediate or delayed type (see Table 2 and Table 3), complete exclusion is not advised, as the Milk Ladder should be initiated and progressed.
(click to enlarge)
If reaction
Less than 1% of infants will have immediate-type cow’s milk allergy (reaction may be with first or subsequent exposure, often after a period of exclusion):
• No modifications to diet of breastfeeding mothers required
• If on formula, switch from regular (cow’s milk) formula to extensively hydrolysed formula (EHF)
• If infant is already on solids (or when infant subsequently starts solids), start infant on Milk Ladder without delay
• Do not use the Milk Ladder if anaphylaxis occurred to milk. In this case, complete avoidance is required and refer as urgent
• Refer all suspected immediate-type milk allergy to a paediatric allergy centre, and start Milk Ladder in primary care.
If delayed-type (non-IgE-mediated) cow’s milk allergy is suspected (delayed, primarily gastrointestinal symptoms, 24-72 hours post ingestion):
• A trial of excluding cow’s milk is required to make a diagnosis: two to four weeks of complete exclusion, followed by reintroduction. If symptoms resolve, then recur with reintroduction, diagnosis is confirmed (no other valid test is available)
• Once diagnosis is confirmed, then progress to longer period of ‘exclusion’ as below, but NOT complete exclusion, as the Milk Ladder should be initiated.
To exclude cow’s milk (both for trial period, and if diagnosis confirmed):
• In most cases, no modifications to diets of breastfeeding mothers required
• If on formula, switch from regular (cow’s milk) formula to extensively hydrolysed formula (EHF)
• If diagnosis confirmed, if infant is already on solids (or when infant subsequently starts solids), start infant on Milk Ladder without delay
• In most cases, manage non-IgE-mediated cow’s milk allergy in the community. There is no need to refer to allergy service (unless there is faltering growth or other concerns, in which case refer to general paediatrics)
• Community dietitian input is advised (where available) for ongoing milk exclusion, refer locally.
Parents can also be advised that the vast majority of cow’s milk allergy resolves following infancy/in early childhood.
Egg allergy
Introduce
For all infants, give egg early in the infant diet. For high-risk infants, aim to give egg at age four to six months, or as early as possible. The earlier egg is introduced and given regularly, the greater chance of preventing egg allergy.
Hardboiled mashed egg is a suitable form (it can be mashed with other foods). Raw egg should never be given to infants (salmonella risk, and most allergenic)
Baked egg (in cakes, biscuits, etc) is tolerated in most egg-allergic infants, ie. most will not react to it.
Heat changes the nature of the egg protein rendering it much less allergenic (especially baked in a matrix of wheat). This is the basis for the IFAN Egg Ladder.
Continue
Once egg has been introduced, if tolerated, it should be given regularly in the diet to maintain tolerance. In high-risk infants, greater vigilance is required to maintain tolerance/ prevent allergy, egg should be given three times a week.
If egg allergy presents (see below), initiate the IFAN Egg Ladder in the community.
If reaction
Egg allergy will occur in 2% of infants. Reaction is often with first exposure, and the risk of allergy is higher if first introduction is delayed until later in infancy, especially in infants with eczema.
Reactions are more common if lightly cooked egg (eg. scrambled) is given first, hence advice to start with well-cooked egg.
If reaction occurs and is convincing for egg allergy, advise avoidance of that form of egg, and initiate the IFAN Egg Ladder in primary care.
Do Not use the IFAN Egg Ladder if anaphylaxis occurred to egg (this is uncommon). Complete avoidance is required and refer as urgent.
Otherwise advise parents to progress up the IFAN Egg Ladder as tolerated and to continue to give the form of egg being tolerated at least three times a week.
If reactions occur when progressing up the ladder, manage with a non-sedating antihistamine, manage any eczema with appropriate steroid/emollient use, drop to the level of the ladder previously tolerated, continue this, and after several weeks reattempt, progressing up to the next rung.
Presence of egg allergy is a flag for increased risk of peanut allergy. In egg-allergic infants, advise as for high-risk infants above, ie. introduce peanut as soon as possible, and if tolerated keep peanut in the diet at least three times a week (followed by tree nuts).
Refer all suspected egg allergy to a paediatric allergy centre – meanwhile in primary care, start the IFAN Egg Ladder and advise introduction of peanut.
Peanut allergy
Introduce
For all infants, give peanut early in the infant diet, there is no reason to delay.
For high-risk infants, aim to give peanut at age four to six months, or as early as possible. The earlier peanut is introduced and given regularly, the greater the chance of preventing peanut allergy.
Give peanut in a safe/age-appropriate form; it should be smooth, as whole or chopped nuts pose a choking risk to infants and small children.
Give in a form without salt or sugar, eg. natural smooth peanut butter. It can be thinned with breastmilk or formula.
It should be spooned into the mouth, rather than allowing food play, to avoid local irritation or sensitisation via the skin.
Continue
Once peanut has been introduced, if tolerated, it should be given regularly in the diet to maintain tolerance.
In high-risk infants, greater vigilance is required to maintain tolerance/prevent allergy. Peanut should be given at least three times a week as one level teaspoon (infant-safe form).
In infants where reaction occurred (see below), peanut should be completely avoided (pending assessment in an allergy centre).
If reaction
Peanut allergy will occur in 2% of infants. In high-risk infants (severe/early onset eczema or egg allergy) the risk is much higher, but early introduction of peanut reduces this risk significantly.
If reaction to peanut occurs, and history/timing fits with peanut allergy, advise complete avoidance of peanut (there is no equivalent ‘ladder’ for peanut).
First reactions to peanut are often mild, regardless of how mild, the advice is complete avoidance, and no attempts at repeat exposure should be made in the community.
Other nuts (tree nuts) being tolerated in the diet should continue to be given, and other food allergens should continue to be introduced.
Refer all suspected peanut allergy to a paediatric allergy centre, and advise strict avoidance of peanut.
Tree nut allergy
Introduce
Tree nuts refer to all the nuts other than peanut (peanut is really a legume). These include Brazil, walnut, pecan, hazelnut, cashew, pistachio and almond (pine nuts are not nuts, they are seeds).
Following introduction of egg and peanut, parents can be advised to move on to introducing the tree nuts one by one.
In high-risk infants, it is preferable to introduce the various tree nuts sooner in the infant diet.
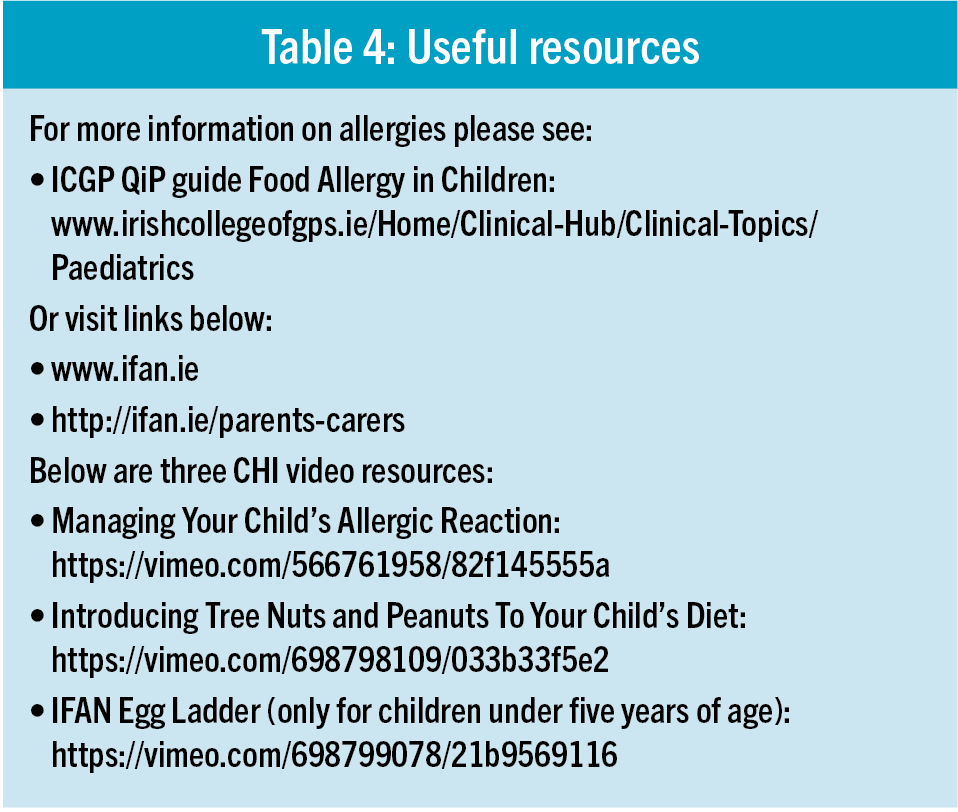
Children’s Health Ireland has very useful videos about introducing and giving tree nuts, see Table 4.
(click to enlarge)
Continue
Any tree nuts once introduced and tolerated should ideally be given regularly in the diet to maintain tolerance.
More vigilance is required in high-risk infants, including those with an existing allergy to egg/peanut/another tree nut. The tree nuts that they tolerate should be given regularly (ideally three times a week) to maintain tolerance to those tree nuts, and prevent allergy developing.
If reaction
If reaction occurs to any tree nut, the management is exactly as for peanut, above:
• Advise strict avoidance of the tree nut to which the reaction occurred
• Refer to a paediatric allergy centre.
Summary
Delayed introduction, or introduction followed by avoidance of food allergens in the infant diet, increases the chance of allergy.
Conversely, early introduction of allergens followed by regular exposure (eating the food) reduces allergy.
• Start eating the food!
• Keep eating the food!
Infants with higher risk of allergy, particularly those with eczema or an existing food allergy, can benefit most from early introduction – especially egg and peanut.
However, as the general population has a baseline risk of food allergy, all infants stand to benefit from being introduced to allergens in the diet early.
While the earlier the better in terms of allergy prevention, this must be balanced with the timeframe it is considered appropriate to introduce solids (four to six months), and with an individual infant’s readiness for solids.
References
Kelleher MM et al. Skin barrier impairment at birth predicts food allergy at 2 years of age. J.Allergy Clin.Immunol. 2016 Apr; 137(4):1111-1116.e8
Grabenhenrich L et al. Frequency of food allergy in school-aged children in eight European countries—The EuroPrevall-iFAAM birth cohort. Allergy (Copenhagen). 2020; 75(9): 2294-2308
Venter C et al. Prevalence and Cumulative Incidence of Food Hypersensitivity in the First 3 Years of Life.” Allergy (Copenhagen). 2008; 63(3): 354-359
Cummings AJ et al. Psychosocial Impact of Food Allergy and Food Hypersensitivity in Children, Adolescents and Their Families: a Review. Allergy (Copenhagen). 2010; 65(8): 933-945
Savage J et al. The Natural History of Food Allergy. J.Allergy Clin.Immunol.Pract. 2016; 4(2): 196-203
Skolnick HS et al. The natural history of peanut allergy. J.Allergy Clin.Immunol. 2001; 107(2): 367-374
Williams H et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the International Study of Asthma and Allergies in Childhood. J Allergy Clin Immunol 1999; 103: 125-38
Du Toit G et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N.Engl.J.Med. 2015; 372(9): 803-813
Perkin MR et al. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J.Allergy Clin.Immunol. 2016; 137(5): 1477-1486
Abrams E et al. Early introduction is not enough: CSACI statement on the importance of ongoing regular ingestion as a means of food allergy prevention. Allergy, asthma, and clinical immunology, 2023; 19: 63
Halken S et al. European Academy of Allergy and Clinical Immunology Food Allergy and Anaphylaxis Guidelines Group. EAACI guideline: Preventing the development of food allergy in infants and young children (2020 update). Pediatr Allergy Immunol. 2021; 32: 843-858
Høst et al. A Prospective Study of Cow’s Milk Allergy in Exclusively Breast-Fed Infants. Acta Paediatrica. 1988; 77(5): 663-70
 (click to enlarge)
(click to enlarge)