Pattern of referrals to an Irish psychiatric intensive care unit
This study aimed to identify referral patterns to an Irish psychiatric intensive care unit over a two-year period, and whether there has been an increase in referral numbers
Dr Shaeraine Raaj, Registrar Psychiatrist, RCSI Training Scheme, Dublin, Dr Sujesha Navanathan, Psychiatry SHO, Phoenix Care Centre, Dublin, Dr Anisha Bhagawan, Registrar Psychiatrist, Phoenix Care Centre, Dublin, Dr Firdous Murad, Registrar Psychiatrist, Phoenix Care Centre, Dublin, Dr Ernest Nwarie, Registrar Psychiatrist, Phoenix Care Centre, Dublin, Dr Pauline Twomey, Consultant Psychiatrist, Phoenix Care Centre, Dublin and Dr Roy Browne, Consultant Psychiatrist and Clinical Director, Psychiatry Intensive Care Unit, Phoenix Care Centre, Dublin
The Phoenix Care Centre, which includes the only psychiatric intensive care unit in Ireland, is a state-of-the-art, purpose-built mental health facility. It is a 54-bed mental health facility split into four separate clinical areas – two psychiatric intensive care units and two rehabilitation units.1 The centre provides a tertiary service for patients who require an intensive care setting for the treatment of acute episodes of their mental illness within a locked therapeutic environment. It covers a population of 1.8 million within the catchment areas of Dublin, Wicklow and the northeast region.
Over the past 20 years a small group of patients has shown to be difficult to manage in a general hospital setting. Risks leading to referral include significant aggression, risk of assault, actual assault and absconding. Those with a symptom pattern indicating a level of risk requiring higher level of observation and management are admitted to the Phoenix Care Centre.
There have been studies of violent incidents in psychiatry units in the past.2,3,4,5 In this study, the authors hypothesised that psychiatry intensive care units have experienced an increase in referral numbers, and that referrals are now more likely to be concerned with risks of assault and/or absconding. The authors also hypothesised that female patients would have a shorter mean length of stay.
Aim
The aim of this study was to identify the referral pattern to a psychiatric intensive care unit in Ireland and to demonstrate the diagnosis, mean length of stay, gender and the indication for referrals over a two years period.
Methodology
The Phoenix Care Centre requires all patients to be referred by a consultant psychiatrist. It has a detailed referral form that can only be completed by the referring consultant psychiatrist.
A retrospective chart study was carried out on admissions in the preceding two years. All patients admitted between January 2014 and January 2016 to the psychiatric ICU were included in the study (n = 67). Information concerning patients’ characteristics was obtained at the time of admission. This included gender, age, indication for referral and the ICD 10 diagnosis.6 Original referrals were retrieved and anonymised before data were extracted. Referrals were compared with regard to the referring gender, indication for referral, age and whether psychotropic medication was already being prescribed. The dates were obscured to provide some blinding to year of referral.
Exclusion criteria included suicide being the main indication without an axis 1 co-morbidity. The referrals were divided between the authors and any uncertainties were discussed and agreed between the authors.
Three initial meetings of the working group took place in order to review the scientific literature in relation to psychiatric intensive care units. All data returned was coded and analysed for descriptive statistics using Microsoft Excel.
Results
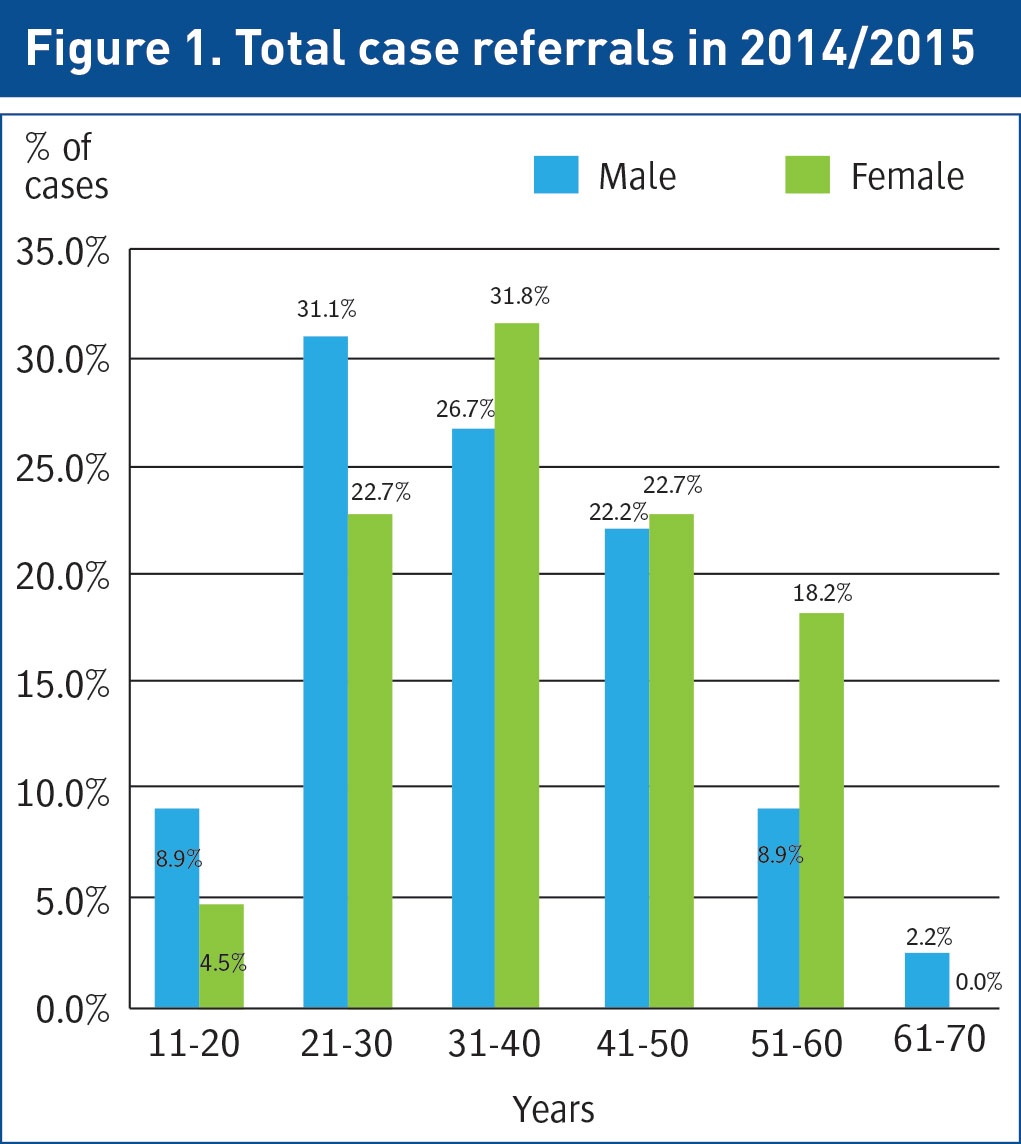
The result of this research indicates that there was a higher rate of male referrals to the Phoenix Care Centre (see Figure 1) (males: n = 45 and females: n = 22).
The incidence for females was higher as they reached the fourth decade of their life (aged 31-40 years) compared to males who had a higher incidence in the third decade of life (aged 21-30 years). Both male and female referrals gradually decrease in incidence as they age (see Figure 1).
(click to enlarge)
Discussion
This study indicates that there was a dramatic increase in referrals to the Phoenix Care Centre in the year 2015 compared to 2014. The results show a higher rate of referrals of males than of females to the centre (males: n = 45 and females: n = 22).
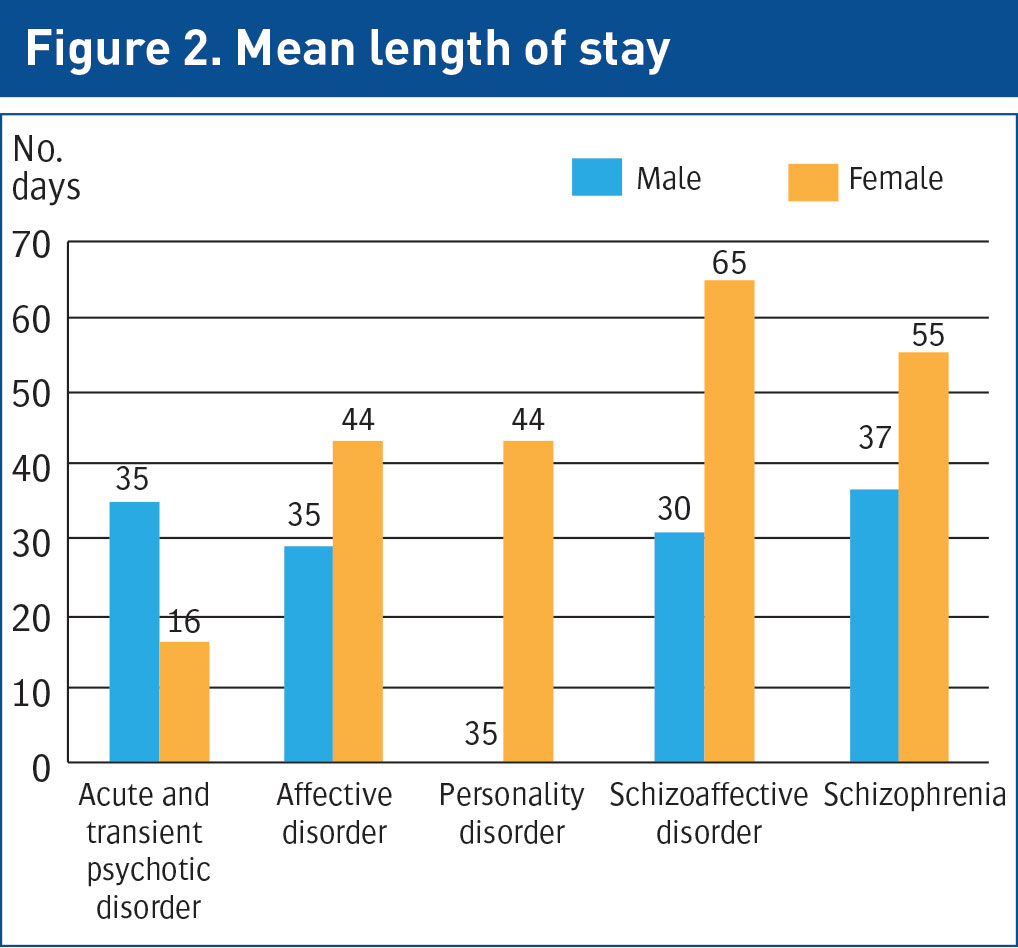
The authors had hypothesised that females have a shorter mean length of stay, however the study shows evidence of females having a longer mean length of stay (see Figure 2).
(click to enlarge)
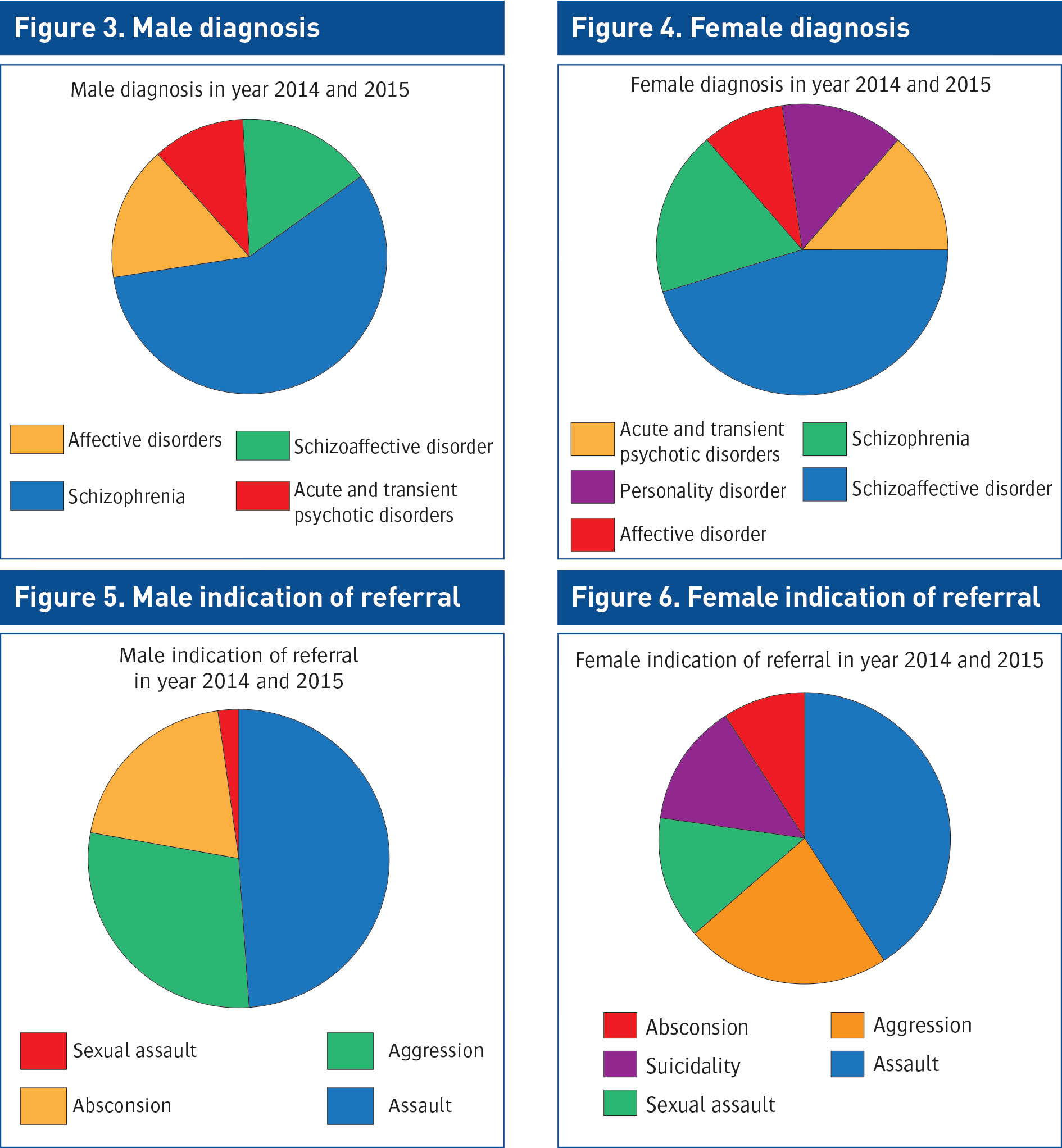
As shown in Figures 3 & 4, males referred most frequently with a diagnosis of schizophrenia disorder (57.8%) compared to females with a most frequent diagnosis of schizoaffective disorder (45.5%). Personality disorder and affective disorder were the least referred diagnoses for both female and males.
Physical assault was the most significant indication for referral in both males (48.9%) and females (40.9%).Sexual assault and those with a history of absconding were less common (see Figures 5 & 6).
The mean stay for females with a diagnosis of schizo-affective disorder (n = 65 days) was higher compared to other stated disorders. Comparatively, males diagnosed with schizophrenia disorder had a shorter period of admission (n = 37 days ) as they responded quicker to psychotropic medication (see Figure 2).
A weakness with this study is that concerns expressed in the referral letters may not have reflected what was actually found on assessment. Patients who were stated to have an allergy to a second generation antipsychotic were found to have a better response to the particular second generation antipsychotic rather than what was indicated to the referral.
The pharmacokinetics and pharmacodynamics of antipsychotic drugs differ in women and men. Drug concentrations are dependent on the volume of distribution (Vd) and clearance (Cl). The parameters are influenced by gender-specific factors such as body build, diet, smoking status, concurrent medication, exercise, substance use and hormonal transition.7
Future research is needed to strengthen these findings and explore types and degree of assault leading to psychiatry ICU. We hope to explore course of inpatient admission; seclusion use; restraint use and to acquire data for the year 2016.
(click to enlarge)
Limitations of the study
Notable limitations persist with the current study. Firstly, it is limited by the small sample size. Secondly, the current study does not have a control group and therefore there were no comparisons made to the findings. Furthermore, there was difficulty obtaining patient data as the method of compilation was not used through the electronic patient record system (EPR).
Conclusion
The authors concluded that the Phoenix Care Centre solely accepts patients who exhibit actual assaults in the form of physical or sexual, aggression and risk of absconding on the background of psychosis. The duration of stay as an inpatient in the centre depends on the patient’s response to antipsychotic therapy, which is generally within six weeks.
Acknowledgement
The authors wish to acknowledge the assistance of the Phoenix Care Centre and thank both Ray Farrelay, Kevin Tracey and Anne Marie in particular for their help.
References
Health Service Executive. Phoenix care centre. http://www.hse.ie/eng/services/list/1/LHO/DublinNW/Mental_Health_Services/Phoenix_Care_Centre/
Fottrell E. A study of violent behaviour among patients in psychiatry hospitals. British Journal of Psychiatry 1980; 136,216-221
Tardiff K, Sweillam A. Assaultive behavior among chronic inpatients. Am J Psychiatry 1982; 139: 212-215
Pearson M, Wilmot E, Padi M. A study of violent behaviour among in-patient in a psychiatry hospital. The British Journal of Psychiatry Aug 1986; 149 (2): 232-235
James DV, Fineberg NA, Shah AK, Priest RG. An increase in violence on an acute psychiatry ward. A study of associated factors. The British Journal of Psychiatry Jun 1990; 156 (6): 846-852
World Health Organization Geneva. The ICD 10 Classification of mental and behavior disorder 1992. Clinical descriptions and diagnostic guidelines.
Seeman MV. Gender difference in the prescribing of antipsychotic drugs. American Journal of Psychiatry Aug 2004; 161(8):1324-1333. https://ils.unc.edu/bmh/neoref/nrschizophrenia/jsp/review/tmp/198.pdf
Further reading
• Anderson GD. Int Rev Neurobiol 2008. Gender difference in pharmacological response. https://www.ncbi.nlm.nih.gov/m/pubmed/18929073/
• Psychiatric Intensive Care Units: a Literature Review.- Len Bowers, City University http://www.kcl.ac.uk/ioppn/depts/hspr/research/ciemh/mhn/projects/litreview/LitRevPICU.pdf
• Brown S, Bass N. The psychiatric intensive care unit: patient characteristics, treatment and outcome. J Mental Health 2004; 13(6): 601-9. Google Scholar
• Cooper SJ, Brown FWA, McLean KJ, King DJ. Aggressive behaviour in a psychiatric observation ward. Acta Psychiatrica Scandinavica 1983; 68: 386-93. Google Scholar Medline
• Psychiatric intensive care units: a literature re https://www.ncbi.nlm.nih.gov/pubmed/18309759view.
• Violent incidents in a Psychiatric Intensive Care Unit- Zuzana Walker, University College London https://www.researchgate.net/publication/15246229_Violent_incidents_in_a_Psychiatric_Intensive_Care_Unit
• Dernovsek M, Novak-Grubic V, Tavcar R, Zmitek A. Psychiatric intensive care units: comment. Australian and New Zealand J Psychiatr 2003; 37(1): 110. Google Scholar Medline
 (click to enlarge)
(click to enlarge)