CANCER
Testicular germ cell cancer: a risk-adapted approach
When treating germ cell tumours, an individualised approach with a collaborative treatment decision-making process is optimal
October 1, 2015
-
Germ cell tumours are the most common malignancy in men between the ages of 15 and 35. They most frequently occur in the gonads or less commonly in the retroperitoneum or mediastinum. The objective in all cases is cure, regardless of the extent of the disease, and survival rates in Ireland are 93.6%.1 There are 176 new cases of testicular cancer diagnosed per year in Ireland and the incidence rate is increasing.1 Testicular cancer risk is increased in cryptorchidism, spermatic or testicular dysgenesis, positive family history, HIV and Kleinfelter syndrome.2,3 In the case of male babies with undescended testes, orchidopexy before puberty reduces the risk of a germ cell tumour.4 Germ cell tumours are derived from premeiotic germ cells which undergo malignant transformation. The majority of tumours are associated with an abnormality on chromosome 12. Most germ cell tumours are hyperdiploid, suggesting that endoreduplication is a necessary early step in malignant transformation.5
Pathology
Germ cell tumours are classified histologically into seminomas and non-seminomas. Seminomas account for 50% of all germ cell tumours, are exquisitely sensitive to chemotherapy and radiation, and have a normal AFP (alpha-fetoprotein). Non-seminomas can contain multiple cell types and are associated with a high AFP and a more aggressive biology. The presence of any component of non-seminomatous tissue with seminoma is treated as a non-seminomatous germ cell tumour. Most non-seminomas show mixed histology and can include: embryonal carcinoma, teratoma, choriocarcinoma, yolk sac or endodermal-sinus tumours.
Diagnosis
The majority of patients present with a diffuse testicular mass which may be hard and painful. Absence of pain is highly suggestive of malignancy. Most patients are initially treated with antibiotics for suspected epididymo-orchitis. If symptoms do not resolve within two weeks a testicular ultrasound is indicated. A delay in diagnosis is associated with a higher stage of disease at presentation. Evidence of a testicular tumour on ultrasound results in a radical inguinal orchiectomy. Testicular biopsies are contraindicated to avoid disturbance of the vascular and lymphatic drainage.6 Levels of alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG) and lactate dehydrogenase (LDH) should be checked. Serum tumour markers are beneficial for prognostication and treatment planning, as well as for monitoring outcomes and relapse.
Patterns of spread
The primary lymphatic drainage for testicular germ cell tumours is to the retroperitoneal lymph nodes. The right testicular artery originates form the aorta and the right testicular vein drains into the inferior vena cava. The left testicular artery originates near the left renal artery and the left testicular vein drains to the left renal vein. Right-sided tumours spread to the interaortocaval lymph nodes and left-sided tumours spread to the para-aortic lymph nodes below the left renal artery and vein. Additional metastatic sites include the retrocrural, mediastinal and supraclavicular lymph nodes, the lungs, liver, central nervous system and bone.
Staging
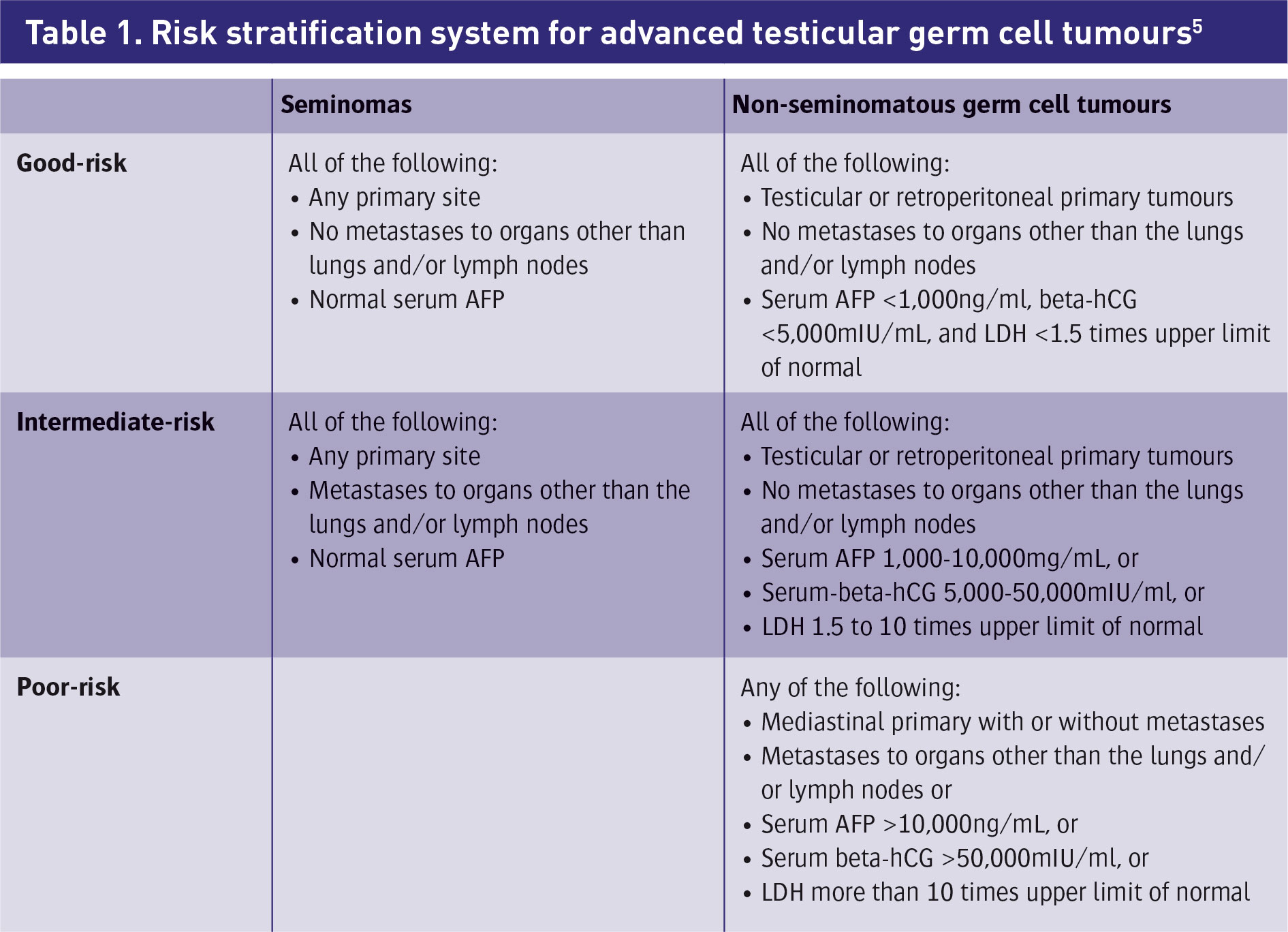
Staging should include LDH, AFP, hCG, chest x-ray, CT thorax/abdomen/pelvis (CTTAP) scan and sperm banking should be offered to all men diagnosed with testicular cancer prior to chemotherapy to preserve fertility where possible. Staging for germ cell tumours is based on the TNM classification developed by the American Joint Committee on Cancer.7 Adverse features include a mediastinal primary site, degree of elevation of AFP, hCG, LDH and the presence of non-pulmonary visceral metastases. Patients are risk stratified into good-risk, intermediate-risk and poor-risk using a validated prognostic model that uses histology, sites of disease and serum tumour markers to predict progression free survival and overall survival.8 It is an important tool to guide treatment selection. In relation to risk stratifications, 60% of germ cell tumours are good-risk and have a five-year survival rate of 91%, 26% are intermediate with a five-year survival rate of 79%, and 14% are poor-risk with a five-year survival rate of 48%.8
Seminoma
Some 70% of patients present with stage 1 seminoma. After radical orchiectomy, standard treatment options include surveillance, adjuvant radiation to para-aortic lymph nodes or single agent carboplatin. Surveillance is the preferred treatment strategy with a risk of relapse of 15-20% at five years with the majority of relapses occurring in the infradiaphragmatic lymphnodes.9.10,11 Overall, survival approaches 100% regardless of management strategy employed.12,13,14 Radiation is associated with long-term cardiac toxicities and secondary malignancies, and is contraindicated in inflammatory bowel disease and horseshoe kidneys. Carboplatin chemotherapy (two cycles) can also be considered; it is non-inferior to radiation and has similar relapse rates.15,16 The National Comprehensive Cancer Network (NCCN) recommends a surveillance schedule consisting of physical exam, tumour markers and CTPA every three to four months for the first two years, and every six to 12 months annually thereafter.17
The standard of care for patients with stage 2 seminoma confined to the retroperitoneum with three or fewer lymphnodes involved is radiation to the para-aortic and ipsilateral lymphnodes.18 In patients with bulky disease the risk of relapse is higher19 and chemotherapy with BEP (bleomycin/etoposide/cisplatinum) for three cycles or EP for four cycles is preferred. Residual masses <3cm in diameter can be observed.11 Masses >3cm should be considered for surgical resection.11
Advanced seminoma
Overall, 15-20% of patients present with advanced seminoma. Patients with retroperitoneal masses >5cm, supradiaphragmatic lymphadenopathy, visceral disease, bulky retroperitoneal tumours, tumour-related back pain and mediastinal extra-gonadal presentations are treated with primary chemotherapy. Of these patients with advanced seminoma, 90% are classified as good-risk with an 86% five-year survival.6
Post-chemotherapy masses may represent fibrosis and can be managed by observation or surgical resection. PET-CT should be performed in patients with residual masses >3cm; residual FDG uptake indicates the need for surgical resection.
Non-seminomatous germ cell tumours – stage 1
Some 30-40% of patients present with stage 1 disease. Options for management include surveillance, retroperitoneal lymphnode dissection or primary chemotherapy. Surveillance is the preferred option for compliant patients with stage 1a. This includes tumours with no vascular or lymphatic invasion or invasion into the tunica vaginalis, spermatic cord or scrotum. Of these patients, 20% will have recurrent disease, with the majority occurring in the retroperitoneum.21 Most recurrences take place within two years of diagnosis and require treatment with chemotherapy.21 Follow up must be meticulous with one to two monthly history, physical exam, chest x-ray and tumour markers, as well as abdominal CT every four to six months. Late recurrences can occur, however cure rates are as high as 98-99%. Patients with stage 1 with high-risk features for recurrence can be treated with nerve-sparing retroperitoneal lymphnode dissection.
Chemotherapy may have a role as low recurrence rates have been seen in patients with clinical stage 1 non-seminonatous testicular cancer, treated with one or two cycles of bleomycin, etoposide, cisplatin.22,23 Concerns remain however, regarding the possibility of unnecessary exposure to chemotherapy and the associated long-term toxicities.
NSGCT stage 2 disease
N1 disease (lymph node mass ≤2cm) has a 20% risk of relapse, and as such surveillance is the preferred option in this group. Patients with N2 disease (lymph node mass 2-5cm) should be treated with surgery and two cycles of adjuvant chemotherapy. Residual masses >3cm should undergo PET imaging and surgical considerations as they are at high risk of containing persistent germ cell tumour.24
NSGCT stage 3 disease
Cisplatin-based chemotherapy combined with surgical resection of residual disease will cure 70-80% of patients with metastatic disease.25 For those with high-risk disease the goal is cure, whereas those with lower-risk disease the goal is to minimise toxicities without compromising cure.25
Risk stratification of advanced germ cell tumours
Treatment depends on the IGCCCG risk classification score8 (see Table 1).
Good-risk
In total, 60% of NSGCT have good-risk features. These include stage 2 or 3 disease with testicular or retroperitoneal primary tumours, no visceral metastases. More than 90% will be cured with combination chemotherapy using cisplatin and etoposide with or without bleomycin.26,27,28,29,30 A trial from the Genito-Urinary Group of the French Federation of Cancer Centres demonstrated that four cycles of etoposide plus cisplatin were equivalent to three cycles of BEP in terms of overall survival. Elimination of bleomycin does not compromise cure as long as the additional cycle of cisplatin and etoposide is given, and the associated Raynaud’s phenomenon and pulmonary toxicity can be avoided.30,31 Carboplatin has less toxicity, however it cannot be substituted for cisplatin and it is associated with significantly inferior event-free and relapse-free survival rates.32
Intermediate-risk
This includes patients with NSGCT with intermediate risk tumour markers as well as patients with seminoma who have primary mediastinal seminoma or non-pulmonary visceral metastasis.
Poor-risk
Poor-risk disease includes patients with non-seminomatous germ cell tumours with non-pulmonary visceral metastasis, poor risk tumour markers or primary mediastinal site. These patients have a five-year survival of approximately 50%.6 The standard of care is four cycles of BEP chemotherapy.
Salvage therapy for germ cell tumours
Overall, 20-30% of people with advanced germ cell tumours fail to achieve a durable response to chemotherapy. This is associated with a poor prognosis. Late relapse beyond two years is associated with a high degree of resistance to standard salvage chemotherapy.30
The combination of paclitaxel, ifosfamide and cisplatin (TIP) was evaluated as second-line therapy for patients with favourable features, including prior complete response to first-line chemotherapy.33
Four cycles of TIP as second-line therapy resulted in 70% complete response rate with a 63% durable complete response and a two-year progression free survival of 65%.TIP followed by surgery may be effective in patient with late relapsing disease A phase I trial using cisplatin and epirubicin has also shown activity in the salvage setting.34 Clinical trials should be considered for patients requiring salvage therapy.
High-dose chemotherapy with peripheral stem cell rescue for germ cell tumours
Patients who do not have an initial complete response to induction chemotherapy or who relapse after first-line salvage chemotherapy should be considered for high-dose chemotherapy with peripheral stem cell rescue. This involves chemotherapy followed by peripheral blood stem cell transplantation or autologous bone marrow transplantation. Once haematopoietic reconstitutions occur, a repeat course of chemotherapy can be given followed by surgical resection of residual disease in selected patients.35
Overall, survival using this method is 52%.35 Treatment outcomes are significantly worse in patients with primary mediastinal tumours treated with high-dose chemotherapy and stem cell rescue.36 Patients with brain involvement have a poor prognosis.38 Treatment options include resection where feasible, whole brain radiation and cisplatin based chemotherapy.38,39
Surgery after chemotherapy for NSGCT
Patients with residual disease post-chemotherapy with normal serum tumour markers should be offered surgery. It is the mainstay of treatment. It improves outcomes and decreases the risk of late recurrence.35,40 A total of 40% of residual masses will consist of mature teratoma; the minority of which will undergo malignancy transformation31 and 5% will contain germ cell tumour and therefore require two further cycles of chemotherapy.41
Survivorship and late effects
There is increased cardiovascular disease in patients treated for testicular cancer. This is due to chemotherapy-induced endothelial damage, mediastinal radiation, metabolic syndrome and gonadal dysfunction.41 Prior radiotherapy increases the risk of secondary malignancies.42 Long-term side effects include ototoxicity, neurotoxicity, pulmonary disease and renal impairment.43 Psychological support should also be available.
A recent study in the Journal of Clinical Oncology recommended that patients with germ cell tumour who survive after more than one line of treatment for disseminated disease should have lifelong follow-up due to the increased risk of late toxicity and death as a result of secondary causes.44
In conclusion, testicular germ cell tumours represent a spectrum of disease and require a risk-adapted approach. As the prognosis is excellent for the majority of cases, clinicians must be judicious in their treatment choices, by weighing up risk of recurrence, adherence to follow-up schedules and long-term toxicities.
Ultimately, an individualised approach with a collaborative, informed, treatment decision making process, is optimal.
 (click to enlarge)
(click to enlarge)