Schizophrenia is a disorder characterised by abnormal thought processes, along with disturbances in behaviour, mood and perception of reality. It usually presents during adolescence or young adulthood (16-30 years) with men reaching a peak vulnerability somewhat earlier (age 16-25) than females (age 25-30), and having a somewhat poorer prognosis. Presentation at this age is associated with significant educational and occupational as well as social sequelae. Recognition of the signs and symptoms of schizophrenia is key to putting together early treatment pathways and reducing long term morbidity and mortality.
Prevalence
The prevalence of schizophrenia (ie. the number of cases in a population at any one time point) approaches 1% internationally and up to 3.48% if all other psychotic disorders are included.1 The incidence (the number of new cases annually) is about 1.5 per 10,000 people. To put that into context, an estimated 26 million people worldwide are currently living with schizophrenia, with about 3,900 people in Ireland, according to Shine, a mental health support organisation. Morbidity and mortality are much higher than expected, with the average life expectancy among those diagnosed with schizophrenia being 12-15 years less than the general population. This is reflected by a high suicide rate (5-10%) as well as increased incidence of cardiovascular disease, especially among those on long-term antipsychotic medications.2
Clinical presentation
Schizophrenia can be considered under the umbrella term of psychotic disorders.3 Other psychoses include:
Affective psychoses (bipolar disorder/major depressive disorder with psychotic features)
Substance induced psychotic disorder
Psychosis due to general medical condition.
These disorders can be distinguished from each other by analysing duration, dysfunction, associated substance use and presence of depression or mania. Schizophrenia can be identified by its long duration, bizarre delusions, negative symptoms and few affective symptoms.
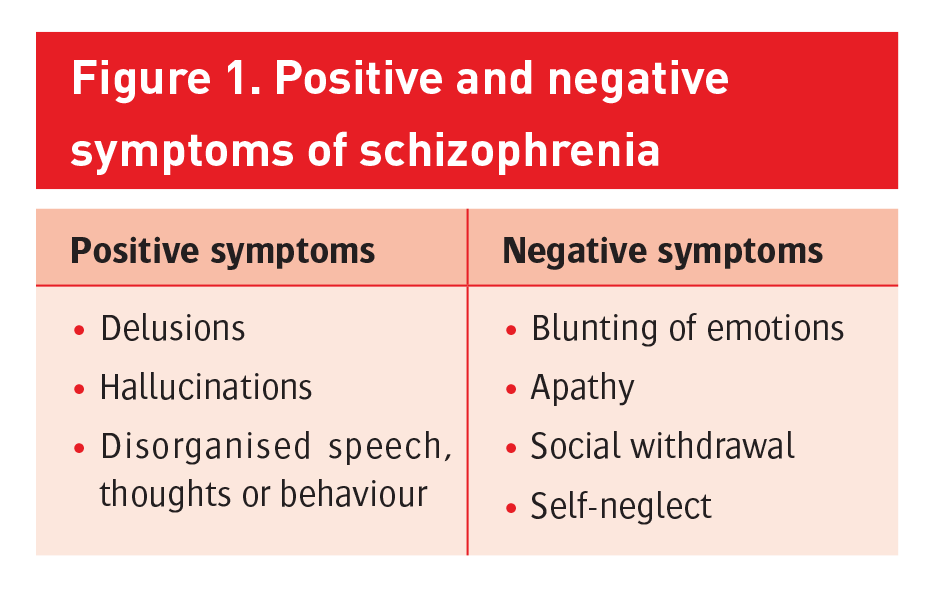
The ICD-10 generally describes symptoms as being positive or negative (see Figure 1). A diagnosis of schizophrenia requires at least two of the positive symptoms for at least one month or at least a year of negative symptoms. While positive symptoms are usually quite apparent, it takes careful observation to recognise the negative symptoms, particularly those with a more insidious onset – as these are generally the early indicators of the condition, and early recognition and treatment results in better prognosis.
Schizophrenia can often be predicted by ‘premorbid precursors’ in childhood and adolescence such as delays in language and motor development, social withdrawal, and social or behavioural problems. These symptoms can often go unnoticed or may be seen alongside a wide variety of other disorders. For example, social withdrawal is common in mood and developmental disorders, speech and thought disturbances are seen in autism, and behavioural disturbance is seen in ADHD and conduct disorders. It is not uncommon for individuals with comorbid diagnosis of one of the above to be diagnosed with schizophrenia in adolescence or young adulthood.
Figure 1. Positive and negative symptoms of schizophrenia(click to enlarge)
Risk factors
A number of risk factors for developing schizophrenia have been identified, but the link between what makes an individual more susceptible to psychoses and what causes schizophrenia to develop in a susceptible individual is still poorly understood.
There is certainly a large genetic component, with twin studies showing heritability estimates of around 80%.3 However, what is inherited is not the illness itself, but a predisposition to developing it. It has been acknowledged that obstetric and perinatal complications, such as foetal hypoxia and maternal infection or malnutrition, may have a role to play. Children brought up in urban environments, as well as those who are part of an immigrant ethnic minority have also shown higher incidences of schizophrenia later in life. Prolonged use of cannabis has been shown to put one at higher risk of developing a psychotic disorder.4 There is a lack of data surrounding other classes of recreational drugs, but it is felt that use of any drug that can induce a temporary psychotic state (LSD, psilocybin, mephedrone, ecstasy etc) increases the chances of developing schizophrenia. For example, a person with a family history of schizophrenia may constitute a ‘susceptible individual’. This person may try LSD at a party in their teenage years, which may cause a temporary psychosis. This may sensitise the person’s dopamine system to a disordered way of thinking. Psychotic episodes may return and become more prolonged over time resulting in a diagnosis of schizophrenia.
According to The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA, 2007) adolescents in Ireland have a higher than average prevalence of lifetime use of an illicit drug. Although, the latest Health Behaviour in School-aged Children survey (HBSC 2009/10), suggests a reduction in reported lifetime cannabis use among 15-16 year olds, from 24% in 2006, to 15% in 2009/10, studies in 15-34 year group (National Advisory Committee on Drugs and Alcohol; NACD) suggest an increase (33.4%).
Given these high rates of cannabis use and that drug induced psychoses are often the first presentation of patients who go on to be diagnosed with schizophrenia, there is little room for complacency with adolescent or youth drug use.
Assessment
If a diagnosis is suspected or being considered, it is crucial to have a recognised approach to assessment and further management. An important first step is to undertake a detailed medical assessment to rule out a potential organic cause for the picture. Cerebro-vascular disease, temporal lobe epilepsy and endocrine disorders may mimic psychiatric disorders, as can the side effects of prescribed medications such as anticonvulsants. This is usually done in a hospital or primary care setting by hospital doctors and GPs. Once a medical cause for the symptoms is ruled out, referral for psychiatric assessment should be made right away to avoid any delay in formal diagnosis. Psychiatric assessment should be part of a multidisciplinary approach that involves mental health professionals (psychiatrists, psychologists etc.), social workers and a community-based team.
Initial psychiatric assessment should include a detailed history from the patient. If presentation is in childhood or adolescence, the patient’s family should be involved in the assessment – which should always be carried out in an open and non-judgmental manner. Any previous mental health or developmental problems should be explored, as should any history of recreational drug use or significant alcohol history, any family history etc. Social networks, relationships, traumatic life events, educational and occupational history should all be examined.
The presenting symptoms should be explored, as well as premorbid behaviour and functioning along with any history of previous symptoms of a similar nature. It should be established if there is a risk of self-harm or violence towards others and, if so, steps should be taken to prevent this. If this is the case, voluntary admission should be sought where possible, but it may be necessary to invoke the Mental Health Act (Section 25), if the patient does not comply.
Treatment
The cornerstone of treatment remains antipsychotic medication, which is best used in combination with cognitive behavioural therapy, psychotherapy and community support. First generation antipsychotics such as chlorpromazine and haloperidol have generally been superseded by the newer atypical antipsychotics, particularly in the younger population. These include medications such as risperidone, olanzapine, quetiapine, ziprasidone and aripiprazole. These medications cause fewer motor side effects than the first generation antipsychotics, but are not without unpleasant adverse events of their own. Metabolic side effects such as weight gain, elevated triglycerides and cholesterol, cause one in 10 people on atypical antipsychotics to develop metabolic syndrome,5 which puts patients at a significant risk for developing cardiovascular disease (CVD) down the line.
When starting patients on antipsychotics, it is imperative that weights are checked at regular intervals along with blood pressure, fasting blood glucose, HbA1c and prolactin levels. If clinically indicated or there is a family history of CVD, a baseline ECG may be necessary (NICE guidelines). Patients should be monitored for response to treatment, ie. reduction in symptoms, improved functioning, monitoring side effects, emergence of movement disorders, adherence to medications and general physical health. If medications are started in childhood or adolescence, weight, height, and waist and hip circumference should be plotted on a centile chart.
Following failure of at least two different antipsychotic medications, a trial of clozapine is warranted. Clozapine is associated with better symptomatic reduction, but comes with a high risk (1-4%) of developing agranulocytosis and requires weekly blood testing to monitor white blood cell count.6
As with most mental illnesses, schizophrenia is a spectrum, and different patients present with different combinations of positive and negative symptoms. As such, treatment is tailored to the individual, with patients with predominantly positive symptoms responding well to antipsychotic medications and those with predominantly negative symptoms not doing as well. For these patients, cognitive behavioural therapy (CBT) can improve coping and reduce distress and negative affect associated with psychotic symptoms.7 In fact recent studies have shown that CBT is beneficial in most patients with a diagnosis of schizophrenia, with CBT-informed treatment showing reduced risk of relapse and better functioning at one and two years follow-up.8 CBT should be delivered over at least 16 planned sessions and should aim to establish links between the patient’s thoughts, feelings and actions, and their current or past symptoms. Perceptions and beliefs should be constantly re-evaluated and patients should be encouraged to understand and accept their experiences, and develop adaptive coping strategies with the main aim being to reduce distress and improve functionality.9
Alongside antipsychotic therapy and CBT, there is an important role for community-based multidisciplinary care. Patients will often require assistance finding work and accommodation, and may need help integrating socially. Families will need support and information, reducing levels of expressed emotion at home, and working with schools to keep stress level to a minimum and offer educational modifications where necessary. Support groups and social workers play an important role in any re-integration process.
More than half of patients with schizophrenia smoke, and rates of alcohol excess and cannabis abuse are far higher than in the general population. Drug and alcohol counselling and attention to lifestyle choices and general physical health are a fundamental part of the treatment plan. A well-knit support network between the primary practitioner (GP), key worker and community mental health team allows for earlier hospital discharge, reduced admissions and improves compliance with treatment programmes. Reports have shown that remission can now be achieved in approximately 80% of patients, provided treatment is put into place early in the course of the illness.10
Children and adolescence
Childhood onset schizophrenia involves onset of psychosis before the age of 13 and occurs in approximately 1/10,000 children, with age and rate of onset similar in girls and boys. Although the prevalence is very rare under the age of 13, 4% start before the age of 15 and 10% of psychoses start between the age of 16 and 20.
Florid symptoms may not emerge for some time, and long prodromal states, left untreated, result in poorer prognosis. Early intervention teams, such as DETECT in Ireland, may help reduce treatment delays by more than 50%.
The complexity of the evolving adolescent mind is becoming more difficult to explore, with fresh challenges faced every day. Drugs that were once unheard of in Ireland are now commonplace on our streets and readily available to a teenager who knows where to look. College trips to exotic countries such as Thailand are often not complete without cathartic experiences under the influence of hallucinogenic drugs. Head shops and internet sites are supplying young people with substances whose pharmacology is poorly understood and the stigma once attached to recreational drug use is fading rapidly. Although prevalence of schizophrenia remains fairly constant, we are seeing rising trends in the diagnosis of drug-induced psychoses11 and it is yet to be seen what the long term implications of this will be.
Tackling stigma
Philip K Dick once described psychosis as “a dream breaking through during waking hours”. A novelist and philosopher, Dick’s works inspired such popular films as Blade Runner, Total Recall and Minority Report. He was one of a number of prominent figures throughout modern history to achieve great things in spite of a background diagnosis of schizophrenia.
As mental disorders go, schizophrenia remains associated with a high degree of stigma, the general perception being that schizophrenics do not integrate well with society, are unstable and are prone to violent outbursts. These widely held beliefs are outdated and result in further marginalisation of an already vulnerable population. Even the term ‘schizophrenia’ itself is being examined. Roughly translated from the Greek for ‘split mind’, the Japanese have already abandoned the term in favour of ‘integration-deregulation syndrome’.
The shattering of the stigma is one of the great challenges that we are faced with in battling mental health problems, and ‘living with schizophrenia’ was the theme for World Mental Health day, 2014. If schizophrenia was viewed in a less negative light, we would see patients seeking help sooner and those diagnosed with the disorder integrated more smoothly into society, leading to a better long-term prognosis and a decreased disease burden. Media campaigns and initiatives aimed at raising awareness of mental health issues will help reduce the stigma, and hopefully result in increased access to effective interventions. ‘First Fortnight’, an Irish charity, challenges mental health prejudice through the creative arts by hosting a two week arts festival each January.
Conclusion
Mental health is finally becoming a priority with the recognition of ‘No Health without Mental Health’ (UK MH Strategy, 2011). Our own MH Policy, A Vision for Change, and public campaigns, such as that led in January 2015 by ‘First Fortnight’, will ensure that this ambition is realised. There remains a lot of work to ensure best treatment outcomes for individuals with schizophrenia and psychoses, but we are moving in the right direction. A diagnosis that was once considered frightening can be looked upon as treatable and, with early recognition and treatment, as well as an informed and educated public, ensures that most patients with schizophrenia recover and live a full and productive life.
References
Perala J, Suvisaari J, Saarni SI et al. Lifetime prevalence of psychotic and bipolar I disorders in a general population. Arch Gen Psychiatry 2007; 64:19-28
Saha S, Chant D, McGrath J. A Systematic Review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch Gen Psychiatry 2007 Oct; 64(10):1123-31
Van Os J, Kapur S. Schizophrenia. The Lancet Vol 374
Moore TH, Zammit S, Lingford-Hughes A et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review. Lancet 2007; 370: 319-28
Patel JK, Buckley PF, Woolson S et al. Metabolic profiles of second- generation antipsychotics in early psychosis: findings from the CAFE study. Schizophr Res 2009; 111: 9-16
Leucht S, Corves C, Arbter D et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet 2009; 373: 31-41
Wykes T, Steel C, Everitt B, Tarrier N. Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor. Schizophr Bull 2008; 34: 523-37
Hutton P, Taylor PJ. Cognitive behavioral therapy for psychosis prevention: a systematic review and meta-analysis. Psychol Med 2014 Feb; 44(3):449-68
Kendell T, Hollis C, Stafford S, Taylor C. Recognition and management of psychosis and children in children and young people: summary of NICE guidance. BMJ. 2013; 346:f150
Robinson D,Woerner MG, Alvir JM et al. Predictors of relapse following response from a first episode of schizophrenia or schizoaffective disorder. Arch Gen Psychiatry 1999; 56: 241-47
Kirkbride JB, Croudace T, Brewin J et al. Is the incidence of psychotic disorder in decline? Epidemiological evidence from two decades of research. Int J Epidemiol 2009; 38 (5): 1255-1264
Psychosis and schizophrenia in children and young people: recognition and management. NICE clinical guideline 155 (2013)
European Monitoring Centre for Drugs and Drug Addiction www.emcdda.europa.eu
National Advisory Committee on Drugs and Alcohol; NACD www.nacd.ie
Health Behavior in School-aged Children (HBSC), 2009-2010 http://doi.org/10.3886/ICPSR34792.v1
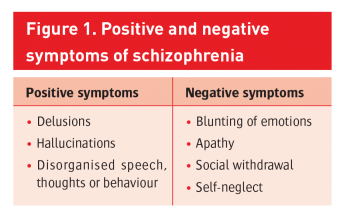 Figure 1. Positive and negative symptoms of schizophrenia(click to enlarge)
Figure 1. Positive and negative symptoms of schizophrenia(click to enlarge)