Sleep-disordered breathing: presentations and treatment
The reported increase of obstructive sleep apnoea syndrome in paediatric populations largely reflects the increasing prevalence of childhood overweight and obesity
Dr Peter Greally, Consultant Respiratory Paediatrician, National Children’s Hospital, Our Lady’s Children’s Hospital, and Charlemont Clinic, Dublin, Mr David Burke, Final Medical Student, National Children's Hospital, Tallaght, Dublin and Dr Oneza Ahmareen, SpR in Respiratory Medicine, National Children's Hospital, Tallaght, Dublin
The American Academy of Pediatrics clinical diagnosis and management guidelines define sleep-disordered breathing (SDB) “as a disorder of breathing during sleep characterised by prolonged partial upper airway obstruction and/or intermittent complete obstruction (obstructive apnoea) that disrupts normal ventilation during sleep and normal sleep patterns, leading to symptoms and signs”.1
Epidemiology
The reported prevalence of SDB, or what was formerly described as obstructive sleep apnoea syndrome (OSAS), has increased in paediatric populations in the developed world. This trend largely reflects the increasing prevalence of childhood overweight/obesity. We recently reported the prevalence of overweight/obesity in 25% of randomly selected healthy Irish school children.
The reported prevalence varies between 2-6% in school-aged children. Obstructive sleep apnoea has a peak incidence between two to eight years of age, which mirrors the peak in growth of the palatine tonsils and adenoids. However, it may affect children at any age, particularly obese adolescents.2,3
Predisposing factors are listed below:4
Adenotonsillar hypertrophy
Increased BMI
Craniofacial syndromes (Pierre-Robin, Apert’s)
African-American race
Upper respiratory tract disease
History of low birthweight5,6
Mucopolysaccharidoses (eg. Hurler and Hunter syndrome)
Orthodontic problems
Family history of OSAS.7,8
Individuals with any condition that gives rise to a less capacious nasopharynx are at higher risk, eg. craniofacial abnormalities, adenotonsillar hypertrophy, increased parapharyngeal adipose tissue, Down’s syndrome and Prader-Willi syndrome.
OSAS is more common in children with neuromuscular disease where arousal responses are impaired and there may be increased hypotonia of the upper airway, eg. muscular dystrophy, cerebral palsy, and Arnold-Chiari malformation. OSAS may be familial and is commoner in African-Americans where comorbidity with sickle cell disease may provide particular challenges from both the diagnostic and therapeutic perspective.
Clinical presentation
History
The presenting complaint to the GP may depend on the age of the child. Parents of preschool children may complain of their snoring at night. Habitual snoring in the paediatric population may be high as 12%, but does not always mean a child suffers from OSAS.12 Conversely, the absence of snoring does not necessarily exclude OSAS.13 Other common symptoms include mouth breathing, sweating, restlessness, frequent awakenings at night and witnessed apnoeic episodes.
Symptoms are often worse in the supine position. School-aged children with OSAS may present with secondary enuresis, behavioural problems, attention deficit and failure to thrive. Older children and teenagers may complain of excessive daytime sleepiness.
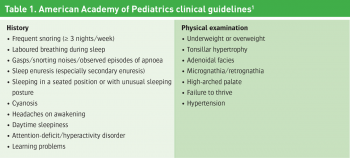
Chervin et al14 interviewed the parents of 866 children about their sleep behaviour. They specifically assessed the presence of attention/hyperactivity disorder. As many as 22% of habitual snorers reported attention deficit and/or hyperactivity compared to only 12% of non-snorers.14 Table 1 outlines the signs and symptoms highlighted by the American Academy of Pediatrics clinical guidelines.1
(click to enlarge)
Physical examination
Affected children may speak with hyponasal speech or rely on mouth breathing. Some children may be obese whereas others may fail to thrive.16,17
It is hypothesised that the latter is explained by the increased work of breathing associated with abrupt arousal from apnoeic states depletes the child of necessary energy for growth and development.16 These children have been shown to thrive following adenotonsillectomy for OSAS.6,18
A thorough head and neck exam is an essential part of the evaluation in a child with suspected OSAS. The child should be inspected for craniofacial anomalies such as retrognathia, micrognathia, adenoidal facies (decreased nasal airflow, mouth breathing) and nasal congestion. Children should be evaluated for oropharyngeal crowding, noting tonsil size and using tools such as the Mallampati score.19
OSAS is associated with systemic hypertension and less frequently with pulmonary hypertension, warranting a blood pressure measurement and cardiac evaluation in each case of suspected OSAS.20, 21
Radiographs of the posterior nasal space may reveal the degree of adenoidal enlargement. However, these X-rays are often taken in the standing position in the awake state and take no account of the dynamic changes in airway tone during sleep, especially rapid eye movement (REM).
Polysomnography
Polysomnography (PSG) is the gold standard investigation for the diagnosis of sleep-disordered breathing. Full PSG requires elective admission to hospital with an overnight PSG the preferred choice, as greater possibility of sufficient duration of sleep to occur, with a likelihood of capturing periods of REM where hypoventilation is most likely to occur.
Multiple channels record variables including video montage, nasal and oral airflow, abdominal and chest wall movements, end-tidal CO2, oxyhaemoglobin saturation, continuous EEG, continuous ECG and a snore microphone.
The evaluation permits the detection of:
Apnoeic and hypopnoeic events
Hypoventilation
Arousals
Snoring
Alteration in body position
Limb movements.
Montage is scored using the American Academy of Sleep Medicine criteria (2007).
The most commonly quoted variable is the apnoea-hypopnea index (AHI) which consists of all the scored apnoeic and hypopnoeic events divided by the total sleep time and is expressed in events per hour. An AHI of less than 1/hr is normal. Those between 1-5/hr are termed equivocal and will comprise of some patients who will require intervention. Values greater than 5/hr are abnormal and many of these patients will require intervention. An AHI of greater than 10/hr is considered severe.
Management
The decision to initiate treatment is on an individual basis based upon the clinical picture and the risks and benefits involved. Important determinants include age, sleep study abnormalities and any underlying medical conditions related to OSAS.1
Adenotonsillectomy is the first-line therapy in children who suffer from OSAS with adenotonsillar hypertrophy. Adenotonsillectomy may also be the initial treatment for children with multifactorial OSAS who present with sizeable adenotonsillar tissue hypertrophy. While not correcting the main aetiologies, clinically it has been shown to improve obstructive signs in certain cases.23
Continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP) can be used where adenotonsillectomy is contraindicated or has failed as a primary treatment.1 The main inhibitory factor in the use of positive airway pressure lies in the lack of compliance.24 Education, training, and close follow-up may tackle this issue.
Other therapies
Avoidance of environmental pollutants and allergens is advocated in the presence of allergic rhinitis causing nasal congestion and increased airway resistance.1 In a recently published study of obese Belgian children, it has been demonstrated that residential care with calorie control diets and rigorous exercise reduces BMI and improves OSAS.24 Weight loss is recommended in obese children, but there have been no studies in the paediatric population advocating this; thus we must rely on evidence based on adult OSAS studies.
In selected cases of OSAS associated with maxillary contraction (high arched palate, crossbite) orthodontic interventions have been successful in reducing the AHI in affected individuals, but further trials are required to identify the appropriate treatment group.25
Intranasal corticosteroids have demonstrated effective treatment response in children with moderate-to-severe OSAS unsuitable for adenotonsillectomy as well as in mild OSAS where adenotonsillectomy is not warranted.26 In a randomised double blind trial of six-week administration of intranasal budesonide versus placebo in children with mild OSAS, there was significant improvement in PSG measurements, with a sustained benefit lasting eight weeks post-therapy discontinuation.27
Small studies have evaluated leukotriene receptor antagonist and have concluded that montelukast either alone or in conjunction with intranasal corticosteroids modestly decreases AHI.
Differences to adults
OSAS in children differs in a number of ways from the condition in adults. Firstly, snoring is less common in children. Apnoea/hypopnoea indices tend to be much higher in adults. Obesity is the main aetiological factor in adults whereas adenoidal and tonsillar hypertrophy have a significant role in the development of OSAS in childhood, thus adenotonsillectomy is rarely indicated in adults. Whereas excessive daytime somnolence is a common feature in adults, difficulty with concentration, poor school performance and attention deficit/hyperactivity disorder are the predominant complaints in children.
There are few published studies which assess the long-term outcomes of OSAS in childhood. In one small series, three of 28 young adults treated successfully for OSAS in the prepubertal period had abnormal PSGs and increased collapsibility of their upper airway during sleep.
With the observed increases in childhood overweight/obesity observed in developed countries, the phenotype associated with obesity is less likely to be remediable with surgical intervention only.
Studies in adults suggest that OSAS increases progressively over time if untreated. Finally, there is a paucity of data relating to the natural history of mild to moderate forms of OSAS in childhood, which may only relate to peak lymphoid tissue growth.
Conclusion
Adenotonsillectomy has been the mainstay in treatment for OSAS and associated adenotonsillar hypertrophy. In a multicentre retrospective study in 2010,28 where 578 children were evaluated post-adenotonsillectomy, 90% of the cohort showed a decreased AHI.
However, only 28% had normal AHI at follow up. The study determined that age (> 7 years old) and BMI were principal determinants for persisting OSAS, highlighting the importance of careful review of all possible causes of OSAS.29 Nasal CPAP therapy has been evaluated by several studies and has shown improvement in signs and symptoms as well as improvement in sleep study results in at least 85% of children.30,31,32,33
References
Marcus CL, Brooks LJ, Draper KA et al. Clinical Practice Guideline: Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics 2012; 130(3): 576-584 doi: 10.1542/peds. 2012-1671
Carroll JL. Obstructive sleep-sleep disordered breathing in children: new controversies, new directions. Clin Chest Med 2003; 24: 261-282
Gislason T, Benediktsdottir B. Snoring, apneic episodes and nocturnal hypoxaemia among children 6 months to 6 years old: an epidemiologic study of lower limit of prevalence. Chest 1995; 107: 963-966
Redline S,Tishler P, Schluchter M et al. Risk factors for sleep-disordered breathing in Children. Am J Respir Crit Care Med 1999; 159: 1527-1532
Rosen CL, Larkin EK, Kirchner HL et al. Prevalence and risk factors for sleep-disordered breathing in 8 to 11 year old children: association with race and prematurity. J Pediatr 2003; 142(4): 383-389
Paavonen EJ, Strang-Karlsson S, Raikkonen K et al. Very low birth weight increases risk for sleep-disordered breathing in young adulthood: the Helsinki Study of Very Low Birth Weight Adults. Pediatrics 2007; 120: 778
Redline S, Tishler PV, Tosteson TD et al. The familial aggregation of obstructive sleep apnea. Am J Respir Crit Care Med 1995; 151: 682
Buxbaum SG, Elston RC, Tishler PV, Redline S. Genetics of the apnea hypopnea index in Caucasians and African Americans: I. Segregation analysis. Genet Epidemiol 2002; 22: 243
Marcus Cl, Omlin KJ, Basinki DJ et al. Normal Polysomnographic value for children and Adolescents. Am Rev Respir Dis 1992; 146: 1235
Hudgel DW, Martin RJ, Johnson B, Hill P. Mechanics of the respiratory system and breathing pattern during sleep in normal humans. J Appl Physiol 1984; 56: 133-137
McIntosh N, Helms P, Smyth R. Forfar and Arneils Textbooks of Paediatrics 2003; 6: 746-747
Carroll JL, McColley SA, Marcus CL, et al. Inability of clinical history to distinguish primary snoring from obstructive sleep apnea syndrome in children. Chest 1995; 108: 610
Rosen CL, Storfer-Isser A, Taylor HG et al. Increased behavioral morbidity in school-aged children with sleep-disordered breathing. Pediatrics 2004; 114: 1640
Chervin RD, Archbold KH, Dillon JE et al. Inattention, hyperactivity, and symptoms of sleep-disordered breathing. Pediatrics 2002; 109: 449
Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. American Academy of Pediatrics. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109: 704
Marcus CL, Curtis S, Koerner CB et al. Evaluation of pulmonary function and polysomnography in obese children and adolescents. Pediatr Pulmonol 1996; 21: 176
Silvestri JM, Weese-Mayer DE, Bass MT et al. Polysomnography in obese children with a history of sleep-associated breathing disorders. Pediatr Pulmonol 1993; 16: 124
Williams EF 3rd, Woo P, Miller R, Kellman RM. The effects of adenotonsillectomy on growth in young children. Otolaryngol Head Neck Surg 1991; 104: 509
Nuckton TJ, Glidden DV, Browner WS, Claman DM. Physical examination: Mallampati score as an independent predictor of obstructive sleep apnea. Sleep 2006; 29: 903
Marcus CL, Greene MG, Carroll JL. Blood pressure in children with obstructive sleep apnea. Am J Respir Crit Care Med 1998; 157: 1098
Guilleminault C, Korobkin R, Winkle R. A review of 50 children with obstructive sleep apnea syndrome. Lung 1981; 159: 275
American Academy of Sleep Medicine. International classification of sleep disorders, 2nd ed. American Academy of Sleep Medicine: Westchester, 2005
Pavone M, Paglietti M, Petrone A et al. Adenotonsillectomy for obstructive sleep apnea in children with Prader-willi syndrome. Pediatr Pulmonol 41: 74-79
Marcus CL, Rosen G, Ward SL et al. Adherence to and effectiveness of positive airway pressure therapy in children with obstructive sleep apnea. Pediatrics 2006; 117: e442
25 Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep 2004; 27: 761
Brouillette RT, Manoukian JJ, Ducharme FM, et al. Efficacy of fluticasone nasal spray for pediatric obstructive sleep apnea. J Pediatr 2001; 138: 838
Kheirandish-Gozal L, Gozal D. Intranasal Budesonide Treatment for Children with Mild Obstructive Sleep Apnea Syndrome. Pediatrics 2008; 122; 149
Van Hoorenbeeck K, Franckx H, Debode P et al. Weight loss and sleep-disordered breathing in childhood obesity: effects on inflammation and uric acid. Obesity 2012; 20(1): 172-177
Bhattscharjee R, Khierandish-Gozal L, Spruyt K et al. Adeno-tonsillectomy outcomes in treatment of obstructive sleep apnea in children: a multicentre retrospective study. Am J Respir Crit Care Med 2010; 182: 676
Marcus CL, Ward SL, Mallory GB et al. Use of nasal continuous positive airway pressure as treatment of childhood obstructive sleep apnea. J Pediatr 1995; 127: 88
Waters KA, Everett FM, Bruderer JW, Sullivan CE. Obstructive sleep apnea: the use of nasal CPAP in 80 children. Am J Respir Crit Care Med 1995; 152: 780
Guilleminault C, Pelayo R, Clerk A et al. Home nasal continuous positive airway pressure in infants with sleep-disordered breathing. J Pediatr 1995; 127: 905
Padman R, Hyde C, Foster P, Borkowski W Jr. The pediatric use of bilevel positive airway pressure therapy for obstructive sleep apnea syndrome: a retrospective review with analysis of respiratory parameters. Clin Pediatr (Phila) 2002; 41: 163
 (click to enlarge)
(click to enlarge)