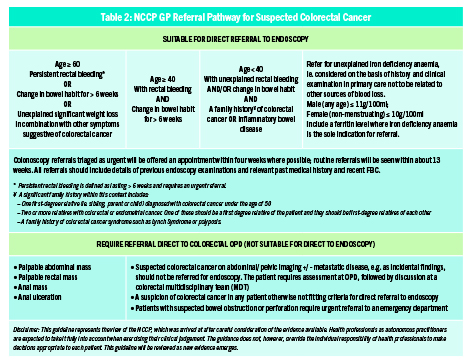
The National Cancer Control Programme has developed a GP Referral Pathway for Suspected Colorectal Cancer that GPs may use to assist them in identifying which patients require referral
Colorectal cancer (CRC) is the third most common cancer worldwide; almost 2 million cases of this disease were diagnosed in 2020,1 and almost one million deaths annually are caused by this disease.
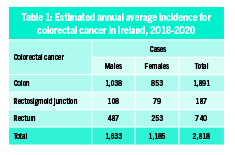
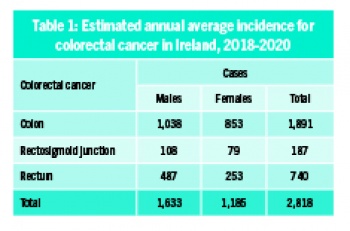
In Ireland, CRC is the third most common invasive cancer and the second most common cause of cancer death. The estimated annual average incidence for colorectal cancer in Ireland between 2018 and 2020 was 2,818 cases per annum (see Table 1).2 This represents 11.4% of invasive cancers (excluding non-melanoma skin cancer). There are approximately 1,000 deaths from this disease annually in Ireland.
(click to enlarge)
Men are more likely than women to develop CRC in this country; the cumulative lifetime risk (to age 74 years) of developing CRC for a male in Ireland is 1 in 27, and for a female is 1 in 39.3
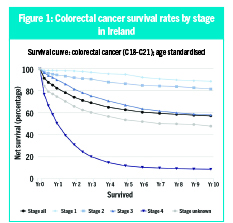
The minority of cases of CRC in Ireland are diagnosed at an early stage; approximately 15% of cases are diagnosed at stage 1 disease, while a further 25%, approximately, are diagnosed at stage 2.3 Overall five-year survival for CRC in Ireland is 62.6%. However, stage at diagnosis has a marked impact on survival from this disease; five-year survival at stage 1 disease is almost 95%, but falls to just 12% at stage 4 (see Figure 1).4
(click to enlarge)
In Ireland, while there appears to be no relationship between deprivation and CRC incidence, deprivation has been shown to be linked to poor survival from CRC. Patients from the most deprived group showed significantly poorer survival (age/sex-adjusted mortality risk 24% higher) relative to the least deprived group.5 In addition, urban patients from the most deprived group were significantly more likely (+20% in relative terms) to present at stage 4 compared with the least deprived group.5
Pathophysiology
CRCs arise from dysplastic adenomatous polyps in the majority of cases via two distinct pathways6: conventional adenoma-to-carcinoma and serrated adenoma-to-carcinoma. Conventional adenomas develop from a mutation in the adenomatous polyposis coli (APC) tumour suppressor gene; progression to cancer is a multi-step process. The genetic defect that gives rise to serrated adenomas is not known.6
CRC typically metastasises to local lymph nodes, to the liver via venous drainage and via the bloodstream to the lungs, and less commonly to bone and brain.7
Risk factors for CRC
Around 70-75% of colorectal cancer cases occur sporadically and are associated with modifiable risk factors, whereas 25-30% of cases are linked to non-modifiable risk factors such as a personal history of polyps or adenoma, or a family history of colorectal cancer or hereditary risk (eg, Lynch syndrome or familial adenomatous polyposis).8
Age
Increasing age is the greatest risk factor for sporadic CRC. The vast majority (almost 90%) of cases of CRC in Ireland occur in people over the age of 50 years.3
However, while absolute numbers remain low, rising rates of CRC in younger adults have been noted in recent years. Between 1990 and 2019 there has been a significant increase in CRC incidence in adults aged < 50 years, especially in developed countries.8
A 2020 systematic review9 found a worldwide increase in CRC in younger adults largely driven by increasing incidence in the US, Australia, and Canada, with the greatest increase occurring in distal colon and rectal cancers.10 It is thought that the main drivers of this phenomenon are lifestyle factors such as diet, obesity and lack of exercise, although further research is needed in this area.
Family history
Family history has a powerful impact on risk of developing CRC. For individuals with one affected first-degree relative, the relative risk of developing CRC is 2.24. This increases to 3.97 with two affected first-degree relatives.11
Lynch syndrome is among the most common forms of inherited cancer susceptibility. Current estimates are that up to one in 300 people has Lynch syndrome and up to 95% of cases are undiagnosed.12 It is an autosomal dominant condition, thought to account for up to 3% of colorectal cancers, as well as being associated with an increased risk of endometrial cancer in women, and other extra-colonic malignancies.13
It is caused by a germline mutation in one of a group of mismatch repair genes including MLH1, MSH2, MSH6 or PMS2 or a germline deletion in EpCAM (leading to epigenetic inactivation of MSH2).13 The Lynch syndrome phenotype is characterised by a predominance of cancers on the right side of the colon. The lifetime risk of CRC in people with Lynch syndrome is 50-80%, which can be reduced with colonoscopic surveillance.
Familial adenomatous polyposis (FAP)
Familial adenomatous polyposis is an autosomal dominant syndrome caused by a germline mutation in the adenomatous polyposis coli (APC) gene on chromosome 5q. It accounts for 1% of colorectal cancer cases. Most patients (approximately 70%) have a family history of CRC.14 In the EU, prevalence of FAP has been estimated at one in 11,000-37,000. Those affected typically develop hundreds to thousands of adenomatous polyps in the colon and rectum by the time they are 20-30 years old and, without prophylactic surgical resection, will inevitably develop colorectal cancer.
Hamartomatous polyposis syndromes
Hamartomatous polyposis syndromes include rare inherited syndromes such as juvenile polyposis, PTEN hamartoma tumour syndrome (includes Cowden syndrome), and Peutz-Jeghers syndrome.15 CRC may occur due to adenomatous change within the hamartomas. The lifetime risk of developing CRC in patients with these syndromes is thought to be as high as 39% and is thought to be due to adenomatous changes within the hamartomas.16
Inflammatory bowel disease (IBD)
Inflammatory bowel disease (including ulcerative colitis and Crohn’s disease) is a chronic progressive disease of the gastrointestinal tract.17 IBD patients are two to six times more likely to develop CRC than the general population18 due to chronic inflammation of the affected intestine.19 In addition, IBD patients tend to develop CRC at a younger age.
In general, CRC risk begins to increase 8-10 years after the diagnosis of inflammatory bowel disease is made and increases over time. Geography plays a role in IBD-CRC development; the risk is higher in North America and the UK than in Scandinavian countries. Finally, similar to sporadic CRC, family history plays a role in the risk of developing CRC in patients with IBD – those with a first-degree relative diagnosed with CRC before the age of 50 have a nine-fold higher risk.20
Human papillomavirus (HPV)
Human papillomavirus (HPV) is a double stranded DNA virus that infects squamous epithelia including the skin and mucous membranes of the upper respiratory and anogenital tracts. HPV has a causal association with anal cancer. In Ireland, from 2010-2014, an estimated average of 538 cases of HPV-associated cancers were diagnosed per year. Of these, 31 were cancers of the anus and rectum.21
Other risk factors for CRC
Obesity is associated with an increased risk of developing CRC compared with normal-weight individuals.22 Lack of dietary fibre, consuming a diet high in processed and red meat also increase the risk of developing the disease.23 Physical activity, however, reduces the risk of the disease. There is an inverse relationship between physical activity and colon (but not rectal) cancer.24
Primary prevention of CRC
Ireland does not have specific guidelines relating to the use of medication for primary prevention of CRC. However, the UK’s National Institute for Health and Care Excellence (NICE) recommends daily aspirin (taken for more than two years), to prevent colorectal cancer in people with Lynch syndrome.25
In the US, the US Preventive Services Task Force recommends initiating low-dose aspirin for the primary prevention of cardiovascular disease and colorectal cancer in adults aged 50-59 years with a 10% or greater 10-year cardiovascular disease risk who are not at increased risk for bleeding and have a life expectancy of at least 10 years.26
The American College of Gastroenterologists recommends low-dose aspirin for those aged between 50 and 69 years with a cardiovascular disease risk of 10% or greater over the next 10 years, who are not an increased risk for bleeding.27
There is insufficient evidence to support a recommendation for aspirin for primary prevention of CRC in other age groups.
(click to enlarge)
Screening for CRC
Bowelscreen
Bowelscreen, Ireland’s national screening programme for bowel cancer, commenced in 2012. This screening programme aims to reduce mortality from colorectal cancer in men and women aged 55-74 in Ireland. The programme is being implemented on a phased basis beginning with men and women aged 60-69. It is important to note that the maximum benefits, in terms of reduction in mortality and cost-effectiveness, will occur only when the programme targets the full 55-74 age population.28
Bowel screening can both prevent CRC by detecting pre-cancerous adenomas in the lining of the bowel, and detect CRC at an early stage in people who are asymptomatic, when cure rates are significantly higher.
Screening is available to all males and females living in Ireland, every two years, aged between 60-69.28 Eligible members of the population must be on the Bowelscreen register in order to be invited to take a screening test. Patients may be advised that they may self-register for Bowel-screen either online (www.bowelscreen.ie) or by telephone (1800 454 555).
To undertake bowel screening, participants are invited by letter to take a FIT test, which is a home test kit that detects occult blood in the stool. The kit is returned by Freepost by the patient for analysis by a contracted laboratory. Approximately 96% of participants’ tests are returned by the laboratory as a normal result.
If a person has a positive (not normal) test result, they move to the endoscopy stage of the pathway, where they are offered a colonoscopy in one of the programme’s colonoscopy units. Once this is completed, the person is either discharged, offered a surveillance scope at a planned interval to monitor them, or offered treatment if a cancer has been diagnosed.28
FIT test
The faecal immunochemical test (FIT) checks for occult blood in the stool. It has a number of advantages over guaiac-based tests (GFOBT)29:
• FIT tests are more sensitive and specific for CRC than GFOBT
• FIT tests are specific to human blood and are therefore not affected by diet, eg. consuming red meat before taking the test. There are also no false positives from upper gastro-intestinal bleeding
• FIT testing is a simpler test for patients to take than GFOBT.
Bowelscreen uptake
Despite the benefits of bowel screening, uptake remains low in Ireland at approximately 42%, particularly among men. Data from Bowelscreen demonstrate that uptake of Bowelscreen is higher among females than males across all age groups.28 Given that CRC more commonly affects males than females,2 and males are less likely to survive CRC,3 this is of particular concern.
There are evidence-based interventions that healthcare professionals, including GPs, can employ to improve uptake of screening including30:
• Client reminders
• Use of small media
• One-on-one education.
(click to enlarge)
Limitations of bowel screening
It is important to note that no screening test is 100% accurate. FIT relies on a cancer or adenoma bleeding at the time of the test.28 Thus, there may be false negatives where the FIT is negative and a lesion is present, and conversely, there may be false positives where the FIT is positive, and a subsequent colonoscopy shows no significant cause.
In some of these cases, it may be that the FIT detects blood from hernias or piles, rather than adenomas linked to cancer. In addition, interval cancers, ie. cancers that present between screening rounds, may occur. A negative screening test should not preclude appropriate investigation in a patient with symptoms suspicious for cancer.
Bowelscreen results
Between January 1, 2018 and December 31, 2019, 534,926 males and females in Ireland were invited to participate in Bowelscreen with a resulting uptake among invitees of approximately 42%. The ‘FIT positive’ rate, ie. the percentage of FIT tests that reached the threshold for blood in stool was 3.3%.30
Over 9,000 colonoscopies were completed, with 304 cancers detected; 192 colon cancers, 94 rectal cancers and 18 cases of cancer where the site was unconfirmed, giving an overall cancer detection rate of 1.4 per 1,000 participants screened by the FIT. In addition, 8,616 adenomas were removed, giving an adenoma detection rate (ADR) on index colonoscopy of 55.1%.30
The cancer detection rate among male participants was higher than for female participants.
Where stage was known to the programme, over 58% were stage 1 or 2. This contrasts with overall figures for CRC in Ireland where approximately just 40% of CRCs are detected at stage 1 or 2.3
Signs and symptoms of colorectal cancer
Rectal bleeding
About 40% of patients with CRC will have rectal bleeding but the risk of colorectal cancer for a patient who presents with rectal bleeding is thought to be relatively low31. A 2006 primary care-based prospective study has shown that, in patients aged > 45 years, rectal bleeding was associated with positive predictive value for colorectal cancer of 5.7% (3.2% to 9.2%). This value was 4.9% (2.6% to 8.4%) for adenoma.
Thus, 1 in 10 patients aged > 45 years with rectal bleeding had colorectal neoplasia.31 The National Cancer Control Programme’s (NCCP) GP Referral Pathway for Suspected Colorectal Cancer offers guidance to GPs about which patients to refer for endoscopy in the case of rectal bleeding (see Table 2).23
Change in bowel habit
Increased frequency of bowel motions, with looser stools, with or without rectal bleeding, is common in left-sided CRC. Constipation (reduced frequency of bowel motion, with hard stools) has a low predictive value for CRC.32
(click to enlarge)
Other symptoms
Loss of weight, abdominal tenderness and abdominal pain all have low positive predictive values for bowel cancer.32
Iron-deficiency anaemia
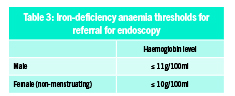
Iron-deficient anaemia has long been recognised as a feature of CRC.33 Almost 90% of patients with right-sided CRCs are anaemic at diagnosis.33 The risk of CRC rises as the haemoglobin level falls.34 Serum ferritin is the protein in the plasma that reflects the body’s iron stores. Ferritin levels are labile and increase when there is inflammation or hepatocellular damage. However, for all practical purposes, a low ferritin level is only seen in iron deficiency.35
The NCCP GP Referral Pathway for Suspected Colorectal Cancer describes unexplained iron-deficiency anaemia as anaemia that is ‘considered on the basis of history and clinical examination in primary care not to be related to other sources of blood loss’, and advise referral for endoscopy for patients in the circumstances outlined in Table 3.
Blood markers
Some blood-based markers are used for surveillance of disease post treatment. These include carcinoembryonic antigen (CEA) and cancer antigen CA19.9. These tests have low sensitivity and specificity ranging from 40-70% and 73-90% respectively, making them unsuitable as screening or diagnostic markers.36 Indeed, blood markers are insufficiently sensitive or specific to be used alone as post-treatment surveillance.37
Colonoscopy
Colonoscopy is the investigation of choice and allows tissue diagnosis38 and removal of incidental polyps. CT, including CT colonography, is of comparable sensitivity to colonoscopy for the detection of clinically significant polyps and tumours. It is the radiological investigation of choice when colonoscopy is contraindicated.38
Barium enema is a less sensitive investigation38 which has been supplanted by colonoscopy and CT colonography.
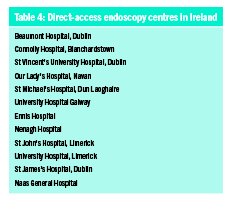
Referral for suspected CRC
Patients with suspected CRC may be referred by their GP for direct-access colonoscopy (where available) or to a colo-rectal or gastroenterology outpatient department for urgent review. Direct access referrals may be made electronically by GPs to the hospitals listed in Table 4.
Electronic referral is available via the four ICGP-accreditated GP software systems: Socrates, Health One, Complete GP and Helix Practice Manager. For GPs who do not use any of these software systems, referrals may be sent via Healthlink, the HSE messaging system which is available free of charge to all GPs. The NCCP recommends that electronic referral, where available, is the preferred method of referral. Faxed referrals are no longer recommended.
Treatment for CRC
Surgical resection of localised CRC is the mainstay of curative treatment. Minimally invasive colectomy/partial colectomy by an experienced laparoscopic surgeon should be considered in appropriate patients;2 however, even for patients undergoing curative resection, the role of extended lymphadenectomy remains uncertain.2 Robotic surgery provides similar short-term advantages to laparoscopic surgery; however, long-term outcome comparisons, including cancer-related outcomes, are not yet available for robotic surgery.2
Pre-operative neoadjuvant and post-operative chemotherapy and/or radiotherapy may be required. The chemotherapy treatment regimen to be used should take into account factors such as histology, molecular pathology, age, performance status, comorbidities and the patient’s preference. Details on the preferred chemotherapy treatment regimens in Ireland can be found on the NCCP website (www.hse.ie/eng/services/list/5/cancer/profinfo/chemoprotocols/gastrointestinal/).
Monitoring
Patients who have had potentially curative surgical treatment for non-metastatic colorectal cancer should be offered follow-up for detection of local recurrence and distant metastases for the first three years. Follow-up should include serum carcinoembryonic antigen (CEA) and CT scan of the chest, abdomen and pelvis. Patients with more advanced disease may require more frequent surveillance.
Complications
Short-term complications of treatment for CRC include side-effects of chemotherapy; including bone marrow suppression, hepatotoxicity, gastrointestinal upset (nausea, vomiting, diarrhoea, abdominal pain) and alopecia. Immunotherapies may lead to anaemia, fatigue, dysphagia, neutropenia, lymphopenia and hypertension.
Loose stool, urgency and faecal incontinence are common after radiotherapy for rectal cancer.
Rectal excision may result in erectile dysfunction, and bladder dysfunction due to damage to pelvic nerves, leading to urinary urgency, incontinence, and retention.
Low anterior resection syndrome (LARS) has a high prevalence (60-90%) after anterior resection and symptoms can last for years after surgery.39 Symptoms of LARS include increased frequency of stool; urgency, with or without incontinence, of stool; feeling of incomplete emptying; fragmentation of stool (passing small amounts little and often); and difficulty in differentiating between gas and stool.40 Management of LARS is symptom-based with little evidence to guide management, and consists of using existing therapies for faecal incontinence, urgency and rectal dysfunction.41
Palliative care
Palliative care may improve the quality of life of people and their families facing the problems associated with life-limiting illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems: physical, psychosocial and spiritual.42 It is a vital and integral part of all clinical practice.
When combined with standard cancer care or as the main focus of care, palliative care leads to better patient and caregiver outcomes. These include improvement in symptoms, quality of life (QOL), and patient satisfaction, with reduced caregiver burden. Earlier involvement of palliative care also leads to more appropriate referral to and use of hospice, and reduced use of futile intensive care.43
Assessment of palliative care needs should be an ongoing process throughout the course of a patient’s cancer illness and services should be provided on the basis of identified patient need.2
Conclusion
Colorectal cancer is one of Ireland’s most common cancers, affecting thousands of people every year. Patients can reduce their risk of CRC by maintaining a healthy body weight and consuming a diet rich in fibre and less red and processed meat. Healthcare professionals must make every effort to promote CRC screening, which has the potential to prevent CRC and detect it at an early stage in eligible populations.
Stage at diagnosis has a profound effect on survival rates from CRC with five-year survival falling from 95% at stage 1 disease to approximately 12% at stage 4 disease. Family history is important in assessing a patient’s risk of CRC, and the possibility of Lynch syndrome should always be considered where there is a history of multiple cancers in family members, particularly at a young age.
The NCCP has developed a GP Referral Pathway for Suspected Colorectal Cancer that GPs may use to assist them in identifying which patients require referral for endoscopy or to gastroenterology or surgical outpatients.
Following treatment, patients will require surveillance for some time. It is important for GPs to remain alert for potential after-effects of treatment such as urinary symptoms, erectile dysfunction and lower anterior resection syndrome (LARS).
 (click to enlarge)
(click to enlarge)