Long-term physical effects reported by prostate cancer survivors in Ireland
Physical symptoms following prostate cancer are common, often multiple, and persist years after diagnosis, representing a large health burden
Dr Anna Gavin, Director, Northern Ireland Cancer Registry, Northern Ireland, Dr Frances J Drummond, Project Manager, PiCTure Study, National Cancer Registry of Ireland, Cork and Prof Linda Sharp, Professor of Cancer Epidemiology, Newcastle University, UK
Results from the All-Ireland PiCTure (Prostate Cancer Treatment, your experience) study show that the burden of symptoms following prostate cancer treatment is very high; nine out of 10 men reported having at least one of the following: urinary incontinence, impotence, bowel problems, breast changes, loss of libido, fatigue or hot flashes, at some time following treatment. Sixty-one percent reported at least three symptoms; 20% four symptoms; 12.5% five; 6% six, and 2% reported all seven symptoms investigated. The most commonly reported was impotence by two thirds of men (68%), followed by loss of libido (58%) and fatigue (55%) by over half of men, and bowel problems by over a quarter of men (26%). Although many recovered, three out of four men reported having at least one ongoing physical symptom after treatment.
These were just some of the findings of the PiCTure study,1 an all-Ireland research project funded by Prostate Cancer UK (PCUK), the Health Research Board (HRB) and Research and Development office of the Public Health Agency, Northern Ireland. The study examined the effect of prostate cancer investigations, treatment and follow-up on the health of 3,348 men in the Republic of Ireland (RoI) and Northern Ireland (NI).
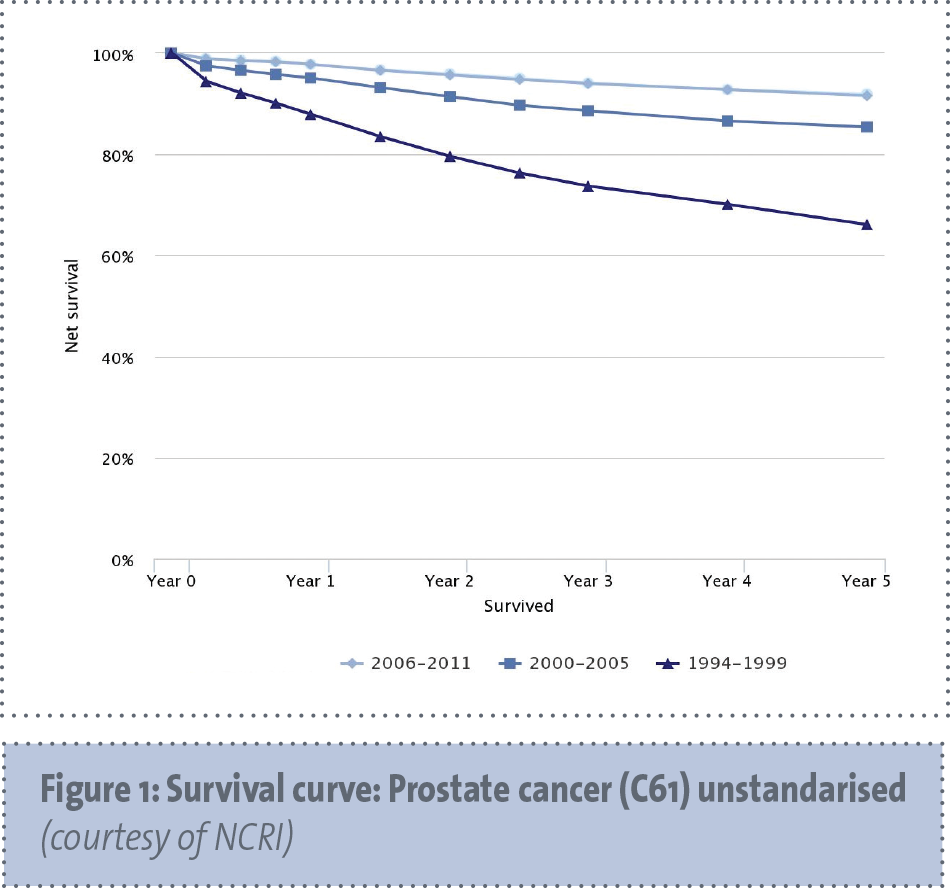
Prostate cancer is now the most frequently diagnosed cancer in males in developed countries,2 with 3,457 cases diagnosed each year in RoI, and 1,047 in NI (2011 figures). Among all of the men living after a cancer diagnosis, prostate cancer is the most common cancer (40% of all male cancer survivors in RoI and 34% in NI). There are a number of prostate cancer treatments, including surgery (radical prostatectomy) radiation (external beam radioactivity, brachytherapy) and active surveillance, which is regular monitoring of men’s PSA levels, with or without prostate biopsy. All prostate cancer treatments carry the risk of both short- and long-term effects including impotence, incontinence, bowel problems, hot flashes and fatigue, which affect men’s health. We wanted to measure these effects in Ireland and, so, collected information from more than 3,000 prostate cancer survivors 2-18 years post-diagnosis.
(click to enlarge)
Symptoms at questionnaire completion
Three-quarters of men reported experiencing at least one ongoing symptom (ie. the symptom was present at the time of questionnaire completion, even though this may have been many years after treatment) with almost one-third (29%) reporting three or more, and 4% at least five symptoms. Almost two-thirds of respondents (65%) reported currently having impotence, urinary incontinence and/or bowel problems, and 57% reported at least one of the following: loss of libido, breast changes, fatigue or hot flashes.
For each symptom, fewer men reported having the symptom currently as opposed to ever (ever was defined as having the symptom at some time after treatment but not at the time of questionnaire completion). The biggest differences were greater for fatigue (ever, 55%; current, 22%), hot flashes (39%, 6%) and urinary incontinence (37%, 16%). The smallest reduction was for impotence (68% versus 57%), which, if present, is less likely to improve than other symptoms. One-quarter of survivors reported no physical symptoms at questionnaire completion. This was most common after brachytherapy treatment (42%). Those treated with brachytherapy also reported lower than average proportions of ongoing impotence (43%), loss of libido (26%), hot flashes (2%), and breast changes (2%).
Overall 45% reported receiving hormone therapy (HT) at some point after diagnosis. Current use of hormone therapy (19% of men) compared to past use (26% of men), and never use (55% of men) was associated with significantly more hot flashes (54% among current users of HT versus 15% among past users of HT versus 4% among never users of HT), loss of libido (62% current HT versus 50% past HT versus 38% never HT), breast changes (23% current HT versus 14% past HT versus 2% never HT) and fatigue (38% current HT versus 23% past HT versus 16% never HT).
We made ‘before’ and ‘after’ treatment comparisons for impotence and loss of libido. Prior to diagnosis, 19% reported impotence and, as expected, this increased with age from 16% of those < 60 years to 21% of men aged >70 years. Impotence as a new ongoing symptom after treatment was reported ‘currently or ongoing’ by 43%, while 5% reported having impotence pre-treatment, but not currently. This varied by primary treatment being highest following prostatectomy at 63%. Loss of libido was reported pre-diagnosis by 15% of survivors; 5% reported this pre-treatment but not currently, and 46% report ‘current’ loss of libido but not pre-treatment.
Ongoing symptoms varied by treatment received. After radical prostatectomy, three-quarters (76%) of men reported ongoing impotence and over one-quarter (28%) experienced ongoing urinary incontinence. These were higher than the average for all respondents while bowel problems (9%), hot flashes (7%) and breast changes (3%), post-radical prostatectomy, were lower than average for this group of men. Men treated with external beam radiotherapy in addition to hormone therapy reported the highest proportions of current bowel problems (20%) compared to men treated with hormone therapy alone (9%), radical prostatectomy (9%), brachytherapy (7%) or observation (active surveillance/watchful waiting; 2%).
Two-thirds of prostate cancer survivors on observation reported no ‘current’ physical symptoms, higher than other groups. The level of libido loss or impotence reported by one in five men was only slightly higher than the pre-treatment average levels. Also other symptoms were less common in the observation group (urinary incontinence (7%), hot flashes (4%), fatigue (4%), bowel problems (2%) and breast changes (2%)) than for any other treatment.
These patterns of side-effects are similar to those reported in other studies. This study was population-based, very large, and included men, whatever their treatments, up to 18 years post-diagnosis; other studies have been much smaller and tended to focus on men undergoing a single form of treatment.
We are fortunate in Ireland to have high-quality cancer registries that organised this study and facilitated population representativeness to be assessed.
We observed that, as with many questionnaire studies, older men were less likely to respond. Also, we recognise that, as prostate cancer treatments have changed over time, investigation patterns and different patient profiles exist with more younger, fitter patients in recent times. We also recognise that accuracy of recall is a potential problem with any study of this type.
While we have documented symptoms reported by prostate cancer survivors, we recognise that not all are caused by prostate cancer treatments, we know for example that erectile dysfunction and urinary incontinence increase with age and that some of the reported physical symptoms may be due to other illnesses, or other treatments.
Implications
International guidelines recommend that survivors and their partners are given opportunities to discuss psychosexual problems and that counselling on sexual problems and urinary incontinence is available as long as needed. Our results suggest there is likely to be a large need for these types of services, with 75% of men reporting at least one physical symptom, almost 60% current impotence and one in six reporting current incontinence.
In conclusion, physical symptoms following prostate cancer are common, often multiple and persist years after diagnosis representing a large health burden. Recognition and treatment of physical symptoms should be prioritised in patient follow-up.
This information will be valuable for men and clinical teams alike for informing prostate cancer treatment decision-making, and also for policy makers assess burden and inform policy to support medium- to long-term prostate cancer survivors.
References
Drummond FJ, Kinnear H, O’Leary E et al. Long-term health-related quality of life of prostate cancer survivors varies by primary treatment. Results from the PiCTure (Prostate Cancer Treatment, your experience) study. J Cancer Surviv 2015; Jan 7: Epub ahead of print.
Siegel RL, Miller KD, Jemal A. Cancer statistics 2015. CA: A Cancer Journal for Clinicians 2015; 65(1): 5-29.
 (click to enlarge)
(click to enlarge)