Gynaecological cancer accounts for more than one in eight cancers arising in Irish women
Dr Noreen Gleeson, Consultant Gynaecologist, St James’s Hospital, Dublin, Dr Aoife Freyne, Specialist Registrar in Obstetrics and Gynaecology, National Maternity Hospital, Dublin and Dr Claire Murtagh, Senior Physiotherapist in Oncology, St James's Hospital, Dublin
According to the National Cancer Registry Report (NCRI 2018), 12.5% of female malignancies are genital tract: body of uterus (4.8%), ovary (3.7%), cervix (2.7%), and others including vulva (1.3%).1 With the exception of ovarian cancer, survival rates for genital tract malignancies are good, and this together with the early median age at diagnosis is reflected in their high ranking of second place with 13,610 (15%), compared to breast cancer at 39,539 (43.6%), in the estimated complete prevalence (90,591) of women living with cancer in Ireland to end of 2016.1
Good survival rates focuses the care of these women on the quality of their survivorship. Cancer-specific impediments to quality of survivorship arise from the disease itself and the adverse sequelae of treatments. Multiple modalities of treatment are often applied to enhance cure rates. Surgery is the mainstay of staging and treatment for most gynaecological cancers and many patients undergo radiation and/or chemotherapy. The lymphatic system is a common site of collateral damage. Lymph flow from lower limbs, vulva and pelvis through the groins and pelvis can be impaired by cancer metastasis or injury arising from these modalities of treatment.
The lymphatic system
The lymphatic circulation is a network of lymphatic vessels of increasing calibre, which withdraw surplus tissue fluid as lymph from the body’s interstitial fluid compartment, filters it through lymph nodes and returns it to the systemic circulation in a low-pressure system. The initial lymph vessels in the dermis, consist of an overlapping single layer of endothelial cells. These drain lymph from the interstitium, when tissue pressure is high, into the low-pressure lymph circulation. The initial lymph vessels, also called collectors, empty into the larger precollectors, in which flow benefits from the proximity to the pulsation and contractility of the arterial circulation.
The precollectors have rudimentary unidirectional valves which aid with lymph drainage to the lymph collectors. Drainage through the lymph collectors is a function of their three-layered structure: intima with its paired valves, media of smooth muscle fibres and adventitia of supportive collagen. Unidirectional flow in the lymph collectors is assisted by pulsations of neighbouring arteries and skeletal muscle contractility. After traversing one or more lymph nodes, lymph enters the larger lymphatic vessels which unite to form the thoracic duct or the right lymphatic duct. Lymph from the abdomen, pelvis and lower limbs enters the venous circulation through the thoracic duct.
Lymphoedema
Lymphoedema is the abnormal accumulation of interstitial fluid and deposition of fibroadipose tissue that results from obstruction to lymph flow.2,3,4,5 In women with genital tract cancer, the lymph flow in previously healthy lymph channels can be impaired by cancer metastases, direct interruption at organ dissection and lymphadenectomy, and also by inflammation induced by radiation and infection. Obesity and other inflammatory conditions compound stasis of lymph.
Localised interruption to flow, typically at the site of lymphadenectomy results in accumulation of fluid as lymphocoeles, also called lymphocysts (but without a true capsule) in the pelvis or groin.6 They can reach a large size and cause compression of adjacent structures or the overlying skin and/or get infected and require intervention by drainage. When the flow impairment is more widespread, the resulting lymphoedema causes varying degrees of cosmetic distortion and dysfunction of the lower limbs, pelvis and vulva.
Prevalence and diagnosis
We estimate that gynaecological cancer accounts for more than 300 new cases of lymphoedema per annum in Ireland because it occurs in 30-70% of these cancers.4,7,8 It may be even more common when full field lymphadenectomy is undertaken as in the traditional surgical approach to cervical and vulval cancers. Radiotherapy induces inflammatory change in and around small vessels that can result in fibrosis and permanent obstruction of lymph flow.
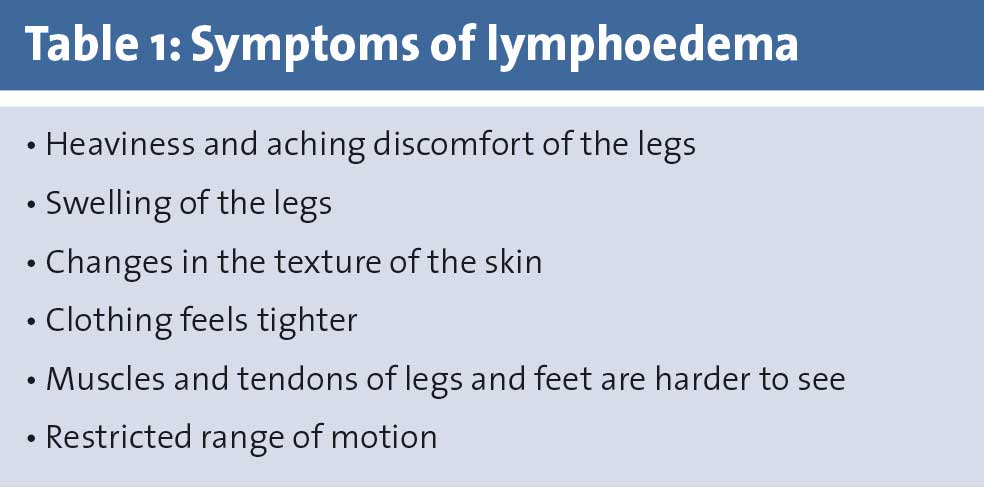
All patients with pelvic cancers and in particular those undergoing surgery and/or radiotherapy for gynaecological cancers should be considered at high risk and earliest possible detection and intervention are recommended in order to minimise the progression of lymphoedema. The onset can be insidious. Symptoms, sometimes unilateral, of skin tightness, swelling, aching pain and restricted movement should be sought (see Table 1).
(click to enlarge)
The physical examination includes general systems, vascular, skin, and soft tissue. Recurrence of cancer should be excluded. At the onset of lymphoedema, swelling in the lower limb or vulva is soft and pitting and reduces with elevation. Pitting reflects movement of the excess interstitial water in response to pressure. Subsequently, the dermis thickens and the skin becomes dry and firm (sclerotic) due to cutaneous fibrosis and adipose deposition.
The overlying skin of the affected limb also becomes thickened and indurated (acanthosis/hyperkeratosis), and verrucous (warty) overgrowth and vesicular (blisters) skin lesions arise. Pachydermous change is irreducible swelling with dry nodular thickening (elephantiasis). Fluid leakage from the vesicular lesions can be very troublesome especially on the vulva.
Stemmer’s sign is a bedside test for lymphoedema. The skin on the dorsal aspect of the proximal phalanx of the second toe is pinched and Stemmer’s sign is positive when the thickened and hardened skin cannot be lifted. A negative Stemmer’s sign does not exclude early lymphoedema.
Chronic venous insufficiency and cardiac oedema enter the differential diagnoses, and venous thromboembolism and recurrence of pelvic cancer may need to be excluded with ultrasound Doppler and CT/MRI respectively.
The diagnosis of lymphoedema is usually clinical. Lymphoscintigraphy is rarely used. CT detects a honeycomb accumulation of fluid within soft tissues and skin thickening. MRI lymphangiography has also been assessed in the evaluation of lymphoedema.9,10,11,12
Objective measurement of limb volume requires assessment by water displacement methods or optoelectronic volumetry, a technique that scans the limb with infrared to calculate the volume. A volumetric difference of 200mL between lower limbs points to lymphoedema in pelvic cancer patients.13,14 Bioelectrical impedance is a new modality that is highly sensitive in the detection of latent or early stage lymphoedema. It measures the body’s resistance to flow of an applied electric current. Bioelectrical impedance reduces the risk of missing early change when intervention can be most effective. Screening with bioelectrical impedance is therefore recommended for high-risk patients.
In the absence of bioelectrical impedance or volumetric equipment, the limb volume can be estimated by taking several circumferential measurements at standard distances. Although there is inherent inter-observer error, simple tape circumferential measurements correlate well with volume measurements. For the lower limbs, measurements at a minimum of four points are recommended, namely at the metatarsal-phalangeal joints (if oedematous), 2cm superior to the medial malleolus, 10cm below the inferior pole of the patella, and 10cm above the superior pole of the patella. A difference of more than 2cm between the affected and contralateral limb is considered clinically significant. Measurement is not possible at the vulva and clinical description has to suffice.
Various grading schemes are described for lymphoedema based on the softness/firmness of skin and limb volume change.15 Lymphoedema of the lower limbs and vulva, results in varying degrees of disruption to cosmesis, mobility, physical, emotional and sexual health.
Cellulitis and lymphangitis can arise with alarming speed especially when there is bullous or papillary change in the skin. In these authors’ experience, lymphoedema of the vulva and mons pubis, even with intact skin, carries a high risk of infection.
The St James’s Hospital Gynaecology Cancer Care team’s grading of lymphoedema reflects the special challenge that vulval and pubic lymphoedema represents (see Table 2). Other grading systems include the staging system of the International Society of Lymphology (ISL), which characterises the severity of lymphoedema (see Table 3), and the Campisi staging system, which determines the disease severity based on how reversible the limb swelling is (see Table 4).
(click to enlarge)
Treatment
High BMI, high fat diet and poor lower limb muscle contractility are reversible risk factors for lymphoedema. Efforts at primary prevention start with optimisation of performance before and during cancer treatment with participation in physical prehabilitation programmes and nutritional advice. Expedient management of their cancers means that women with gynaecological cancers cannot indulge in protracted intervention programmes to reduce obesity, improve nutrition and physical strength but there is often a four- to six-week window from first visit to surgery and pretreatment programming should encourage better lifestyle during and after treatment as well.
Avoidance of dual modality treatment especially surgery and radiotherapy is important and pretreatment and postoperative multidisciplinary discussion of individual cases is essential to ensure that there is a reasonable evidence base for all those prescribed radiotherapy after surgery. Brachytherapy is less likely to induce inflammation in the pelvic sidewall, but patients with confirmed metastases to lymph nodes or other high-risk factors require external beam therapy.
Intraoperatively, the surgeon focuses on minimising disruption to the lymphatic system. Individualising surgical care to avoid unnecessary lymphadenectomy is important. Several multi-centre prospective surgical studies published in the last few years have allowed gynaecological oncologists to moderate their approach to lymhadenectomy.
For squamous cancer of vulva, systematic groin inguinofemoral lymphadenectomy is replaced by sentinel lymphadenectomy with pathological ultrastaging for small volume vulval stage I cancers.7,16,17
For cervix and endometrial cancer para-aortic lymphadenectomy is confined to those at substantial risk of metastases and in the good prognostic groups, sentinel lymphadenectomy is becoming standard of care in selected endometrial and cervical cancers.18,19,20,21,22,23 Systematic pelvic and para-aortic lymphadenectomy in ovarian cancer for patients with no apparent metastasis in the retroperitoneum at the completion of intraperitoneal cytoreduction gives no survival advantage and increases morbidity.24
In the immediate postoperative phase the intermittent compression devices used to prevent venous thrombosis probably enhance lymph flow as well. Physiotherapy to assist mobilisation is essential. The onset of lymphoedema can be insidious, so all women undergoing treatment for endometrial, cervical and vulval cancer should be empowered to identify early symptoms and prevent complications.
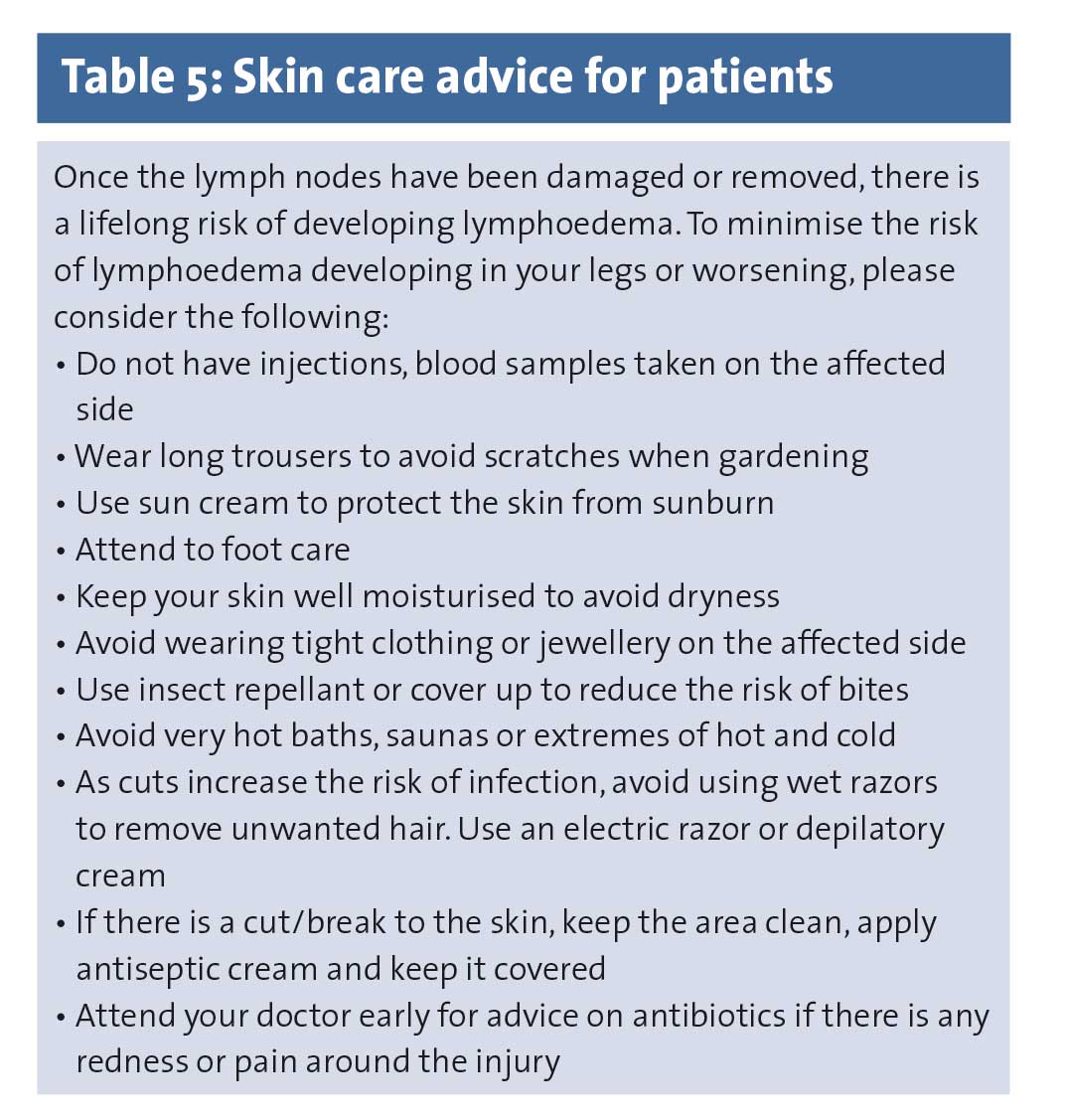
High-grade compression stockings should be prescribed for women at highest risk, for example after inguinal or full pelvic lymphadenectomy and those prescribed radiotherapy after pelvic surgery. Once the lymph nodes have been damaged or removed, there is a lifelong risk of developing lymphoedema (see Table 5).
(click to enlarge)
Treatment of established lymphoedema
At-risk women with symptoms of heaviness in their legs but no measurable increase in diameter and volume should be regarded as having latent lymphoedema. These and any with measurable change should have early intervention to avoid progression to the sclerotic stage. A skilled physiotherapist will massage and teach self-massage, prescribe exercise and fit graded compression stockings.
Manual lymph drainage decongests the lower limb and the risk of re-accumulation of fluid is minimised by high-grade compression garments. Reduction in tissue pressure then improves the efficiency of the muscle and joint pumps.
Patients diagnosed with SJH LE3 stage or higher should be cared for by a specialist lymphologist/physiotherapist. They are at risk of substantial long-term health impairment and cellulitis.
In 2018, an estimated 1,451 patients were admitted to Irish hospitals with cellulitis related to lymphoedema and had an average length of stay of 11 days. Apart from the total cost, estimated at ?13.6 million, each episode of cellulitis is life threatening.25 Patients with sclerotic lymphoedema need manual lymph drainage (MLD) and compression bandaging. MLD is a gentle massage technique that encourages the movement of fluid away from the congested areas by increasing flow through the normal lymphatics, by-passing ineffective lymph vessels.
Complete/compression decongestive therapy (CDT) is an intensive programme that combines manual lymphatic drainage with bandaging; using multilayered padding materials and short-stretch bandages, compression garments, exercise, and self-care. Bandaging loosens the fibrosis and maximises lymph and venous return. Once recovery is achieved bandaging can be alternated daily with compression garments. At present, CDT is offered only by specialist clinics abroad. Pneumatic compression devices are beneficial.
With the support of the St James’s Hospital Foundation, we have purchased compression garments and pumps for application in their own homes for some of our patients with the highest grades of lymphoedema. Full length customised zipped garments extend from toes to groin.
Pressure of 100mmHg is recommended with application for at least one hour per day. Compliance is good, serial EORTC quality of life scoring confirms benefit to all patients and no patient has had a further hospital admission for cellulitis. Peripheral vascular disease (ankle brachial index), recurrent cancer and venous thrombosis should be excluded in all patients prior to commencement of compression treatments (see Pictures 1 and 2).
(click to enlarge)
Surgical interventions for severe lymphoedema aim to restore the lymphatic circulation and excise the excess subcutaneous fibroadipose tissue. Lymph venous bypass and lymph node microsurgical transplantation are described to restore the circulation. Lymph node transplantation is reported to substantially reduce episodes of cellulitis and is supported by a systematic review of 18 studies with a total of 305 patients.26
Lymphovenous bypass procedures, similar to lymph node transplantation, are also effective in patients with early-stage lymphoedema. In a prospective study of 100 consecutive patients, Chang DW et al noted that 96% of patients with upper extremity lymphoedema had symptomatic improvement (lighter, softer, less painful arms) and 74% had quantitative reduction in excess volume.27 Some surgeons combine lymph node transplantation and lymphovenous bypass in an effort to maximise results.
Lymphatic surgery is an evolving field. Its value in women who have undergone irradiation to groins or pelvis remains to be established. Surgical removal by liposuction28,29 or excision30 of subcutaneous fibroadipose tissue may be considered alone or in combination with flow-enhancing techniques.
Low-level laser therapy (also known as cold laser therapy) is a photochemical treatment that may decrease fibrosis, stimulate macrophages and promote lymphangiogenesis. Small trials in upper limb lymphoedema have given conflicting results.31,32,33,34
In conclusion, in the absence of evidence for surgical interventions after radiotherapy, dynamic interventions are still the mainstay of treatment for gynaecological oncology patients with lymphoedema. Short- term use of antihistamines and steroids in selected patients to relieve erythema and pruritus, has also been utilised by some practitioners.2
Lymphoedematous skin is at risk of recurrent infections, including cellulitis, erysipelas, and lymphangitis.35,36,37,38,39,40,41,42 Typical manifestations of infection include erythema, pain, and tenderness. Fever may not be present but prodromal nausea and anxiety are common.
Cellulitis is a complication but also a significant contributor to deterioration in the condition. Severe cellulitis/lymphangitis necessitates immediate hospital admission for intravenous antibiotics and sepsis observation. All episodes should be treated urgently with antibiotics that include gram-positive cocci cover. If patients experience three or more episodes of cellulitis in a year, extended oral antibiotic therapy is considered. The International Society of Lymphology recommends prophylactic penicillin or broad spectrum antibiotic if repeat limb ‘sepsis’ occurs despite optimal CDT.2
Impact on quality of life
In addition, and in part due to physical deformity and disfigurement, lower limb lymphoedema impairs psychological health and quality of life. Emotional, social, sexual and financial wellbeing are compromised.43,44 Psychological support should be provided in parallel with other interventions. The Irish Lymphoedema Society provides guidance and friendship for what can be a socially isolating condition (www.lymphireland.com).
Conclusion
Disability arising from lymphoedema in gynaecological cancer patients is a substantial problem. Screening to detect the earliest signs in at-risk patients needs to be progressed. Dynamic intervention is the cornerstone of treatment at all stages and is likely to be most effective early in the disease process. Expansion of lymphology services is urgently required to address the current major deficiency in this aspect of survivorship in gynaecological cancer care.
References
National Cancer Registry Ireland. Cancer in Ireland 1994-2016 with estimates for 2016-2018: Annual Report of the National Cancer Registry; 2018. NCRI, Cork, Ireland
Executive Committee. The diagnosis and treatment of peripheral lymphedema: 2016 Consensus Document of the International Society of Lymphology. Lymphology 2016; 49(4): 170-84
Brayton KM, Hirsch AT, O Brien PJ, et al. Lymphedema prevalence and treatment benefits in cancer: impact of a therapeutic intervention on health outcomes and costs. PLoS One 2014; 9(12): e114597
Yost KJ, Cheville AL, Al-Hilli MM, et al. Lymphedema after surgery for endometrial cancer: prevalence, risk factors, and quality of life. Obstet Gynecol 2014; 124: 307-315
Kerchner K, Fleischer A, Yosipovitch G. Lower extremity lymphedema update: pathophysiology, diagnosis, and treatment guidelines. J Am Acad Dermatol 2008; 59(2): 324-331
Weingold AB, Marino J. Pelvic lymphocyst: diagnosis and management. Arch Surg 1967; 95(2): 304-307
Gaarenstroom KN, Kenter GG, Trimbos JB, et al. Postoperative complications after vulvectomy and inguinofemoral lymphadenectomy using separate groin incisions. Int J Gynaecol Cancer 2003; 13(4): 522-527
Abu-Rustum NR, Alektiar K, Lasonos A, et al. The incidence of symptomatic lower-extremity lymphedema following treatment of uterine corpus malignancies: a 12-year experience at Memorial Sloan-Kettering Cancer Center. Gynecol Oncol 2006; 103(2): 714-718
Hadjis NS, Carr DH, Banks L, Pflug JJ. The role of CT in the diagnosis of primary lymhoedema of the lower limb. AJR AM J Roentgenol 1985; 144(2): 361-364
Monnin-Delhorn ED. Gallix BP, Achard C, et al. High Resolution unenhanced computer tomography in patients with swollen legs. Lymphology 2002; 35(3): 121-128
Neligan PC, Kung TA, Maki JH. MR Lymphangiography in the treatment of lymphoedema. J Surg Oncol 2017; 115(1): 18-22
Celina M, Oliva G, Menozzi A, et al. Non contrast magnetic resonance imaging lymphangiography: an emerging technique for the study of lymphoedema. Clin Imaging 2019; 53: 126-133
Casley-Smith. Measuring and representing peripheral oedema and its alterations. Lymphology 1994; 27: 56-70
Deltombe T, Jamart J, Recloux S, et al. Reliability and limits of agreement of circumferential, water displacement, and optoelectronic volumetry in the measurement of upper limb lymphedema. Lymphology 2007; 40: 26-34
Campisi C, Campisi C, Accogli S, et al. Lymphoedema staging and surgical indications in geriatric age. BMC Geriatr 2010; 10: 1 A50
Van der Zee AG, Oonk MH, De Hulla JA, et al. Sentinel node dissection is safe in the treatment of early-stage vulvar cancer. J Clin Oncol 2008; 26: 884-889
Grootenhuis NC, Van der Zee AG, Van Doom HC. Sentinel nodes in vulvar cancer: Long-term follow-up of the GROningen INternational Study on Sentinel nodes in Vulvar cancer (GROINSS-V)I. Gynecol Oncol 2016; 140: 8-14
Rossi EC, Kowlaski LD, Scalici J, et al. A comparison of sentinel lymph node biopsy to lymphadenectomy for endometrial cancer staging (FIRES trial): a multicentre, prospective cohort study. Lancet Oncol 2017; 18: 384-392
Ballester M, Dubernand G, Lecuru F, et al. Detection rate and diagnostic accuracy of sentinel-node biopsy in early-stage endometrial cancer: a prospective multicentre study (SENTIENDO). Lancet Oncol 2011; 12: 469-76
Holloway RW, Abu-Rustum NR, Backles FJ, et al. Sentinel lymph node mapping and staging in endometrial cancer: a Society of Gynaecologic Oncology literature review with consensus recommendations. Gynaecol Oncol 2017; 146: 405-15
Cibula D, Abu Rustum NR, Dusek L, et al. Bilateral ultrastaging of sentinel lymph node in cervical cancer: Lowering the false negative rate and improving the detection of micrometastasis. Gynaecol Oncol 2012; 127: 462-466
Lecuru F, mathevet P, Querleu D, et al. Bilateral negative sentinel nodes accurately predict absence of lymph node metastasis in early cervical cancer: results of the SENTICOL study. J Clin Oncol 2011; 29: 1686-91
Rob L, Robova H, Halaska MJ, et al. Current status of sentinel lymph node mapping in the management of cervical cancer. Expert Rev Anticancer Ther 2013; 13: 861-70
Harter P, Sehouli J, Lorusso D, et al. A randomised trial of lymphadenectomy in patients with advanced ovarian neoplasms. N Engl J Med. 2019; 380(9): 822-832
Health Service Executive Policy Document. Lymphoedema and lipodema treatment in Ireland. A model of care for Ireland. A working group report 2018
Ozturk CM, Ozturk C, Glasgow M, et al. Free vascularised lymph node transfer for treatment of lymphoedema. A systematic evidence based review. J Plast Reconstr Aesthet Surg 2016; 69(9): 1234
Chang DW, Suami H, Skorachi R. A prospective analysis of 100 consecutive lymphovenous bypass cases for treatment of extremity lymphoedema. Plast Reconstr Surg 2013; 132(5): 1305-14
Brorson H. Complete reduction of arm lymphoedema following breast cancer surgery. A prospective twenty one year study. Plast Reconstr Surg 2015; 136: 134
Hoffner M, Bagheri S, Hansson E, et al. SF-36 shows increased quality of life following complete reduction of post mastectomy lymphoedema with liposuction. Lymphat Res Biol 2017; 15(1): 87-98
Doscher ME, Herman S, Garfein ES. Surgical management of inoperable lymphoedema, the re-emergence of abandoned techniques. J Am Coll Surg 2012; 215(2): 278-83
Carati CG, Anderson SN, Gannon BJ, et al. Treatment of post mastectomy lymphoedema with low level laser therapy. A double blind, placebo-controlled trial. Cancer 2003; 98(6): 1114-22
Kozanoglu E, Basaran S, Paydas S, et al. Efficacy of pneumatic compression and low level laser therapy in the treatment of postmastectomy lymphoedema: a randomised controlled trial. Clin Rehabil 2009; 23(2): 117-24
Kaviani A, Fateh M, Yousefi Nooraie R, et al. Low level laser therapy in management of post mastectomy lymphoedema. Lasers Med Sci 2006; 21(2): 90-94
Mayia AG, Olivia ED, Dibya A. Effect of low level laser therapy in the management of post mastectomy lymphoedema. Physiotherapy Singapore 2008; 11(1): 2-5
Kerchner K, Fleischer A, Yosipovitch G. Lower extremity lymphoedema update: pathophysiology, diagnosis and treatment guidelines. J Am Acad Dermatol 2008; 59(2): 324-31
Valiant L, Gironet N. Infectious complications of lymphoedema. Rev Med Interne 2002; 23(3): 403-407
Dupuy A, Benchikhi, H, Roujeau JC, et al. Risk factors for erysipelas of the leg (cellulitis) case-control study. BMJ 1999; 318(7198): 1591-4
Herpetz U. Erysipelas and lymphoedema. Fortschr Med 1998; 116(12): 36-40
Masmoudi A, Maaloul I, Turki H, et al. Erysipelas after breast cancer treatment (26 cases). Dermatol Online J 2005; 11(3): 12
Kerketta AS, Babu BV, Rath K, et al. A randomized clinical trial to compare the efficacy of three treatment regimens along with footcare in the morbidity management of filarial lymphoedema. Trop Med Int Health 2005; 10(7): 698-705
Soo Jk, Bicanic TA, Heenan S, Mortimer PS. Lymphatic abnormalities demonstrated by lymphoscintigraphy after lower limb cellulitis. Br J Dermatol 2008; 158(6): 1350-1353
Damstra RJ, van Steensel MA, Boomsma JH, et al. Erysipelas as a sign of subclinical primary lymphoedema: a prospective quantitative scintgraphic study of 40 patients with unilateral erysipelas of the leg. Br J Dermatol 2008: 158(6): 1210-1215
Tobin MB, Lacey JH, Meyer L, Mortimer PS. The psychological morbidity of breast cancer-related arm swelling. Psychological morbidity of lymphoedema. Cancer 1993; 72(11): 3248-52
McWayne J, Heiney SP. Psychologic and social sequelae of secondary lymphoedema: a review. Cancer 2005; 104(3): 457-66
 (click to enlarge)
(click to enlarge)