Chronic Obstructive pulmonary disease (COPD) is a common, preventable and treatable disease, characterised by persistent airflow limitation that is usually progressive. It is associated with an enhanced chronic inflammatory response of the airways and the lung to noxious particles or gases, particularly tobacco smoke. Exacerbations and comorbidities contribute to the overall severity in individual patients.
The chronic airflow limitation characteristic of COPD is caused by a mixture of small airway disease (obstructive bronchiolitis) and parenchymal destruction (emphysema), the relative contributions of which vary from person to person. The terms ‘emphysema’ and ‘chronic bronchitis’ were widely used in the past when describing what is now called COPD. Emphysema, or destruction of the gas-exchanging surfaces of the lung (alveoli), is a pathological term that is often incorrectly used clinically and describes only one of several structural abnormalities present in patients with COPD.
Chronic bronchitis, or the presence of cough and sputum production for at least three months in each of two consecutive years, remains a clinically and epidemiologically useful term. However, it does not reflect the major impact of airflow limitation on morbidity and mortality in COPD patients. Cough and sputum production may precede the development of airflow limitation; conversely, some patients develop significant airflow limitation without chronic cough and sputum production.
Burden of COPD
Ireland has the highest death rate from respiratory disease in the European Union – death rates are over twice the EU average.1 There is widespread under-recognition and under-diagnosis of COPD and it is thought that available data underestimates the burden of respiratory disease in Ireland.
Data from the second INHALE report2 shows that respiratory disease and COPD in particular, has a serious effect on health. In this report in 2008, Ireland had moved from fourth to second place since 2003 in the league of European countries with the highest death rates from COPD. Respiratory illnesses cause one-in-five deaths in Ireland and are still the most common reason for patients to visit their GP.
The report commented that given the prevalence of smoking among young adults, it does not appear likely that mortality from COPD will fall in the medium term. Ireland’s high rates of death from COPD were known as far back as 1989 and this does not seem to be changing. In addition, the report warned that there is evidence that COPD develops earlier than usually believed. Ireland is among five countries where the prevalence of moderate COPD was highest at 5% or more.
In a report on lung disease in Ireland published by the Irish Thoracic Society in December 20133 it was noted that deaths due to chronic lower respiratory disease are likely to be under-represented in statistics as many COPD patients die from cardiac rather than respiratory failure. Mortality rates for COPD are just over 27 per 100,000, with only two European countries with higher rates. Irish hospital admission rates for COPD are 264 per 100,000, whereas the European average is 200.
A major problem with COPD is estimating its real prevalence in the general population, which may considerably change according to the diagnostic tools used, respiratory symptoms reported by the patient, physician’s diagnosis or presence of lung function impairments.
Diagnosis of COPD
Diagnosis of COPD depends on clinical judgement based on a combination of history, physical examination and functional assessment and is confirmed by the presence of airflow obstruction using spirometry.
The new GOLD guidelines on COPD4 recommend that a clinical diagnosis of COPD should be considered in any patient who has dyspnoea, chronic cough or sputum production and a history of exposure to risk factors for the disease.
Assessment of severity
The GOLD guidelines state that assessment is based on:
The patient’s level of symptoms
Future risk of exacerbations
Severity of the spirometry abnormality
The identification of comorbidities.
Assessment of COPD severity is based on the severity of the spirometric abnormality4 and the patient’s level of symptoms as assessed by the Modified British Medical Research Council (mMRC) dyspnoea scale.5
Another useful tool is the COPD assessment test (CAT score).6 The CAT is an eight-item measure of health status impairment in COPD. It correlates very closely with health status measured using the St George Respiratory Questionnaire (SGQR), and is reliable and responsive.
The test is simple to perform and in most instances can be done by the patient themselves following instructions. It is a useful tool for discussion between the doctor and the patient and can help identify where COPD is having the greatest effect on the patient’s daily life. It is complementary to the spirometry in helping to produce a clinical assessment.
(click to enlarge)
Measurement of airflow limitation (spirometry)
Spirometry is an objective measure of how an individual inhales and exhales air as a function of time and is the gold standard for diagnosing, assessing and monitoring COPD.
Whereas spirometry has previously been used to support a diagnosis of COPD, the January 2014 GOLD guidelines now state that spirometry is required to make a confident diagnosis.4 The presence of a post-bronchodilator FEV1/FVC < 70% confirms the presence of persistent airflow limitation and thus of COPD.
Spirometric classification of airflow limitation
GOLD 1: Mild COPD. Individual may not be aware that his/her lung function is abnormal. Mild airflow limitation (FEV1/FVC < 70%; FEV1 ≥ 80% predicted) and sometimes, but not always chronic cough and sputum production
GOLD 2: Moderate COPD. Patients typically seek medical attention at this stage because of chronic respiratory symptoms or an exacerbation of their disease. Worsening airflow limitation (FEV1/FVC < 70%; FEV1 50-80% predicted), with shortness of breath typically developing on exertion
GOLD 3: Severe COPD. Further worsening of airflow limitation (FEV1/FVC < 70%; FEV1 30-50% predicted), greater shortness of breath, reduced exercise capacity, and repeated exacerbations which have an impact on a patient’s quality of life
GOLD 4: Very severe COPD. At this stage, quality of life is very appreciably impaired and exacerbations may be life-threatening. Severe airflow limitation (FEV1/FVC < 70%; FEV1 < 30% predicted or FEV1 < 50% predicted plus chronic respiratory failure).
The latest guidelines say that use of the fixed ratio (FEV1/FVC) may lead to more frequent diagnoses of COPD in older adults with mild COPD, but underdiagnosis in people under 40. The concept of staging based on FEV1 has been abandoned, as using this alone was inadequate and there isn’t another evidence-based system.
Management strategy
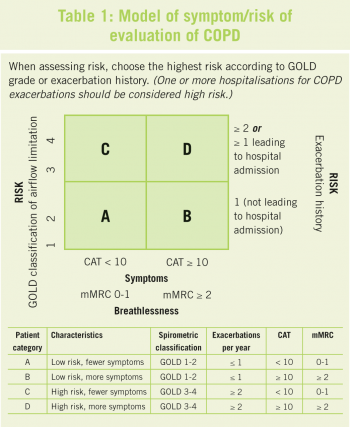
The evidence for pharmacological treatment of COPD had in the past been based mostly on the severity of airflow limitation (FEV1 as percentage predicted). However, the 2014 guidelines stressed: “The level of FEV1 is an inadequate descriptor of the impact of the disease on patients.” Therefore, individualised assessment of symptoms and future risk of exacerbation should be incorporated into the management strategy (see Table 1).
Symptoms
There is no evidence-based division between low versus high level of symptoms. Typically, the patient with a high level of symptoms will have activity-limiting breathlessness, mMRC2 and/or trouble walking two flights of stairs, or a CAT score > 20.
Risk
Similarly, there is no clear evidence-based division between low versus high risk. Typically, the patient with high risk will have frequent exacerbations (two or more per year), FEV1 < 50% predicted, poor health status and a history of heartburn.
The impact of COPD on an individual patient depends not just on the degree of airflow limitation, but also on the severity of symptoms. There is an imperfect relationship between the degree of airflow limitation and the presence of symptoms.
Recommendations
COPD should be considered in any patient who is > 35 years, has dyspnoea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease. COPD should also be considered in:
Patients who present with respiratory symptoms who smoke should be offered smoking cessation advice
The diagnosis requires spirometry for confirmation
The presence of a post-bronchodilator FEV1/FVC < 70% and FEV1 < 80% predicted confirms the presence of airflow limitation that is not fully reversible
Assessment of COPD severity is based on the patient’s level of symptoms, the severity of the spirometric abnormality and the presence of complications
There is no need to perform spirometry more often that every 24 months
Measurement of arterial blood gas tensions should be considered in all patients with FEV1 < 50% predicted or clinical signs suggestive of respiratory failure or right heart failure
COPD is usually a progressive disease and lung function can be expected to worsen over time, even with the best available care. Symptoms should be monitored to determine when to modify therapy and to identify any complications that may develop
Comorbidities are common in COPD and should be actively identified. Comorbidities often complicate the management of COPD, and vice versa.
Care of patients with COPD
Once COPD has been diagnosed, effective management should be aimed at goals based on an individualised assessment of disease to reduce current symptoms and future risk. These goals should be reached with minimal side-effects from treatment, a challenge in COPD patients because of comorbidities.4 Ongoing monitoring should ensure that treatment goals are being met.
The overall approach to managing people with stable COPD should be guided by the following general principles:
Determine disease severity on an individual basis by taking into account the patient’s symptoms, airflow limitation, frequency and severity of exacerbations, complications, respiratory failure, comorbidities, and general health status. The level of FEV1 is a poor descriptor of disease status and for this reason the management of stable COPD based on a strategy considering both symptoms and future risk is recommended
Implement a stepwise treatment plan that reflects this assessment of disease severity.
Smoking cessation
Smoking cessation has the greatest capacity to influence the natural history of COPD. Identification and reduction of exposure to risk factors are important in the treatment of COPD.
Nicotine replacement therapy in any form (eg. nicotine gum, inhaler, nasal spray, transdermal patch, sublingual tablet or lozenge) reliably increases long-term smoking abstinence rates. Pharmacological support from agents such as bupropion and varenicline can significantly aid smoking cessation quit rates.
Vaccines
Influenza vaccines can reduce serious illness such as the risk of hospitalisation due to lower respiratory tract infections and death in COPD patients. Influenza and pneumococcal vaccination are given as per the National Immunisation Guidelines. The regular use of antitussives and the use of mucolytic agents are not recommended.
Patient education
Patient education can play a role in improving skills, ability to cope with illness and health status. Ideally, educational messages should be incorporated into all aspects of care and in all settings from the first assessment and continuing with each follow up visit for COPD.7
Topics should include information about the nature of COPD, advice about reducing risk factors, recognising symptoms and early exacerbation interventions and coping skills including specific information on treatment options as disease severity increases. The intensity and content of these educational messages should vary depending on the severity of the patient’s disease.
Each patient should have a self-management plan with advice on how to prevent exacerbations and actions in the event of one occurring.7
Pharmacological treatment
Pharmacological therapy is used to prevent and control symptoms, reduce the frequency and severity of exacerbations, improve health status, and improve exercise tolerance. Existing medications for COPD do not modify the long-term decline in lung function that is the hallmark of this disease. The GOLD 2014 guidelines offer a model for pharmacological management based on the individualised assessment of symptoms and exacerbation risk (see table 2).
Treatment should be cumulative with more medications required as the disease state worsens. Regular treatment needs to be maintained at the same level for long periods unless significant side-effects occur or the disease worsens.
Individuals differ in their response to treatment; careful monitoring and support is needed over an appropriate period to ensure that the specific aim of introducing a therapy has been met without an unacceptable cost to the patient.
(click to enlarge)
Early pulmonary rehabilitation
Ideally, rehabilitation should be offered at time of diagnosis. This should be as early as possible in disease severity.
COPD patients at all stages of disease appear to benefit from pulmonary rehab programmes, improving with respect to both exercise tolerance and symptoms of dyspnoea and fatigue. The principal goals of pulmonary rehabilitation are to reduce symptoms, improve quality of life and increase physical and emotional participation in everyday activities. To accomplish these goals, pulmonary rehabilitation covers a range of non-pulmonary problems that may not be adequately addressed by medical therapy for COPD; exercise de-conditioning, relative social isolation, altered mood states (especially depression), muscle wasting and weight loss.
Pulmonary rehabilitation has been carefully evaluated in a large number of clinical trials and is shown to increase exercise capacity, reduce dyspnoea and improve quality of life. Benefits have been reported from rehabilitation programmes conducted in inpatient, outpatient and home settings. Considerations of cost and availability most often determine the choice of setting.
The minimum length of an effective rehabilitation programme is six weeks; the longer the programme continues the more effective the result. However, as yet, no effective programme has been developed to maintain the effects over time. Pulmonary rehab improves exercise capacity and reduces the perceived intensity of breathlessness. It reduces hospitalisations, improves recovery if hospitalisation is necessary and improves survival. It can enhance the effects of long-acting bronchodilators. Patients unable to participate in a structured programme can be advised to exercise on their own (eg. walking 20 minutes daily). It is recognised that patients who exercise more post-exacerbation of COPD do better.
The components of pulmonary rehabilitation vary widely but a comprehensive programme includes exercise training, smoking cessation, nutrition counselling and education.
Nutritional state is an important determinant of symptoms, disability, and prognosis in COPD; both overweight and underweight can be a problem. A reduction in body mass index is an independent risk factor for mortality in COPD patients.
References
National Respiratory (COPD) Framework 2008. Irish Thoracic Society/HSE/ICGP
INHALE Report 2nd Edition 2009. A compilation of statistical data by Dr Niall Brennan, Suzanne McCormack and Dr Terry O’Connor
Lung disease in Ireland – Prevalence and Trends: Implications for workforce planning. Irish Thoracic Society 2013
GOLD Guidelines. Global strategy for the diagnosis, management and prevention of COPD. (Updated 2014)
Modified British Medical Research Council Dyspnoea Scale. Fletcher CM et al. The significance of respiratory symptoms and the diagnosis of chronic bronchitis in a working population. British Medical Journa1959
www.CATestonline.org
COPD management - quick reference guide. Joint initiative of the ICGP Quality in Practice Committee and the Irish Thoracic Society. 2009
 (click to enlarge)
(click to enlarge)
