Pain is both a symptom and a disease. As a symptom, acute pain is often difficult to treat due to the coexistence of comorbidities, and chronic pain is now recognised as a disease. As early as in 2001, the European Federation of IASP Chapters (EFIC) declared chronic pain as a disease in its own right. It explained that while acute pain acts as a warning system and alerts the patient to danger and the need to seek help; chronic pain can persist long after the tissue damage has healed.1
Acute pain is usually related to an injury or illness whereas chronic pain often has no clearly identifiable cause. In these instances, chronic pain may not directly relate to the initial disease or injury but to secondary changes, including changes to the physiology and pathophysiology of the pain process. Unrelieved or undertreated, severe acute pain is a major predictor for chronic pain and for associated reduction in quality of life.
Consequences of unrelieved acute pain
Unrelieved pain can result in a range of adverse consequences including poor sleep, reduced mobility with subsequent loss of strength, and sometimes to anxiety and depression. It can also impair the immune system and subsequently lead to an increased susceptibility to infection. Above all, if moderate to severe pain is unrelieved it can lead to changes in the nervous system and to chronic pain syndromes.2,3,4
The mechanisms underlying the progression from acute to chronic pain are related to peripheral and central sensitisation.5 Trial data is limited but most of the evidence is derived from laboratory or epidemiological data. Initiation of peripheral and central sensitisation is most likely when a patient is ‘primed’ by intense pain, a genetic predisposition or a psychological state.6
Inflammation at the site of tissue damage and ectopic discharges after nerve injury lead to a barrage of pain signals that can produce changes to the peripheral nerves, spinal cord, higher central pain pathways, somatosensory cortex and the sympathetic nervous system.
Once sensitisation has become established, chronic pain develops and the patient experiences allodynia (pain in a non-painful area) and hyperalgesia (excessive pain) which lowers the pain threshold. Psychological factors such as depression, psychological vulnerability and stress can be triggers in the development of chronic pain.
Pain assessment
Assessing pain is essential in the process of diagnosing the cause of the patient’s discomfort, selecting appropriate analgesia, evaluating and then modifying the treatment plan according to the patient’s response. Pain is subjective and sometimes very difficult to assess. However, the gold standard is what the patient says it is. McCaffrey in 1968 wrote: “Pain is whatever the experiencing person says it is, existing whenever the experiencing person says it does”.7 This definition reflects the move away from the biomedical model towards recognising the psychological and social aspects affecting pain, seeing the patient as a person with their own voice.
It recognises the association between psychological factors such as heightened anxiety, catastrophising, depression and stress and disability at later points in time.4 Psychiatrist George Engel (1977) proposed the biopsychosocial model which incorporated the physiological, psychological and environmental factors that impinge on a patient’s pain and focuses on rehabilitating and improving their quality of life.8
Assessing acute pain
Assessment begins with a thorough medical history, a pain history and a general examination. The mnemonic ‘OLD CART’9 (onset, location, duration, characteristics, aggravating/relieving factors, treatment) and ‘SOCRATES’10 (site, onset, characteristics, radiation, alleviating, timing, exacerbating, and severity) have been used for years to guide acute pain assessment.
Consideration is given to pain intensity (at rest and on movement), location of the pain, temporal characteristics such as the pattern of the pain, and whether it is ongoing, intermittent, worst in the mornings or evenings. The assessment should monitor the aggravating and relieving factors, and whether treatment is effective.
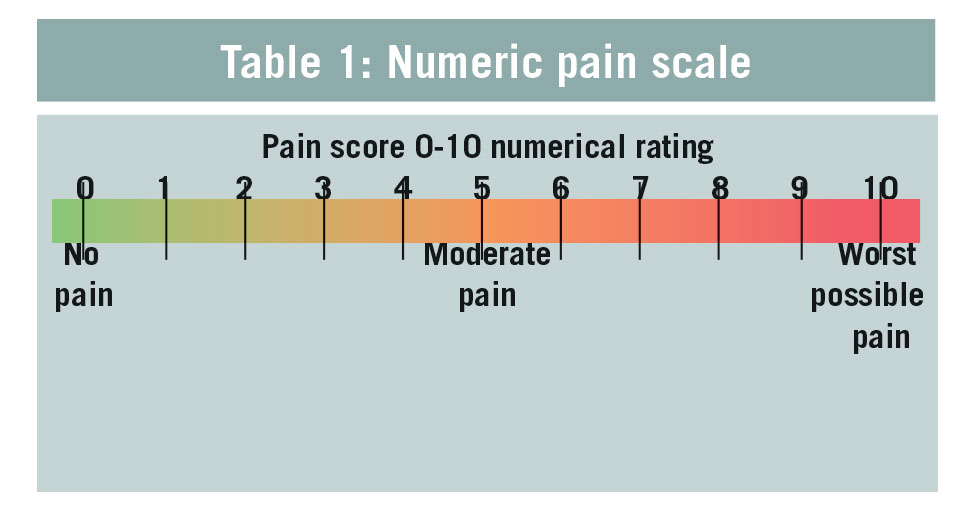
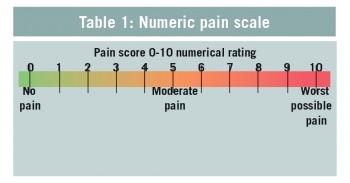
Measuring pain aims at giving a numerical value to the patient’s subjective experience of the pain intensity and the associated distress. The numeric pain scale is a universal tool through which the patient can score their pain between 0 and 10 with verbal descriptors (see Table 1).11
(click to enlarge)
In 1999, the American Veterans Health Administration launched the ‘Pain as the fifth vital sign’ toolkit to improve pain management among health professionals, requiring a pain intensity rating (0-10) at all clinical encounters.12 It was a controversial move at the time in the US as many clinicians were not educated in pain management; and patients demanded their pain to be immediately and permanently relieved.
The analogy of insulin administered to treat blood glucose was applied to the practice of treating pain with opioids until the pain was gone.13 This resulted in large-scale use of opioids that has left its own legacy of addiction problems.
When performing a clinical examination, it is important to diagnose if there is nociceptive pain, neuropathic pain or both. Nociceptive pain can be somatic (musculoskeletal) or visceral; somatic pain arises from the skin, muscles, bones, joints, or connective tissue. It is described as sharp, hot, stinging and is generally well localised, with tenderness in the surrounding tissues.
In contrast, visceral pain is derived from the internal organs and may be described as dull, crampy, colicky pain that is less localised. It is often associated with referred pain and can be accompanied by nausea, sweating and cardiovascular changes.
Neuropathic pain is caused by abnormal signalling in the peripheral or central nervous system, caused by trauma, inflammation, metabolic conditions (diabetes), infections (herpes zoster), tumours, toxins, and primary neurological diseases. It becomes a chronic disease when pathophysiological changes arise independent of the inciting event and sensitisation occurs.
Neuropathic pain may be continuous or episodic and is felt in different ways; burning, tingling, prickling, shooting, electric shock-like, spasm or cold. Sensory deficits such as numbness, dysesthesias and paraesthesias (unpleasant sensations at rest, movement or following touch) can co-exist with abnormally painful conditions such as allodynia and hyperalgesia.
Assessment of pain in older patients with cognitive impairment
In the early stages of dementia, the patient may be able to verbally report pain. However, as the dementia progresses pain is often under-recognised and under-managed, which can lead to sleep disturbances, weight loss and depression. With cognitive impairment, pain is often manifested as agitation, confusion, decreased mobility with a much-reduced quality of life.
PAINAD (PAIN in advanced dementia) is a commonly used observational behavioural pain tool that monitors five items: breathing, negative vocalisation, facial expression, body language and consolability. Each of these five items are scored 0, 1, or 2, out of a total of 10 on the pain scale.14 PAINAD is only a tool to aid assessment, other ways include asking a close relative or carer for their opinion.14,15 Also, it can be assumed that if they have any underlying conditions such as arthritis, then they are more likely to suffer pain. If all this fails, administer appropriate analgesia and observe their behaviour and determine if they appear calmer.
Assessment of pain in babies, toddlers and young children
If pain is not treated quickly and effectively in children, it can cause long-term physical and psychological sequelae. Pain assessment should involve a clinical interview with the infant/child, parent, physical assessment and the use of an age-appropriate pain intensity measurement tool. In neonatal intensive care it was found that facial expression in response to pain was more reliable than physiological measures but may be dampened among pre-term neonates.16,17
Behavioural assessment tools provide additional support for the use of behavioural observations in quantifying pain in infants. However, behavioural distress unrelated to pain may also be identified by observational tools. In these cases, careful consideration should be taken in relation to the context of the behaviours.
Pain assessment for neonates and infants to two months
Premature infants have a limited ability to display and maintain behavioural or physiological manifestations of pain. The Neonatal Infant Pain Scale (NIPS), however, is specifically formatted for newborn infants and is based on five behavioural and one physiological indicator. Assessed in the NIPS tool are facial expression, cry, movements of arms and legs, state of arousal and breathing patterns.18,19,20
Pain assessment for infants at two months to seven years, and for children 4-18 years with cognitive impairment
The FLACC observational tool is validated for children from two months to seven years, and from 4-18 years in children with cognitive impairment.21 It is a useful behavioural pain assessment tool for children unable to self-report their pain. It observes facial expression; legs; activity; crying and consolability. FLACC has been found to be a reliable tool that is simple to follow.
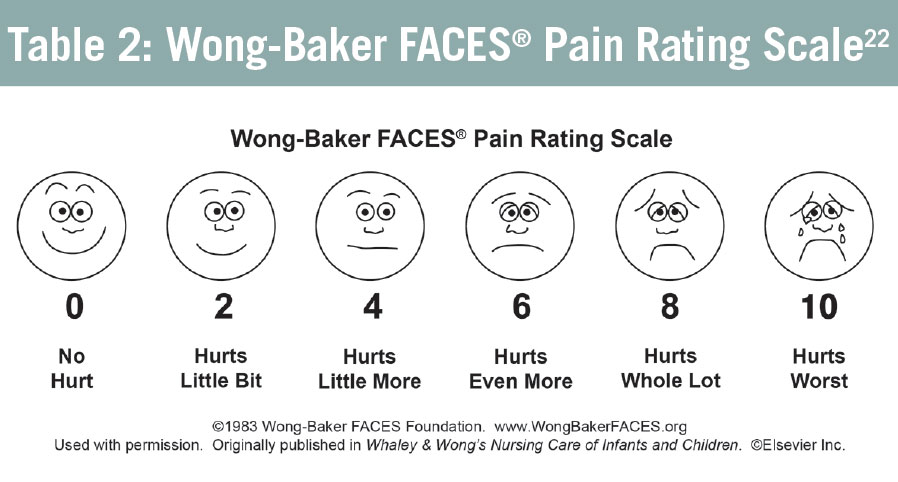
Pain assessment for children from 3 years and into adulthood
Using the Wong-Baker FACES® Pain Rating Scale,22 a child is asked to select one of six neutral faces that accurately reflect their pain, which is scored from 0 to 10 (see Table 2).
(click to enlarge)
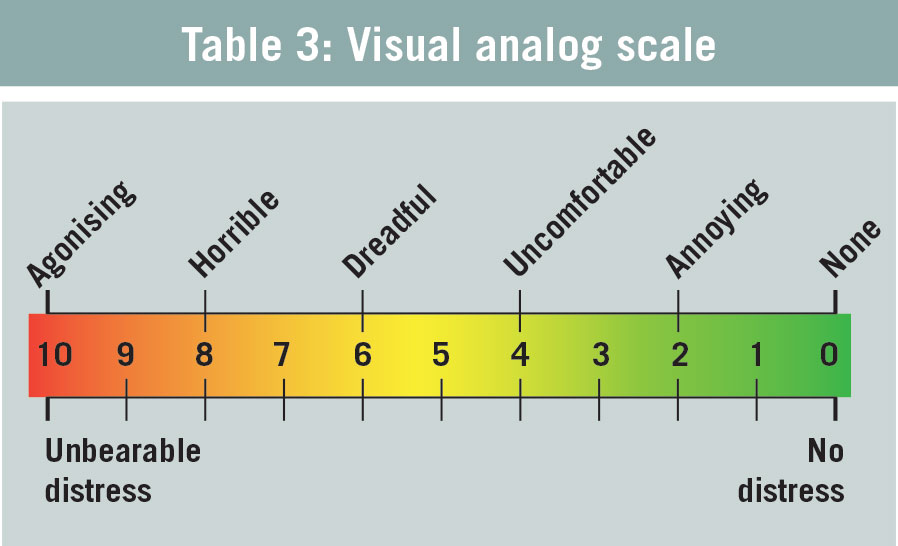
Pain assessment for children from 8 years
Older children (> 8 years of age) who are able to understand abstract concepts can use the visual analog scale (VAS, see Table 3)23 and the 0-10 numeric rating scale (NRS).11 The child makes a mark on the line to indicate his/her level of pain.
(click to enlarge)
Managing acute pain
Multimodal analgesia was introduced more than a decade ago to improve the management of pain. The rationale is that the additional or synergistic effects of different analgesics, used in combination, delivers better pain control. By using smaller doses, the risk of developing side-effects is reduced.
Historically, opioids were the mainstay of pain management but with the increasing knowledge of pain mechanisms, dependence on them has been reduced. Newer medications are gaining a prominent role in controlling severe acute and chronic pain.
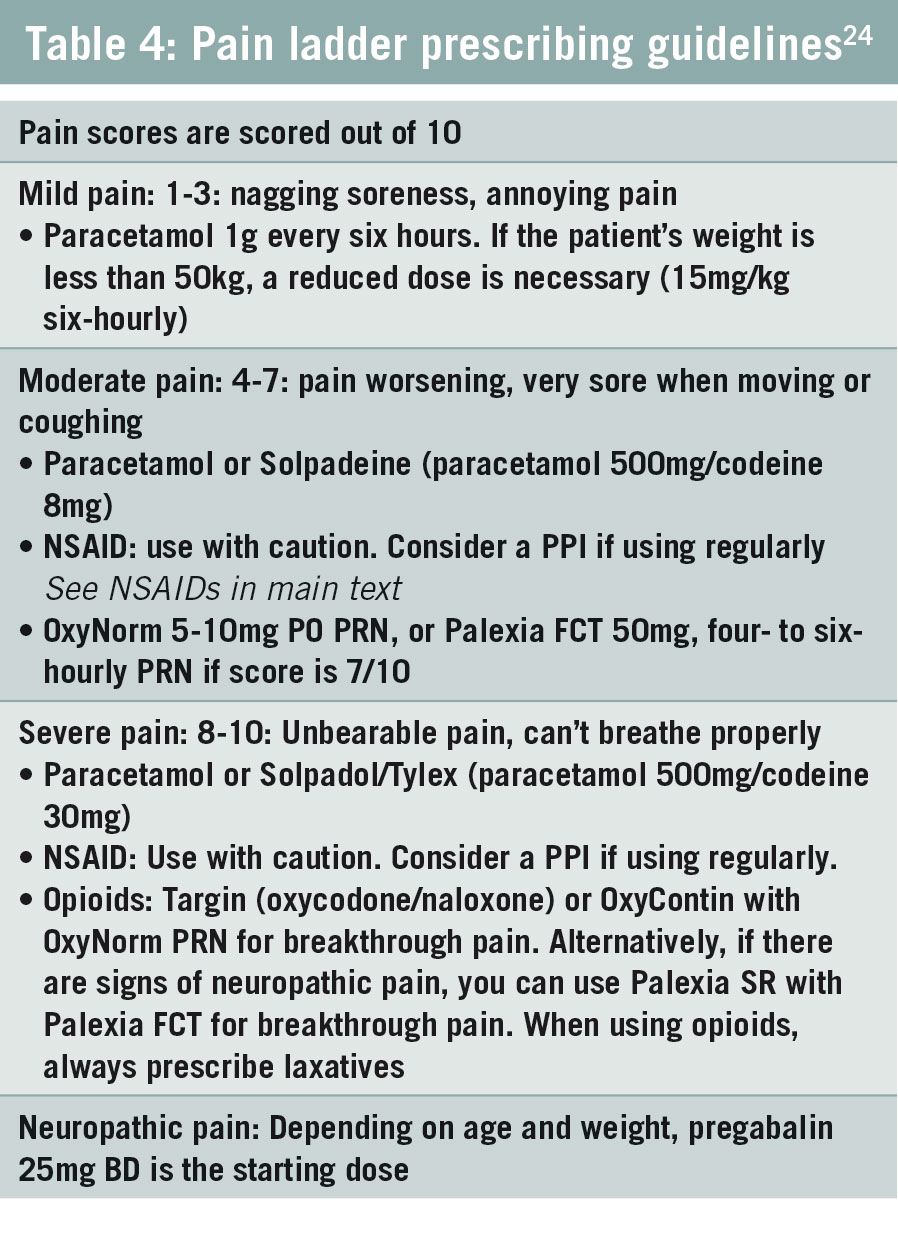
When deciding on appropriate therapy, several factors should be considered, such as comorbidities, recent therapy, potential risks and side-effects and the patient’s own preferences (see Table 4 for St Vincent’s University Hospital pain ladder prescribing guidelines).24
(click to enlarge)
Paracetamol
If the patient’s weight is over 50kg, then the maximum daily dose of paracetamol is 4g. The maximum daily dose is 3g for patients:
With a body weight less than 50kg; the dose is 15mg/kg six-hourly
With hepatic impairment (chronic cirrhosis, chronic malnutrition, dehydration)
On enzyme-inducing drugs.
If the creatinine clearance (GFR) is less than 30mL/min, give the dose appropriate for the patient’s weight with a minimum interval of six hours, and not four.
Bear in mind that pain relieving medication such as Solpadeine contains paracetamol 500mg + codeine 8mg (paracetamol 1g + codeine 16mg) and Solpadol/Tylex contains paracetamol 500mg + codeine 30mg (paracetamol 1g + codeine 60mg).
Non-steroidal anti-inflammatory drugs (NSAIDs)
When prescribing an NSAID the following should be considered (NICE 2013)25:
If the person is already taking an NSAID, such as over-the-counter aspirin or ibuprofen
Whether an alternative to an oral NSAID is appropriate, eg. paracetamol or codeine for analgesia; a topical NSAID for localized analgesia; physiotherapy
Renal impairment: NSAIDs inhibit prostaglandins (PGE2 and PG12). Inhibition of these prostaglandins may result in sodium retention, reduced renal blood flow and renal failure26
Pregnancy: All NSAIDs are contraindicated from 28 weeks gestation because of the risk of premature closure of the ductus arteriosus or decreasing amniotic fluid27,28,29,30
Currently active asthma. Unless NSAIDs clearly cause severe exacerbations of asthma, people with asthma should not be denied the benefits of NSAIDs without being offered the option of a trial to assess the effect on asthma control
Hepatic impairment: Liver fibrosis, cirrhosis, variceal bleeding, hepatorenal syndrome and encephalopathy. Severe liver impairment is when the liver enzymes levels are more than three times the upper limit of the normal range and the serum albumin is less than 25g/L
Ischaemic heart and cardiovascular disease: NSAIDs can cause inhibition of COX-2 which can lead to a significant risk for thrombotic and cardio- and cerebrovascular events31
An inflammatory bowel condition such as Crohn’s, ulcerative colitis, diverticulitis
If the patient has a history of mild GORD, they may need a proton pump inhibitor (PPI) in accordance with NICE 2013 guidance32
If there are potentially hazardous interactions with other drugs such as thiazide-type diuretics, selective serotonin reuptake inhibitors (SSRIs), and warfarin
Review patients currently prescribed NSAIDs. If continued use is necessary, consider changing to ibuprofen (1,200mg per day or less) or naproxen (1,000mg per day or less)
The European Medicines Agency undertook a review (June 2013) of systemic diclofenac and found adverse effects on the heart and circulation similar to those of selective COX 2 inhibitors (etoricoxib, celecoxib)33
Diclofenac is contraindicated for elderly patients with congestive cardiac failure, ischaemic heart disease, peripheral arterial disease or cerebrovascular disease
The risks of adverse effects vary among individual NSAIDs, depending on the dose and duration of use. Adverse effects may be minimised by using the lowest effective dose for the shortest duration necessary to control the symptoms.
The 2007 Oxford league table sets out analgesic efficacy of the commonly used and newer analgesics for acute pain.34 Numbers needed to treat are calculated for the proportion of patients with at least 50% pain relief over four to six hours compared with placebo in randomised, double-blind, single-dose studies in patients with moderate to severe pain. This is based on the use of oral analgesics except IM morphine. This is a detailed table and can be accessed at several sources, including www.bandolier.org.uk
The Pharmaceutical Society of Ireland has highlighted safety issues around the misuse of non-prescription products containing codeine and in particular combination products, where codeine is used with another analgesic. Guidance was issued to pharmacists in 2010.35 These products should not be accessible to the public for self-selection without the input of a pharmacist and should be displayed out of public view.
Medicines with codeine should not be used for longer than three days without medical supervision. Pharmacists are advised to refer patients in the first instance to their GP or an addiction outreach worker if they become aware of abuse of codeine medications.
Prescribing opioids36
The role of opioids for severe and cancer pain is well established. However, opioid use for chronic non-cancer pain remains controversial.
Opioid tolerance occurs when increasing amounts of opioids are required to produce the same level of effectiveness.
Addiction is a form of psychological dependence and refers to extreme behaviour patterns associated with obtaining and consuming opioids. Withdrawal symptoms include dysphoria (agitation), anxiety, volatility of mood and physical symptoms such as hypertension, tachycardia and sweating.
Opioid induced hyperalgesia (OIH) is a condition where high doses of opioids cause more pain than relief and a decreased pain threshold. Reductions of dosage may be appropriate in the elderly and in patients with chronic hepatic disease, renal impairment, severe hypothyroidism, adrenocortical insufficiency, prostatic hypertrophy, shock or where sedation is undesirable.
Slow release opioids should not be given to patients with an ileostomy as they can pass into the stoma bag unabsorbed.
Always prescribe laxatives when using opioids to prevent constipation.
Opioids are recommended for moderate to severe pain. It is important that the patient’s baseline opioid dose is maintained before acute pain can be treated.
From the hospital to the community – a case study in pain control
Lilly is a 31-year-old woman who presented at a GP clinic having been discharged four days previously from hospital following a small bowel resection for a stricture arising from Crohn’s disease. While in hospital, she suffered a wound infection and required daily dressings initially, but now it is every second day. She has a temporary loop ileostomy and is well able to manage the stoma bag. She is anaemic with a haemoglobin of 9.5 and a white cell count of 18.5, CRP is 430, down from 680 prior to discharge.
Lilly is very distressed and is feeling very low. She had been doing well enough to be able to hold down her job but is afraid she may not be able to continue. She has good family support and has a boyfriend who appears to be committed to her. The main reason why Lilly is attending her GP is to help manage her pain.
Prior to surgery Lilly was opiate naïve, but now her postoperative pain is not well controlled. In the hospital the junior doctor prescribed fentanyl 200µg lozenges for the dressings as they were particularly painful. She found them very effective and is now looking for a prescription for more.
Her behaviour is very persuasive and she becomes tearful when discussing her pain. She is adamant that she needs the fentanyl to be able to function and implores her GP for the prescription, even for just one month.
Medication on discharge from hospital:
Antibiotics: metronidazole + ciprofloxacin
Immune system suppressor: adalimumab
Steroids: prednisone (on a tapering dose post-op)
Analgesia: OxyContin 15mg BD with OxyNorm 5-10mg PO every four hours if needed. Paracetamol 1g every six hours.
Discussion
Lilly is only 31, therefore she should not be on opioids for long. Once she has recovered from the postoperative acute pain, they should be stopped.
As Lilly has an ileostomy, the chances are high that the OxyContin tablet is passed into the stoma bag and is not being absorbed fully. Instead of using a slow-release opioid, use an immediate release formulation such as OxyNorm or Palexia FCT instead. This way the chance of her absorbing the opioid is greater.
She was prescribed fentanyl lozenges for the dressings. Fentanyl is 100 times more potent than morphine and should not be used for someone who is young and vulnerable to developing chronic pain. Instead, OxyNorm PO, or Palexia PO, could be given 30 minutes prior to the dressing as they are less potent than fentanyl. If the opioids are ineffective, check for neuropathic pain and treat accordingly.
It is imperative that Lilly comes off the opioids as soon as possible. Once the pain improves, she could use a paracetamol 500mg/codeine 30mg combination for a short period of time as she comes down off the opioids and she should them be moved onto a paracetamol 500mg/codeine 8mg combination. Do not prescribe additional paracetamol with the combination prescription.
Never prescribe NSAIDs for any inflammatory bowel disease as it can trigger a flare up.
References
EFIC’s declaration on chronic pain as a major healthcare problem, a disease in its own right, 2001. As accessed on: https://s3.amazonaws.com/rdcms-iasp/files/production/public/Content/ContentFolders/GlobalYearAgainstPain2/20042005RighttoPainRelief/painasadisease.pdf
Latremoliere A and Woolf CJ. Central Sensitization: A Generator of Pain Hypersensitivity by Central Neural Plasticity. The Journal of Pain, 2009: 10; 895-926
Schug SA, Pogatzi-Zahn EM. Chronic pain after surgery or injury. IASP Clinical Updates 2011; 19(1)
Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J. (2015) Acute pain management: scientific evidence, fourth edition. Med J Aust 2015; 204(8): 315-317
Baron R, Hans G, Dickenson AH. Peripheral input and its importance for central sensitisation. Ann Neurol 2013;74(5):630-6
Lavand’homme P. The progression from acute to chronic pain. Curr Opin Anaesthesiol 2011; 24(5): 545-50
McCaffery M. (1968) cited in Mc Caffery M, Beebe A, Latham J, Ball D. (eds) Pain: Clinical Manual for Nursing Practice. London and St Louis, MO: Mosby
Engel GL. “The clinical application of the biopsychosocial model”. American Journal of Psychiatry. 1980; 137(5): 535-544
Seidel HM, et al. Mosby’s Guide to Physical Examination. Mosby: St Louis, 2003
Clayton Holly A (2000) ‘Socrates on Pain Assessment’. Med Surg Nursing. Retrieved 2008-03-31.
www.physio-pedia.com
Veterans Health Administration National Pain Management Strategy. 1998. November 12, 1998. https://www.va.gov/PAINMANAGEMENT/docs/Pain_As_the_5th_Vital_Sign_Toolkit.pdf
Onieal ME. The Paradox of Pain Management. Clinician Reviews. 2016; 26(11): 12-16
Warden V, Hurley AC, Volicer L. Development and psychometric evaluation of the Paqin Assessment inAdvanced Dementia (PAINAD) Scale. Journal of the American Medical Directors Association. 2003; 4: 9-15
www.dementiapathways.ie
Slater R, Cantarella A, Franck L, et al. How well do clinical pain assessment tools reflect pain in infants? PLoS Med 2008; 5(6): e129
Stevens B, Franck L, Gibbins S, et al. Determining the structure of acute pain responses in vulnerable neonates. Can J Nurs Res 2007; 39(2): 32-47
Sarhangi F, Mollahadi M, Ebadi A, Matinzadeh ZK, Tadrisi SD. Validity and reliability of Neonatal Infant Pain Scale in Neonatal Intensive Care Units in Iran (2010). Pak J Med Sci 2011; 27(5):1087-109
Suraseranivongse S, Kaosaard R, Intakong P, Pornsiriprasert S, Karnchana Y, Kaopinpruck J, Sangjeen K. A comparison of postoperative pain scales in neonates. British Journal of Anaesthesia 2006; 97(4): 540-4
Lawrence J, Alcock D, McGrath P, Kay J, MacMurray SB, Dulberg C. The development of a tool to assess neonatal pain. Neonatal Netw. 1993; 12(6): 59-66
Merkel S, et al. The FLACC: A behavioral scale for scoring postoperative pain in young children. Pediatr. Nurse 1997; 23(3): 293-297
Wong-Baker FACES Foundation (2018). Wong-Baker FACES Pain Rating Scale. Retrieved on April 25, 2018 with permission from
www.WongBakerFACES.org
Visual Analog Scale: Pasero C & McCaffrey M (2011) Pain assessment and pharmacologic management. P 55, St Louis, Mosby
Pain Ladder developed at St Vincent’s University Hospital for an Acute Pain app, called ‘Appease’, available at the app store
NICE guidelines on NSAIDs. www.nice.org
Neal MD, Brown JB, Moore EE, Cuschieri J, Maier RV, Minei J, et al. Pre-hospital Use of Non-Steroidal Anti-inflammatory Drugs (NSAIDs) is Associated with a Reduced Incidence of Trauma-Induced Coagulopathy. Annals of surgery. 2014; 260(2): 378-382.
UKTIS. UK Teratology Information Service. www.uktis.org
Nakhai-Pour HR, Broy P, Sheehy O, Bérard A. Use of nonaspirin nonsteroidal anti-inflammatory drugs during pregnancy and the risk of spontaneous abortion. CMAJ (Canadian Medical Association Journal) 2011; 183: 1713-20
Nielsen GL, Sørensen HT, Larsen H, Pedersen L. Risk of adverse birth outcome and miscarriage in pregnant users of non-steroidal anti-inflammatory drugs: population based observational study and case-control study. BMJ 2001; 322: 266-70
Edwards DR, Aldridge T, Baird DD, Funk MJ, Savitz DA, Hartmann KE. Periconceptional over-the-counter nonsteroidal anti-inflammatory drug exposure and risk for spontaneous abortion. Obstet Gynecol 2012; 120: 113-22
Varga Z, Sabzwari S, Rafay A, Vargova V. Cardiovascular Risk of Nonsteroidal Anti-Inflammatory Drugs: An Under-Recognized Public Health Issue. Muacevic A, Adler JR, eds. Cureus. 2017; 9(4):e1144. doi:10.7759/cureus.1144
NICE Guidance on GORD and Dyspepsia. www.nice.org.uk
www.ema.europa.eu
2007 Oxford league table, as accessed on http://www.bandolier.org.uk/booth/painpag/Acutrev/Analgesics/lftab.html
Non-prescription medicinal products containing codeine: Guidance for phamacists on safe supply to patients. Pharmaceutical Society of Ireland. 2010
British College of Anaesthetists, Faculty of Pain Medicine website www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware
 (click to enlarge)
(click to enlarge)