A 34-year-old male presented with a swollen and bruised left ankle following injury while playing football the day before. The patient was limping as he entered the assessment room. He described how his foot landed atop the football in a dorsiflexed and inverted position in an attempt to bring it under control. He did not report hearing any ‘pop’ or ‘click’, or experiencing any tearing sensation. He was able to weight-bear immediately after the incident. Self-treatment before presentation consisted of oral NSAID and the application of an ice-pack.
He had no previous history of similar injury or recurrent sprains, no disorder predisposing to ligament hyperlaxity or poor sensorimotor control, nor foot/ankle biomechanical abnormality. He was not taking any regular medication and had no known drug allergies. His past medical history included a left-sided pneumothorax secondary to left chest trauma sustained during a football match one year previously. On examination there was obvious swelling and ecchymoses predominantly on the lateral aspect of the left ankle. There was some slight sub-malleolar tenderness laterally on palpation. There was no appreciable movement of the forefoot relative to the ankle on ‘Anterior Drawers Test’, nor notable discomfort on ‘Talar Tilt’.
Furthermore, ‘squeeze’ and ‘external rotation stress’ were both negative, suggesting the absence of syndesmotic (ie. high ankle) sprain. Joint range-of-movement (ROM) was not significantly impaired and there was no distal neurovascular compromise. The patient was sent for plain film radiograph of his ankle, which did not reveal any fracture or abnormality, was advised on early treatment following a ‘Rest Ice Compression Elevation’ (RICE) protocol, followed by graded rehabilitation, and prescribed a short course of non-steroidal anti-inflammatory medication.
(click to enlarge)
(click to enlarge)
Background
Ankle injuries are very common, with an estimated incidence of one in 10,000 individuals per day.1 Ankle sprains are the most common pathology, although a fracture prevalence of 15% has been reported,2,3 presenting the GP or alternative first-line clinician (eg. emergency physicians) with the diagnostic dilemma of identifying such cases. In the past, routine x-ray of the joint, often unnecessarily, formed part of the diagnostic approach. Moreover, the diagnostic process is compounded by subjective elements of history and physical examination in ankle injury, eg. presence of swelling, bruising, ability to plantar or dorsiflex against resistance, etc.2
In their 2011 review, Seah and Mani-Babu4 reported that while ankle sprains occur commonly, their management is not always readily agreed upon. They examined the evidence supporting the use of clinical decision rules and assessment instruments applicable to ankle sprain, and found that although two higher quality studies were identified, most studies ranged between levels three and five on the hierarchy of evidence. They concluded that the strength of recommendation for putting this evidence into clinical practice was limited. However, they noted that the Ottawa Ankle Rules (OAR) were ‘ubiquitous in the clinical pathway’ and could be reliably applied by GPs, emergency doctors and triage nurses.
Wynn-Thomas et al5 measured and validated the baseline use of OAR by GPs in a retrospective cross-sectional survey. Their study showed 100% sensitivity for the diagnosis of fractures using OAR and specificity of 47%. In comparison, the sensitivity of GPs’ clinical judgement was 100% and the specificity was 37%. In this study, implementing OAR in the decision pathway would have reduced XR utilisation by 16%, suggesting that the OAR is valid for use in a primary care setting.
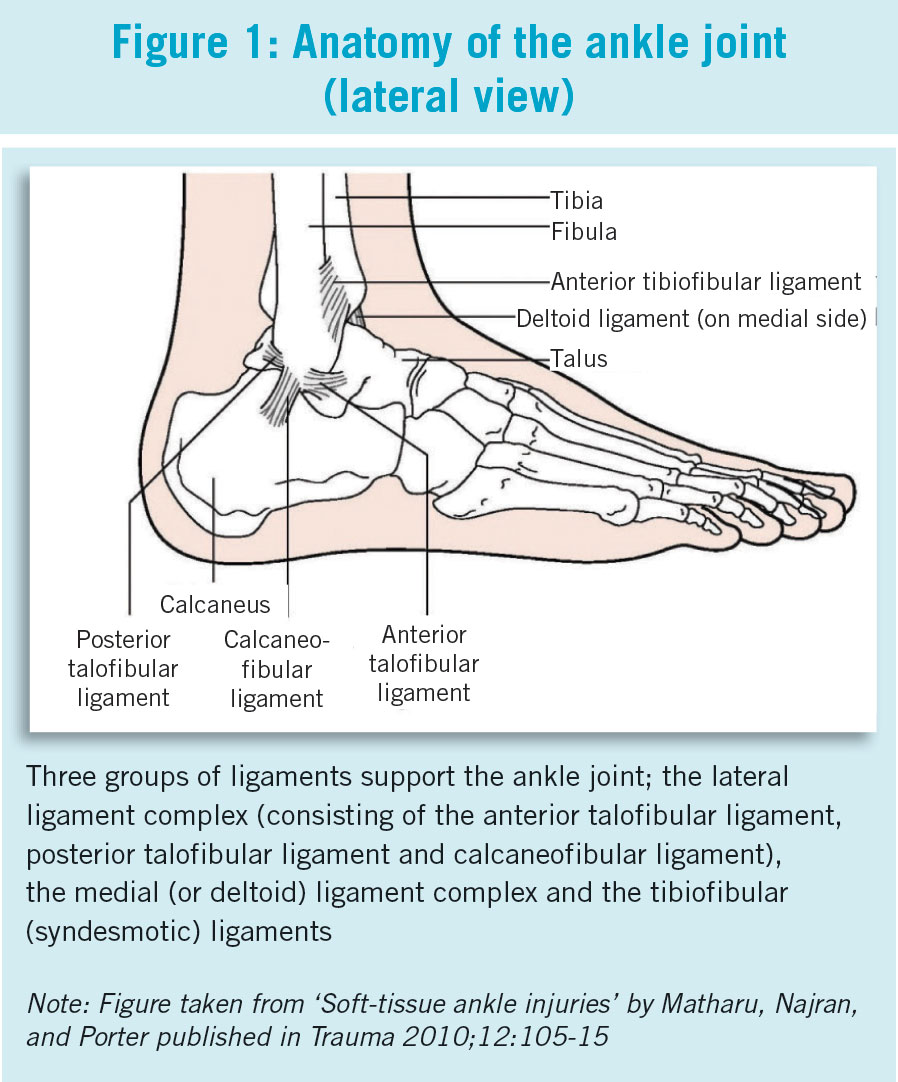
Anatomy recap
A brief review of ankle anatomy is useful when considering potential sprain injuries. The ankle joint is supported by three ligament complexes: the medial (deltoid) ligament complex, the lateral ligament complex and the tibiofibular (syndesmotic) ligaments. The lateral ligaments account for 85% of ankle sprain injuries and reflect their relative weakness compared to the medial side.1 Lateral ligament complex injuries comprise approximately one quarter of all sporting injuries.4 The typical mechanism of injury is falling onto a plantar-flexed, inverted ankle. Medial ligament injury in isolation represents 5% with syndesmotic sprains affecting the anterior tibiofibular and posterior tibiofibular ligaments accounting for 10%.
In the former, the mechanism of injury is usually a forceful and abrupt eversion and rotation, and can often be associated with malleolar fracture; whereas ankle eversion and dorsiflexion, coupled with tibial internal rotation is implicated in the latter.
Grading of ankle sprains
Ankle ligament sprains are usually graded on the basis of severity:
• Grade I – Mild stretching of the ligament complex without joint instability
• Grade II – Partial rupture of the ligament complex with mild instability
• Grade III – Complete rupture of the ligament complex with joint instability.
However, clinically grading can be subjective and often is in the acute setting in the absence of radiological investigations.
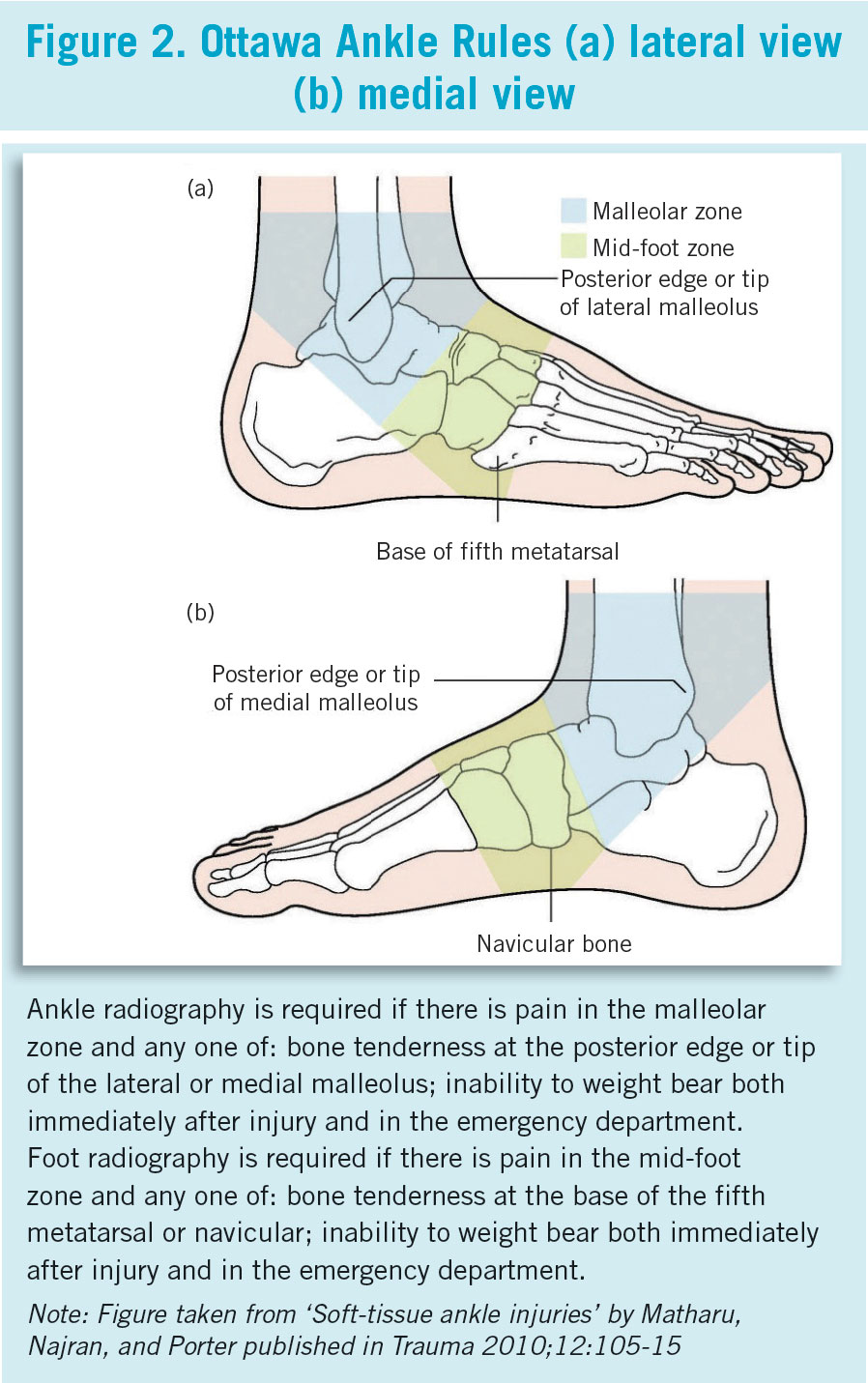
The Ottawa Ankle Rules
In 1992, the University of Ottawa evaluated clinical findings in ankle and mid-foot injury and developed a now well-validated clinical decision aid for suspected fractures. The Ottawa Ankle Rules (OAR) state that ankle x-ray is only necessary if there is any pain in the malleolar zone AND any one of the following:
• Bone tenderness along the distal 6cm of the posterior edge of the tibia or tip of the medial malleolus or
• Bone tenderness along the distal 6cm of the posterior edge of the fibula or tip of the lateral malleolus or
• An inability to bear weight both immediately and in the emergency department for four steps.
In addition, a foot x-ray series is indicated if there is any pain in the mid-foot zone AND any one of the following:
• Bone tenderness at the base of the fifth metatarsal (for foot injuries) or
• Bone tenderness at the navicular bone (for foot injuries) or
• An inability to bear weight both immediately and in the emergency department for four steps.
A negative result on applying these rules means an x-ray is not required.
Overview of evidence
Having reviewed the evidence for management of ankle sprains, Seah and Mani-Babu4 noted only conservative treatments, consisting of immobilisation, functional interventions – eg. elastic bandaging, soft casting, etc and supervised rehabilitation programmes, currently had good evidence for placing into clinical practice. For interventional treatment, the authors felt restricted in meaningfully commenting on the evidence strength owing to small study numbers and questionable quality evidence in one of the implicated reviews. They said therapeutic hyaluronic acid injection of the ankle may have a role in expediting return to sport, although further research is needed. The authors believe there is a role for surgery in severe acute and chronic ankle injuries, but current evidence is limited.
Conservative management
Most treatment focuses on pain control and reduction of swelling, followed by early restoration of movement. After implementation of the RICE protocol and analgesia, management can be divided into conservative and surgical. The latter is not considered here. Delayed examination and reassessment three to five days after injury is recommended where pain and swelling hinder accurate initial assessment.
Functional treatment approaches were shown to be statistically superior to immobilisation for multiple outcome measures for mild-to-moderate ankle sprains.4 For severe cases, a short course immobilisation in a below-knee cast or pneumatic brace resulted in quicker recovery than tubular compression bandage alone.4 Lace-up supports are a more effective functional treatment than elastic bandaging, resulting in less persistent swelling over the short term in comparison with semi-rigid ankle supports, elastic bandaging and tape.4
Beneficial ankle support can be provided by semi-rigid orthoses and/or pneumatic braces and may prevent subsequent sprains in high-risk sporting settings. A combination of supervised rehabilitation and conventional treatment for acute lateral ankle sprain can be beneficial, although further research is required. If pain persists, ligament laxity remains, or where severe pain occurs on ligament stress, consider orthopaedic specialist review.
 (click to enlarge)
(click to enlarge)