The waiting list of patients for a specialist appointment in public hospital services has increased over the past decade. In Ireland, hospital waiting lists continued to rise despite tens of millions of euro pumped into the health system to reduce delays.1
According to the National Council for the Blind of Ireland (NCBI), currently the longest waiting list for outpatient appointments and surgery is in ophthalmology.2 The latest figures show that in February 2017, almost 34,000 people were waiting for outpatient ophthalmology appointments and 3,898 of these had already been waiting for at least 18 months.2
According to NCBI chief executive Chris White: “It is clear that ophthalmology waiting lists are out of control and this is even more shocking when you consider that as much as 75% of sight loss is avoidable.”2 This means that people are dealing with vision loss that may have been prevented if they were diagnosed early and had timely access to treatment. Such evidence would strengthen the need to develop more nurse-led ophthalmic services that will help reduce the growing waiting list in the health service.
Nurse-led corneal crosslinking service
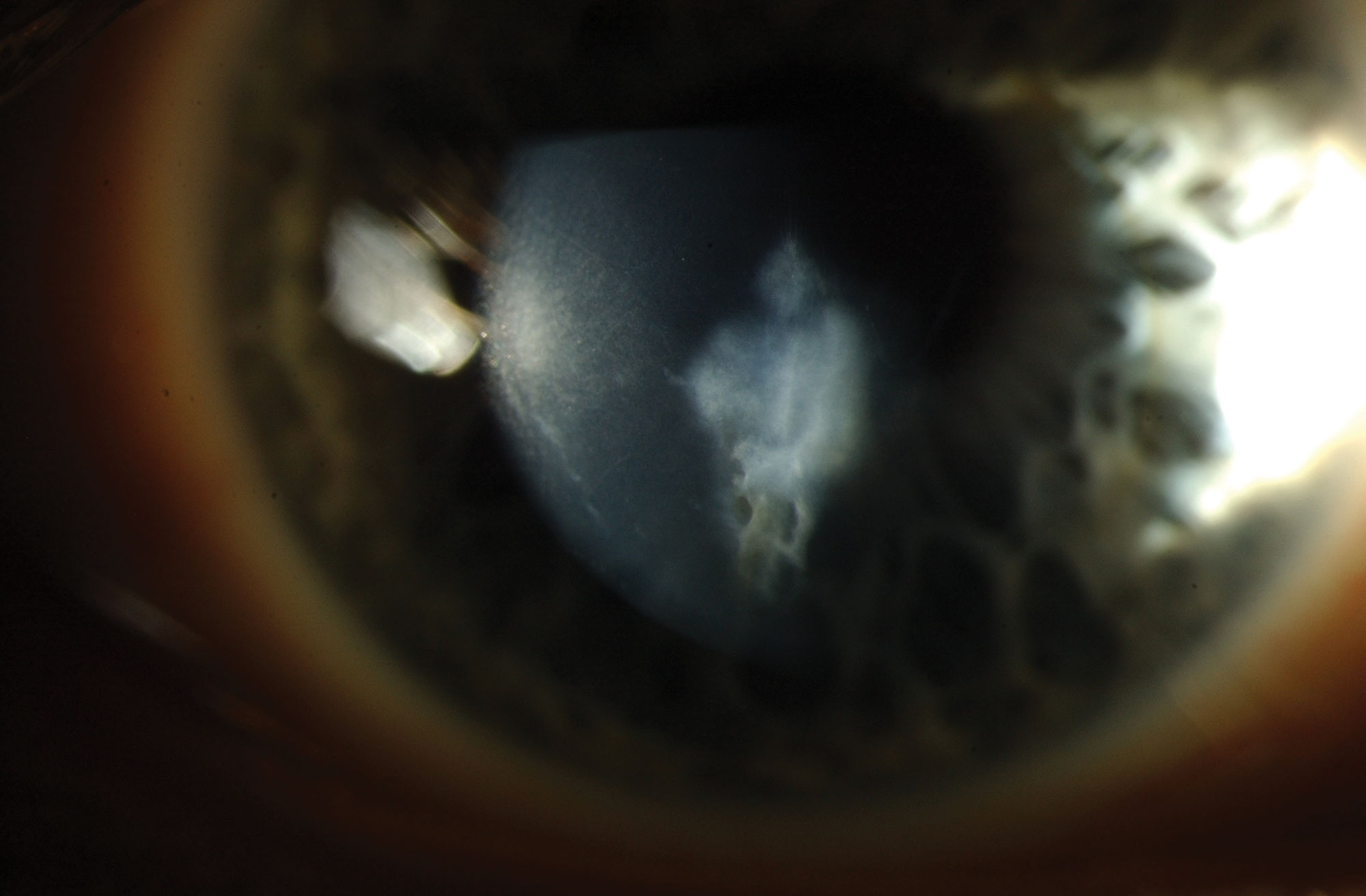
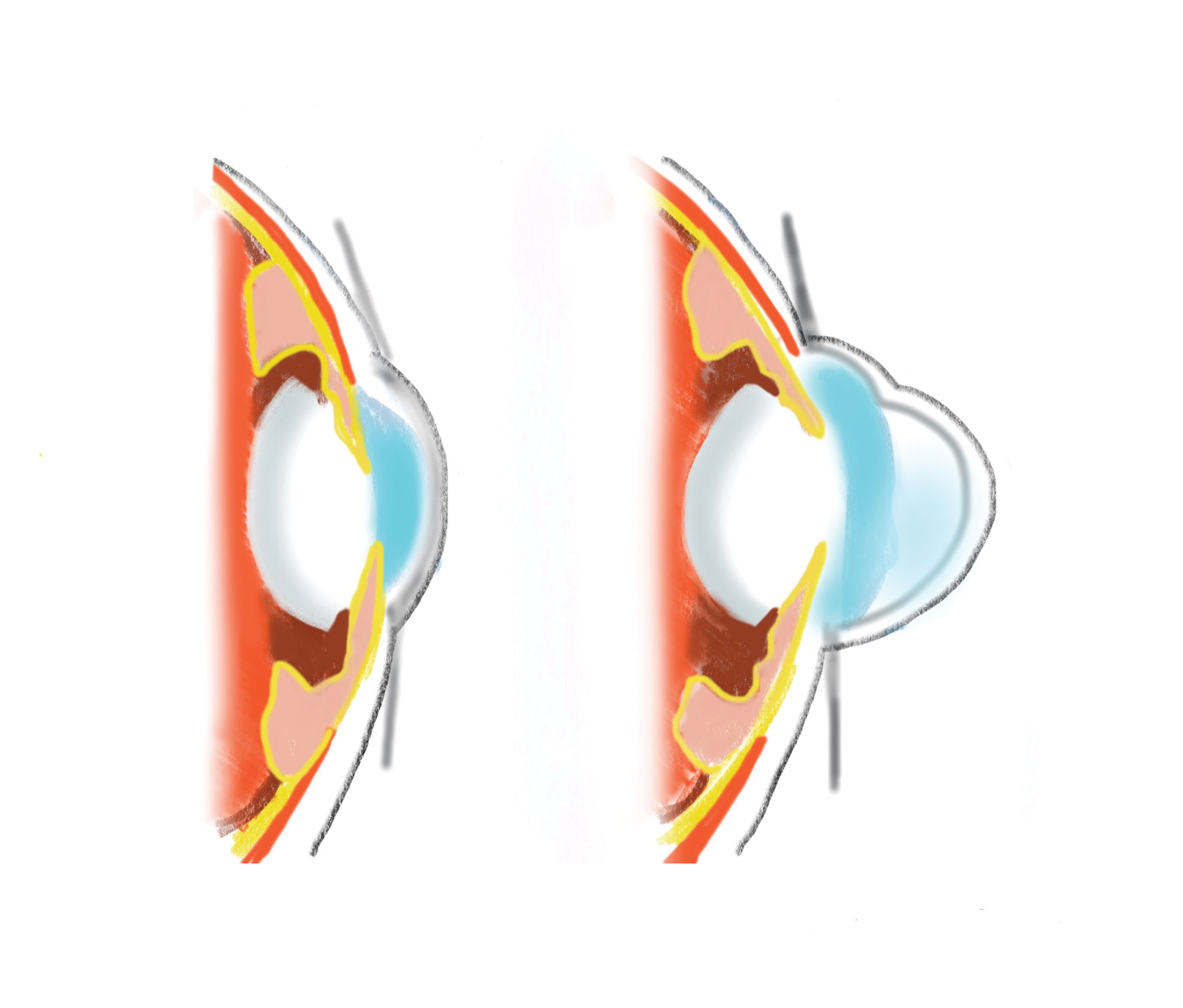
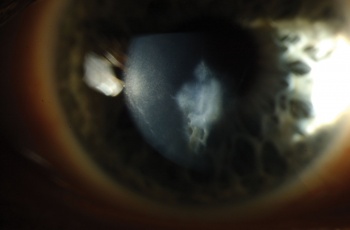
Corneal crosslinking (CXL) is a treatment for keratoconus, a non-inflammatory eye condition in which the normally round dome-shaped cornea progressively thins causing a cone-like bulge to develop.3 The image below shows a corneal scar in advanced keratoconus.
(click to enlarge)
In keratoconus, eye rubbing, genetic predisposition and poorly fitted contact lenses cause eye bulging which results in astigmatism, blurry vision and increased sensitivity to light.4 It typically begins in the teens or 20s (age group: 10-44), and if not diagnosed early could result in significant visual dysfunction, reduced quality of life and permanent changes in lifestyle.5
Before CXL, there were no interventions available to arrest or slow disease progression and corneal transplantation was required in up to 25% of keratoconic eyes.6 As soon as keratoconus is detected, at as young as 10 years of age, CXL is recommended to prevent vision loss.5
Early detection of keratoconus using topography screening has become the norm, resulting in many countries almost eliminating the need for corneal transplantation due to advanced keratoconus.5 Therefore, early diagnosis is essential and timely access to CXL treatment is necessary to stop the progression of keratoconus and to achieve better visual outcomes.
The Royal Victoria Eye and Ear Hospital (RVEEH) through the years has pioneered nurse-led services in ophthalmology. In January 2016, with the collaboration of ophthalmologists and ophthalmic nurses in RVEEH who were open to innovation in ophthalmic services, the first nurse-led CXL service in Ireland started in RVEEH.
Five CXL procedures were observed before starting the training programme. Some 20 CXL procedures were done under supervision on February 23, 2016.
The nurse-led CXL service has its own cohort of patients whereby the nurse assesses, obtains consent, performs the surgical procedure and prescribes medication.
Objectives
The main objective of this study was to explore the impact of the nurse-led CXL service on patient care. The study investigated patients’ acceptability and satisfaction with the nurse-led ophthalmic service, its impact on reducing patient waiting time for treatment and patient stay in the hospital, its safety and cost-effectiveness.
Methodology
A retrospective chart review was performed in January 2017 to assess the result of the nurse-led CXL service. Medical charts of patients who were treated in the nurse-led CXL service from January 2016 to December 2016 were reviewed. A sample of 128 eyes from 100 patients was chosen for this study. Data on post-operative outcome, patient waiting time for CXL and patient stay in the hospital during CXL treatment were collected and analysed.
To compare the waiting time before the nurse-led CXL service, 20% of the 119 eyes treated with CXL from January 2014 to December 2014 were randomly selected. Information on patient waiting times for treatment and patient stay in the hospital was collected and analysed.
A patient satisfaction survey was carried out among patients who were treated in the nurse-led CXL service. The survey was conducted by telephone. This is to assess patients’ acceptability and satisfaction with the nurse-led CXL service. The Likert-type scale was used for seven statements to assess satisfaction with the nurse-led service and one question was used to determine patient preference in terms of practitioner.
A medical student from the Royal College of Surgeons in Ireland (RCSI) surveyed the patients to avoid bias. The aim of the study was explained to the respondents and informed consent was obtained verbally. Patients’ responses were entered into a database spreadsheet and analysed.
Findings
Patient satisfaction
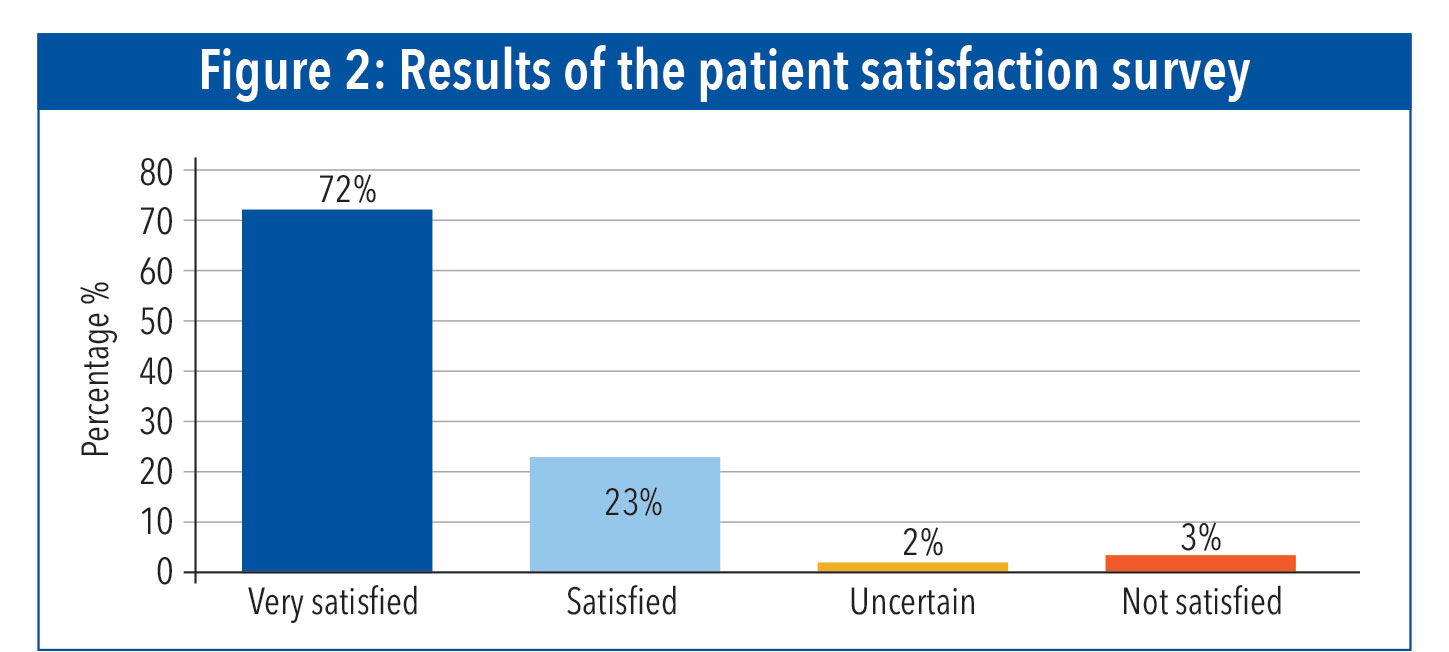
Some 95 patients participated in the telephone patient satisfaction survey. Results showed that 72% of patients were very satisfied with the nurse-led CXL service, 23% were satisfied, 2% uncertain, and 3% were not satisfied – although in all of these cases the dissatisfaction arose from delays in receiving follow-up appointments rather than the procedure itself (see Figure 1).
(click to enlarge)
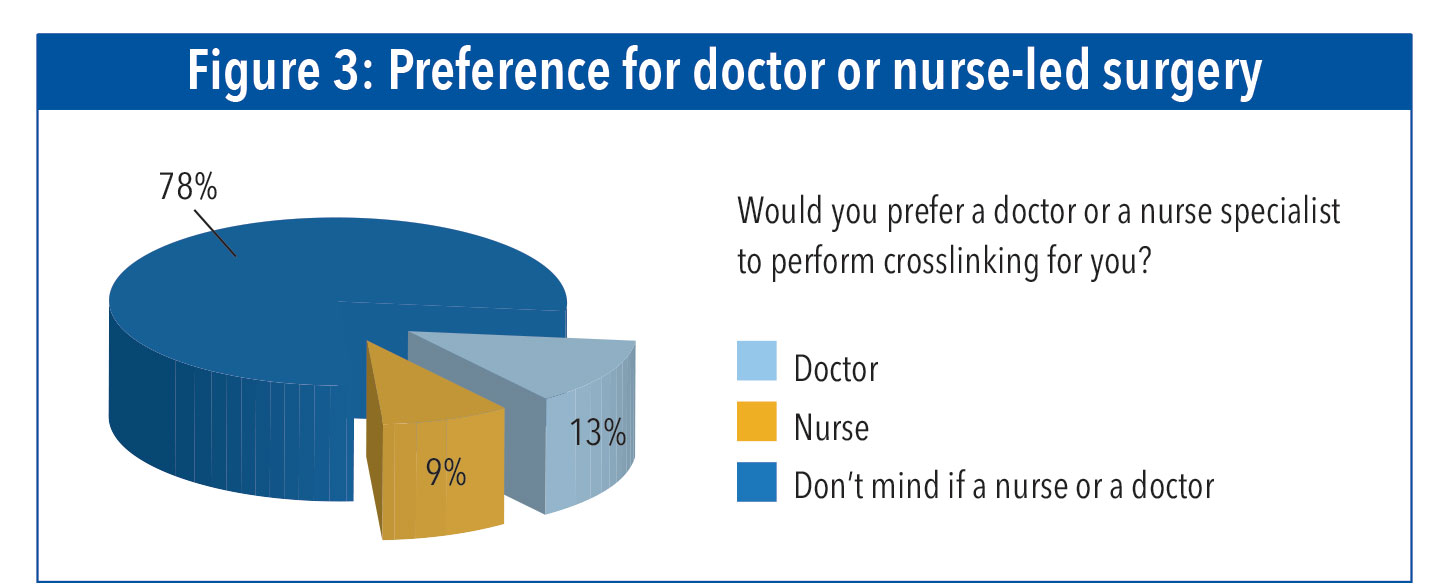
During the telephone survey, the patients were also asked if they prefer a nurse or a doctor to perform the surgical procedure for them, this is to determine patient preference in terms of practitioner. Most prefer a skilled practitioner, be it a nurse or a doctor. The result showed that 78% of patients did not mind if a nurse or a doctor did the procedure, while 9% preferred the nurse and 13% would have preferred if a doctor did the procedure. Overall, the nurse-led CXL service was well accepted by patients (see Figure 2).
(click to enlarge)
Quality assurance
Quality assurance mechanisms are essential to ensure safe practice and to detect any suboptimal management in nurse-led ophthalmic services.7 In this study, safety was monitored by recording the post-operative complications of nurse-delivered CXL over a 12-month period.
Some 144 eyes were treated in the nurse-led CXL service from January 2016 to December 2016. Twenty eyes were treated under the supervision of the consultant surgeon or corneal fellow/registrar and 124 eyes were treated by the corneal nurse specialist without direct observed supervision with no adverse events. Three (2.1%) eyes developed corneal infiltrates post operatively which responded well to treatment. Two eyes developed corneal haze which gradually improved after a month (see Figure 3).
(click to enlarge)
Results showed no patient had serious post-operative complications from the nurse-delivered CXL. Most patients had healed corneal epithelium one week post CXL treatment.
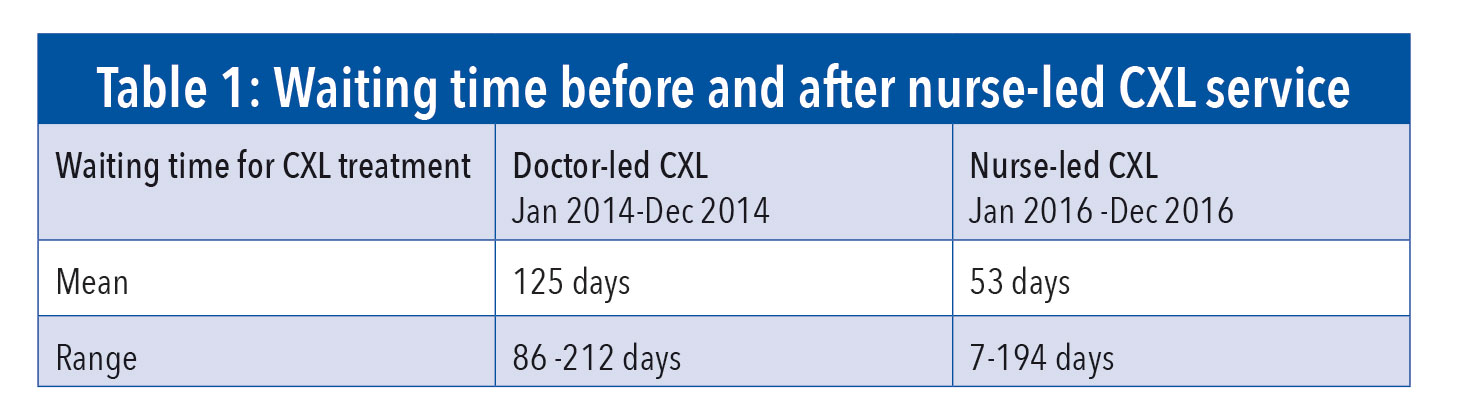
Patient waiting times
The goal of early treatment of keratoconus is to provide maximal vision function and to avoid the need for corneal transplantation.5 It is essential that patient should be treated with CXL as soon as they are diagnosed. The study showed that the introduction of nurse-led CXL service has reduced patient’s waiting time for CXL treatment (see Table 1).
(click to enlarge)
Pre-operation waiting time can for most patients become a very emotional time, the longer they wait the more anxious they become. A study by Bleustein et al8 confirms the strong relationship between waiting times and patient satisfaction.
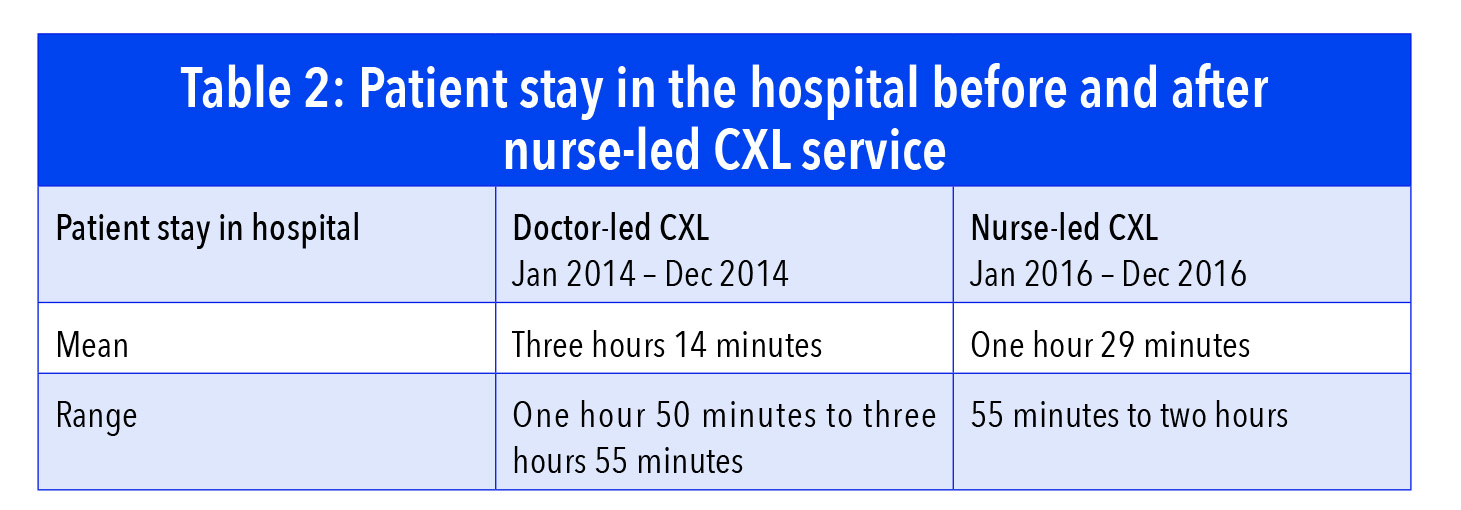
While it has always been the goal of healthcare systems to provide quality care as efficiently as possible their study further emphasised the need to minimise waiting time to improve patient satisfaction. Minimising waiting time in hospital promotes better patient experience thus improving patient satisfaction. This is one of the goals of the nurse-led CXL service, to minimise patient stay in hospital.
The study showed that patient stay in the hospital from admission to discharge was reduced with the introduction of the nurse-led CXL service. Patients used to wait more than three hours for a doctor to be available to perform CXL treatment. This is because junior doctors are busy admitting patients in the ward or doing surgical procedures in theatre. With the nurse-led CXL service the mean patient stay in the hospital fell to 1.29 hours (see Table 2).
(click to enlarge)
Cost-effectiveness
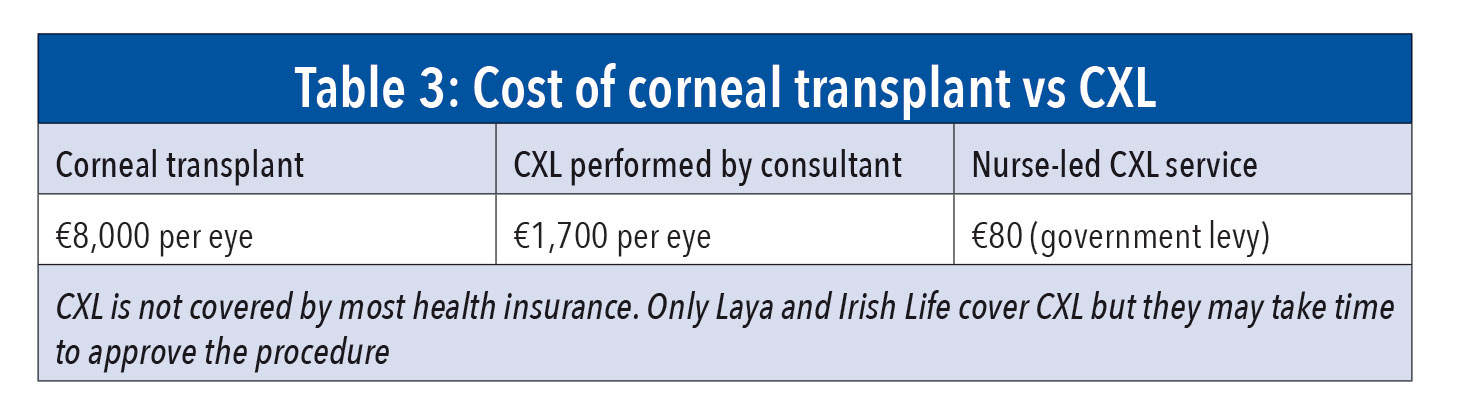
One of the main advantages of the nurse-led services is its cost-effectiveness compared to the medical-led services. The key determinant of cost-effectiveness is the practitioner’s salary,8 but cost of consumables also has an impact in the treatment of keratoconus patients. If keratoconus is not diagnosed and treated early, the condition continues to progress causing high corneal curvature, high astigmatism, low visual acuity, presence of corneal scarring and poor contact lens tolerance, in which case the patient will require cornaseal transplantation.9 Corneal transplantation is traditionally viewed as being successful in restoring vision. However it consumes considerable resources in terms of surgical cost, surgical time and follow-up, and requires constant access to donor tissue.10
In Ireland, corneal transplant costs €8,000 per eye, excluding the consultant fee and anaesthetist’s fee. There’s also the risk of graft failure, graft rejection and repeat of corneal transplant. CXL has less risk than corneal transplant and is cheaper – costing €1,700 per eye in private hospitals in Ireland. However for the nurse-delivered CXL, the patient will only pay a hospital levy of €80 per eye. This service is contributing more savings to the health service (see Table 3).
(click to enlarge)
Conclusion
To my knowledge, this study is the first report on the outcomes of nurse-led CXL service. The results showed that Ireland’s first nurse-led CXL service at RVEEH is as safe and effective as CXL performed by ophthalmologists. The service is acceptable to patients as reflected in the patient survey, which revealed overwhelming patient satisfaction levels. The study also showed that the nurse-led CXL service has reduced patient waiting time for treatment as well as patients’ stay in the hospital.
With early diagnosis of keratoconus and timely access to CXL treatment, the need for corneal transplantation can be eliminated resulting in significant cost savings to the health service and better quality of life to patients.
Diana Malata's work on setting up this service formed a research project that was the winner of the CJ Coleman 2018 INMO Research Award
Acknowledgements: Illustration by Ed Reynolds.
Photos by Stephen Comiskey and Hugh Nolan.
Patient survey by Othman Alrashidi
References
Cullen P and Duncan P. (2015) Inpatient, day case waiting list soar 11,710 percent, The Irish Times, October 9, 2015
Gordon D. (2017) Ophthalmology waiting lists ‘out of control’, Irishhealth.com, http://www.irishhealth.com/article.html?id=25730, March 14, 2017
Godefrooji DA, de Wit AG, Uiterwaal CS, Imhof SM, Wis RPL. (2016) Age-specific Incidence and Prevalence of Keratoconus: A Nationwide Registration Study, American Journal of Ophthalmology, Volume 175, 169-172
Trattker W. (2016) Corneal Cross-linking (CXL): For Keratoconus Treatment And LASIK-Related Corneal Ectasia. [Internet]: San Diego: allaboutvision.com; undated [ updated 2016 Nov, cited 2017 Feb 15]
Tullo W. (2013) When do you diagnose keratoconus? Optometry Times, May 22, 2013
Pearson AR, Soneji B, Sarvananthan N, Sandford-Smith JH, (2000) Does ethnic origin influence the incidence or severity of keratoconus?, Eye (London), Aug;14 ( Pt 4):625-8
Kirkwood JB, Pesuvidovs K, Latimer P and Coster D. (2006) The efficacy of a nurse-led preoperative cataract assessment and postoperative care clinic, Medical Journal of Australia, 184;6; 278-281
Bleustein C, Rothschild DB, Valen A, Valatis E, Schweitzer L, Jones R. (2014) Wait times, patient satisfaction scores, and the perception of care, American Journal of Managed Care, May;20(5):393-400
Kirkwood JB, Pesuedovs K, Loh R and Coster DJ. (2005) Implementation and evaluation of an ophthalmic nurse practitioner emergency eye clinic, Clinical and Experimental Ophthalmology, 33; 539-597
Sray WA, Cohen EJ, Rapuano CJ, Laibson PR. Factors associated with the need for penetrating keratoplasty in keratoconus, Cornea, 2002; 21(8):784-6
Salmon HA, Chalk D, Stein K, Frost NA. Cost effectiveness of collagen crosslinking for progressive keratoconus in the UK NHS. Eye (London). 2015;29:1504–1511
 (click to enlarge)
(click to enlarge)