Nutritional decline in cancer: Impact on quality of life, tolerance to treatment and survival, and an Irish context
Nutritional deterioration has unfortunately become an accepted part of the pathogenesis of cancer and its treatment
Dr Derek Power, Consultant in Medical Oncology, Cork University Hospital, Cork, Ms Samantha Cushen, Research Dietitian, Department of Food and Nutritional Sciences, University College Cork, Ms Aoife Ryan, Lecturer in Nutritional Sciences, University College Cork, Cork, Ms Erin Sullivan, Research Dietitian, University College Cork, Cork and Ms Louise Daly, Post Doctoral Scientist, University College Cork, Cork
It is well established that a decline in nutritional status is associated with poor quality of life and increased morbidity and mortality. Cancer cachexia (CC) is thought to affect 50-80% of patients with cancer. Its aetiology is multifactorial and complex, driven by pro-inflammatory cytokines and specific tumour-derived factors, which initiate an energy intensive acute phase protein response and drives the loss of skeletal muscle, even in the presence of adequate food intake. The most clinically relevant phenotypic feature of cachexia is muscle loss (sarcopenia) as this relates to asthenia, fatigue, impaired physical function, reduced tolerance to treatments, impaired quality of life and reduced survival. Sarcopenia is present in 11-90% of cancer patients depending on the tumour site and stage.2
Attention to secondary symptoms of the primary malignant disease, including weight loss (WL) and muscle wasting, is currently not a main priority in clinical care because management of the primary tumour is difficult on its own. Consequently, CC is rarely recognised, assessed or managed in a systematic manner, despite its significant clinical consequences.3 Furthermore, in the face of a global obesity epidemic, it is becoming increasingly difficult for oncologists and healthcare professionals to identify patients at risk of malnutrition as a high BMI does not preclude the presence of sarcopenia. Research into evidence-based interventions to prevent or reverse nutritional decline in cancer is under-funded. There is also a critical shortage of oncology dietitians in Ireland to refer patients to.
The clinical nutrition research group in University College Cork (UCC) is examining this often overlooked topic in order to identify the predictors of nutritional decline, understand the impact this decline has on tolerance to treatment, survival and QoL, and devise nutritional treatment pathways to attenuate or reverse the wasting associated with cancer. Ultimately, we need to move toward evidence-based detection and management of malnutrition early in the cancer journey in the hope of improving outcomes.
Aetiology of malnutrition in cancer
The aetiology of malnutrition in cancer is complex and multi-factorial. The pathophysiology includes derangement of metabolic and hormonal processes due to inflammatory mediators produced by the tumour microenvironment which can impair appetite and promote an inflammatory state associated with increased energy requirements and anabolic resistance.4 As well as abnormal metabolism of nutrients absorbed, there is also a reduction in oral intake and absorption due to nutrition impact symptoms such as anorexia, dysgeusia, nausea, constipation, diarrhoea, malabsorption and early satiety due to mechanical obstruction.5 These symptoms are caused by the mass effect of tumours as well as more complex, centrally mediated mechanisms such as attenuated orexigen production. Physical inactivity due to fatigue and pain are also important as reduced stimulus to muscles can lead to muscle atrophy.
Syndromes of abnormal body composition: Cachexia, sarcopenia and myosteatosis
Cachexia has been defined as ‘a multifactorial syndrome defined by ongoing loss of skeletal muscle mass (with or without loss of fat mass) that cannot be fully reversed by conventional nutrition support and leads to progressive functional impairment’.3 Its pathophysiology is characterised by a negative protein and energy balance driven by a variable combination of reduced food intake and abnormal metabolism. According to the 2011 consensus definition, CC can be diagnosed when any of the following three criteria are met3:
Weight loss > 5% of body weight in < six months, or
A BMI < 20kg/m2 and any degree of weight loss > 2%, or
Muscle depletion (sarcopenia).
Weight loss less than 5% in six months with corresponding loss of appetite or reduced dietary intake is termed pre-cachexia.3
The European Working Group on Sarcopenia in Older People defined sarcopenia as a syndrome of progressive and generalised loss of skeletal muscle mass and strength with a risk of adverse outcomes such as physical disability, poor QoL and death. While muscle loss is a normal part of ageing, this syndrome can also occur in association with disease, such as cancer. A generally accepted cut-point is skeletal muscle mass two standard deviations below that of a healthy, young population.6
Many studies globally have demonstrated high prevalence of sarcopenia (between 11-90%) in cancer patients across all primary sites and stages.1,2 Prevalence of sarcopenia is particularly high in patients with tumours of the gastrointestinal tract and lung,7 however diseases not commonly associated with nutrition intake are also affected by sarcopenia. In a recent large study of 3,241 women with stages II-III breast cancer, 34% presented with sarcopenia.8
Our group have examined the prevalence of sarcopenia, CC and reduced muscle radiodensity in a variety of Irish cancer cohorts using standardised diagnostic criteria.9,10,11,12,13 In a recent large study using computed tomography (CT) analysis of body composition in 725 patients on chemotherapy, our group reported that 42% had CC and 41% sarcopenia.13 This is the first time this data has been recorded for an Irish cancer population. While these results concur with those reported internationally, an important finding is that these conditions of abnormal body composition are prevalent across the spectrum of BMI classifications. In patients with a BMI < 18.5 kg/m2, 79% had CC, while 27% of those in the obese category had CC.13 Undernutrition is often overlooked in patients with normal or even high BMI who have lost significant amounts of weight. However, recent research reports that cancer patients with WL and muscle wasting have a poor prognosis regardless of overall body weight.14 Therefore, body composition is an important part of a complete nutritional assessment and simplistic screening tools, especially those based on BMI alone, are not suitable for use in oncology settings.13
Diagnosis: CT is readily available and is the gold standard
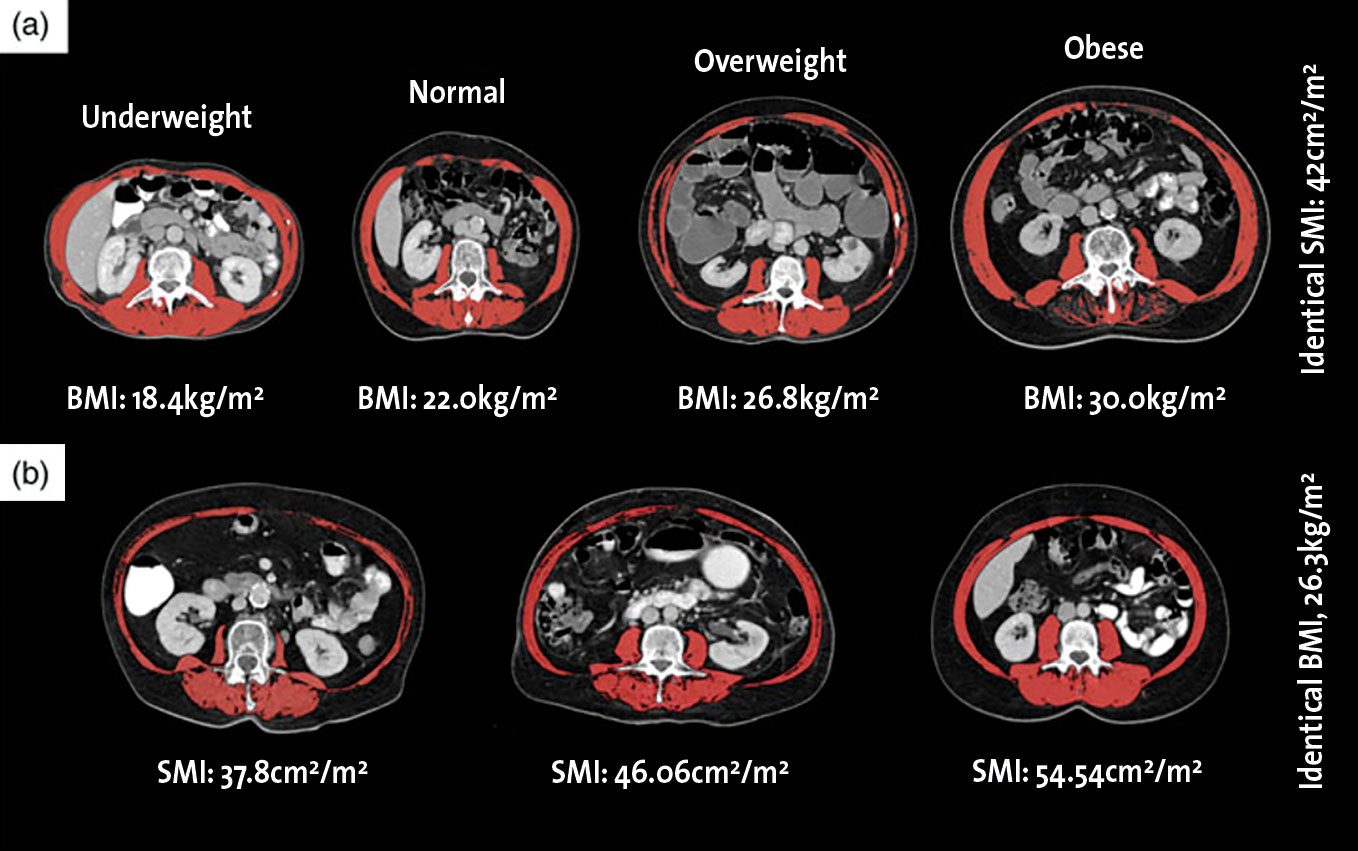
Malnutrition in cancer often presents with abnormal body composition that is not visually apparent and requires detailed assessment in order to be diagnosed. Recent studies have reported that despite having reported weight loss at the time of diagnosis, between 40-60% of cancer patients remain overweight or obese, even in the setting of metastatic disease.7,13,15,16 However, a high BMI does not preclude the presence of muscle wasting, and sarcopenia can be hidden by excess adipose tissue leading to a condition known as sarcopenic obesity. As a result, many patients with cancer-related malnutrition can often go undiagnosed until late in the course of their disease when wasting becomes visually apparent (see Figure 1).
Figure 1(a) shows four male sarcopenic patients with identical skeletal muscle index (SMI) ranging across different BMI categories. Figure 1(b) shows three female patients with identical BMI but varying SMI. Muscle depicted in red in all images.(click to enlarge)
Computed tomography (CT) imaging (a gold standard body composition tool) used daily in oncology practice to provide diagnostic information and monitor the progress of treatment, has uncovered significant findings about the body composition in cancer patients and reference values have been published for a variety of populations (for full review see Daly et al2). Axial CT images at the level of L3 are analysed to determine muscle mass, muscle radiodensity and adipose tissue mass (total, subcutaneous and visceral). Regression formulae are available to estimate whole body compartments using these data.17
The precision associated with CT analysis of body composition (1-1.5%) has allowed recent investigations to focus on the nature and magnitude of changes in body composition during the disease trajectory in patients with cancer. Studies have shown that cancer patients commonly lose muscle while undergoing active treatment and also this can be a consequence of some cancer directed therapies.18,19 In oesophagogastric cancer patients, neoadjuvant chemotherapy treatment, which is typically delivered over a 6-8-week period, can decrease skeletal muscle area by 9.59 cm2 (p < 0.0001), which is the equivalent to a loss of 2.9 kg of lean mass.20
We corroborated these findings in a study of 84 patients with metastatic melanoma treated with ipilimumab, whereby the prevalence of sarcopenia almost doubled (from 17% to 32%) during 12 weeks of treatment.12 In patients with cancer, muscle is lost at a very high rate of 3-5% per 100 days during systemic chemotherapy,12,21,22,23,24 and losses are exponentially increased with progressive disease and proximity to death.25,26 Noteworthy is that rate of muscle decline has been reported to be up to is 24-fold more rapid than that observed in healthy ageing adults who tend to lose muscle at a rate of 1-1.4% per year.27,28
Impact of nutritional deterioration
Tolerance to anti-cancer treatments
Chemotherapy can often be associated with severe toxicity that can result in dose delays, dose reductions and treatment termination, referred to as dose-limiting toxicities (DLT). Severe toxic events can result in hospitalisations and can even be life threatening. It has recently been acknowledged that variability in body composition (lean body mass, fat mass and total body water) of cancer patients may be a source of disparities in the metabolism of cytotoxic agents resulting in increased toxicity.29,30,31 To date, over thirty studies have examined the relationship between sarcopenia or low lean mass and the prevalence of severe or DLT in patients with cancer (for full review see Daly et al2).
Strong agreement has been reported among studies and they have concluded that sarcopenia is an independent predictor of DLTs. This relationship was true irrespective of the type of systemic chemotherapy (cytotoxic single agents, regiments, targeted agents and immunotherapies) and low muscularity has been associated with poorer tolerance to chemotherapy in patients with breast,32,33 renal,9,29,34 liver,35 lung,36 colorectal,37,38 thyroid39 and melanoma skin cancer.12,40
The oncology research group at UCC have contributed to this emerging body of literature and have published three studies looking at sarcopenia and its relationship with treatment tolerance.9,10,11 In a cohort of 84 patients with metastatic melanoma treated with ipilimumab, we reported that patients with sarcopenia were five times more likely to experience a severe treatment related adverse event (OR = 5.34, p = 0.033).12 Our group has also showed that sarcopenia was a significant predictor of DLT in 55 patients with metastatic renal cell carcinoma (p = 0.012)9 and in patients with metastatic prostate cancer treated with docetaxel (n = 63), a combination of both low muscle mass and low MA was associated with an increased risk of DLT (59 vs 29 %, p= 0·021).10
Collectively, these results highlight the emerging role of body composition assessment to improve the anticipation of chemotherapy-related toxicities. The ongoing collection of pharmacokinetic data in our institution could allow for further toxicity studies to help validate the possibility of individual drug dosing in specific chemotherapies.
Quality of Life
Cancer-associated malnutrition and CC have also been shown to have a profound effect on patient’s performance status, psychological wellbeing and overall quality of life (QoL).3,41 A recent systematic review reported a negative correlation between QoL and weight loss in 23 out of 27 studies of patients with CC.42
In Irish data (recently presented at ASCO 201843), studying 1,015 patients with solid tumours (27% colorectal, 24% foregut, 12% lung, 10% lymphoma and 10% breast cancer), percentage weight loss over the preceding six months was the greatest predictor of global QoL, and on random forest analysis was a more important determinant of global QoL than disease stage.43 The mode by which weight loss exerts its influence on QoL is not fully understood but may relate to muscle atrophy associated with cachexia, resulting in fatigue and reduced functional capacity which affect overall QoL.44
Survival
The adverse prognostic impact of weight loss and cachexia on overall survival in patients with cancer has long been recognised45,46,47,48 and in 2015, it was reported that even weight loss as little as 2.4% was predictive of survival independent of disease site, stage or performance status in a heterogenous group of cancer patients (n = 8,160).
The impact of body composition and sarcopenia on survival in oncology was first identified in a cohort of 250 obese lung and gastrointestinal cancer patients by Prado and colleagues in 2008.49 Within this study, sarcopenic obese patients had a lower median overall survival compared to their non-sarcopenic counterparts (11.3 vs 21.6 months, p < 0.001), and sarcopenic obesity independently predicted survival when adjusted for known prognostic covariates [HR: 4.2 (95% CI: 2.4-7.2), p < 0.0001)].49 Since then, sarcopenia has repeatedly been shown to be independently prognostic of reduced survival in a number of cancer sites and stages including pancreatic,50 kidney,51,52 liver,53,54,55 lung,56 oesophageal,57 colorectal,58,59,60 urothelial61,62 and lung and gastrointestinal cancers.7
More recently, the adverse prognostic role of muscle loss during treatment has been reported. Loss of muscle during systemic anti-cancer treatment is associated with increased mortality in patients with pancreatic,21,63 lung,64,65 colorectal,24,66 ovarian,23 melanoma,12 and foregut cancer.67 We have previously reported that in 89 patients with advanced cancers of the foregut, those with high rates of skeletal muscle loss (> 6%/100 days) were at more than double the risk of mortality [HR: 2.66 (95% CI: 1.42-4.97, p = 0.002)].67 In a further Irish study in metastatic melanoma, a loss of > 7.5% skeletal muscle mass per 100 days was also a significant predictor of survival (HR: 2.1, p = 0.046) when adjusted for age, gender and disease stage.12
In an Irish prospective cohort of 1,015 patients with cancer (preliminary findings recently presented at ASCO 201843), we reported that the most important predictors of overall survival were cancer site, and stage, followed by systemic inflammation, anorexia, weight loss and mean MA. This is important given that inflammation, loss of appetite, weight loss and deranged body composition are the hallmarks of cancer cachexia. Importantly, nutritional parameters were more reliable prognostic indicators than many clinical variables, including performance status.
The individual components of the cachexia syndrome are predictive of survival and therefore, the importance of cancer cachexia is highlighted. Importantly, survival was greatest in weight stable patients over those who either lost or gained weight during the preceding six months. Further work is ongoing in our group to examine the impact of changes in the specific compartments (subcutaneous or visceral) of adipose tissue on survival in colorectal and foregut cohorts in association with the already described changes in muscle.
Patient attitudes
A study currently underway on the Mercy University Hospital chemotherapy day ward is an extension of the previous study of 1,015, with a focus on patients attitudes toward nutrition in cancer, including dietitian referrals, use of nutritional supplements and knowledge of fad diets. Additionally, changes in taste and smell and specific food avoidances are being examined. Most notably, we are now collecting data on dietary intake which is not widely available at present. With these new data, we hope to identify predictors of malnutrition and abnormal body composition. Alongside this, a nationwide survey was rolled out in association with IrSPEN during Cancer Week (week of September 24, 2018), to nationally assess patient knowledge and attitudes regarding dietetic services, nutritional supplements, alternative diets and the importance of nutrition in cancer survivorship. To date, much of this information is anecdotal and the results of these surveys may help provide evidence of the need for increased services for cancer patients.
Management of cachexia
Unfortunately CC has perhaps suffered more from selective neglect and therapeutic nihilism than any other symptom requiring palliative care.68 There is currently no safe drug to reverse cachexia and no consensus on the optimal treatment, yet here is a urgency for improving management.1 Coupled with this is the severe shortage of dietitians working in oncology in Ireland, and recently the Irish Nutrition and Dietetic Institute workforce planning estimations submitted to the National Cancer Control Programme have highlighted that there are just six whole-time equivalent dietitians working in oncology outside the Dublin region and a further 65 WTE dietitians are required nationally to meet the needs to cancer patients.
Best practice, as stated by the American Society for Parenteral and Enteral Nutrition (ASPEN)69 and the National Institute for Health and Care Excellence (NICE)70 requires that all patients undergo nutritional screening and assessment, and the European School of Oncology recommends early recognition of cachexia.71 However, a UK survey reported that 80% of oncologists expressed uncertainty in identifying malnutrition in cancer patients and suggested that there needs to be improvements made in raising awareness of nutritional issues in oncology.72 Greater understanding of factors contributing to nutritional deterioration in cancer, as well as patients’ expectations and the personal impact of the disease, are required to devise meaningful nutritional therapy.
Several trials (including trials conducted in Ireland73) have examined single therapies for CC, including oral nutritional supplements, exercise, omega-3 fatty acids or anti-inflammatory drugs, however, results have been disappointing. Optimising oral intake is a key component to attenuating weight loss and nutritional interventions, (high-protein, high-calorie diets, enteral feeding and supplements) have been a mainstay of cachexia management to-date. Our group have produced three cookbooks to assist patients in meeting their nutritional requirements. These are available from Breakthrough Cancer Research (free of charge) and are aimed toward cancer patients in general, cancer patients with dysphagia and pancreatic cancer patients, respectively (https://www.breakthroughcancerresearch.ie/books-new/).
However, for those with established cachexia, nutritional interventions alone have failed to reverse the syndrome, there has been increased interest in pharmacological approaches, however, these have not shown great promise. Licenced appetite stimulants and anabolic steroids, have the potential for serious side effects and safer alternatives, such recently developed ghrelin mimetics (eg anamorelin), have yet to be licensed.74
The MENAC trial (a multimodal intervention of exercise, nutrition and anti-inflammatory medication plus standard care versus standard care alone) to prevent/attenuate cachexia will test the efficacy of a multi-dimensional approach during chemotherapy and is now under way at 12 international sites and will open in Cork in late 2018. Patients with advanced pancreatic and lung cancer will be studied to determine if the intervention achieves a difference in skeletal muscle index at six weeks.
The Pre-MENAC study showed that advanced cancer patients at risk of cachexia are capable of engaging in such a multimodal intervention which combines attenuation of inflammatory processes impairing normal metabolic processes using NSAID, providing anabolic stimulus in the form of mixed aerobic and resistance training as well as ensuring sufficient substrate by way of an EPA-enriched high protein, high calorie oral nutritional supplement.75 Identification of a successful cachexia treatment would mark significant progress in the field of oncology nutrition, and given the impact of nutrition on survival and tolerance to treatment, the oncology field as a whole.
Future priorities
Malnutrition and body composition changes in cancer are extremely common and are associated with poorer QoL as well as increased morbidity and mortality and are often considered an inevitable part of the cancer journey. However, since efficacy of unimodal therapies has been disappointing to date, it appears that the focus must be placed on multimodal approaches in order to tackle the multifactorial nature of cachexia pathophysiology. Further research into the pathogenesis, consequences and optimal management of cancer malnutrition, in particular refractory cachexia is of the utmost importance and stands to improve longevity and QoL for cancer survivors.
References
Ryan AM, Power DG, Daly L, et al. Cancer-associated malnutrition, cachexia and sarcopenia: the skeleton in the hospital closet 40 years later. Proc Nutr Soc 2016; 75(2): 199-2112
Daly LE, Prado CM, Ryan AM. A window beneath the skin: how computed tomography assessment of body composition can assist in the identification of hidden wasting conditions in oncology that profoundly impact outcomes. Proc Nutr Soc 2018; 77: 135-51
Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011; 12: 489-95
Argilés JM, Busquets S, Stemmler B, López-Soriano FJ. Cancer cachexia: understanding the molecular basis. Nat Rev Cancer 2014; 14: 754-62
Blum D, Omlin A, Baracos VE, et al, Collaborative EPCR. Cancer cachexia: a systematic literature review of items and domains associated with involuntary weight loss in cancer. Crit Rev Oncol Hematol 2011; 80: 114-44.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010; 39: 412-23
Martin L, Birdsell L, Macdonald N, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol 2013; 31: 1539-47
Caan BJ, Cespedes Feliciano EM, Prado CM, et al. Association of muscle and adiposity measured by computed tomography with survival in patients with nonmetastatic breast cancer. JAMA Oncol 2018; 4: 798-804
Cushen SJ, Power DG, Teo MY, et al. Body composition by computed tomography as a predictor of toxicity in patients with renal cell carcinoma treated with sunitinib. Am J Clin Oncol 2017; 40: 47-52
Cushen SJ, Power DG, Murphy KP, et al. Impact of body composition parameters on clinical outcomes in patients with metastatic castrate-resistant prostate cancer treated with docetaxel. Clinical Nutrition 2016; 13: e39-e45
Daly LE, Ní Bhuachalla É, Power DG, et al. Loss of skeletal muscle during systemic chemotherapy is prognostic of poor survival in patients with foregut cancer. J Cachexia Sarcopenia Muscle 2018; 9(2): 315-325
Daly LE, Power DG, O’Reilly Á, et al. The impact of body composition parameters on ipilimumab toxicity and survival in patients with metastatic melanoma. Br J Cancer 2017; 116: 310-7
Ní Bhuachalla É, Daly LE, Power DG, et al. Computed tomography diagnosed cachexia and sarcopenia in 725 oncology patients: is nutritional screening capturing hidden malnutrition? J Cachexia Sarcopenia Muscle 2017; 9(2): 295–305
Martin L, Birdsell L, Macdonald N, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. Journal of Clinical Oncology 2013; 31: 1539-47
Gioulbasanis I, Martin L, Baracos VE, et al. Nutritional assessment in overweight and obese patients with metastatic cancer: does it make sense? Ann Oncol 2015; 26: 217-21
Martin L, Senesse P, Gioulbasanis I, et al. Diagnostic criteria for the classification of cancer-associated weight loss. J Clin Oncol 2015; 33:90-9
Mourtzakis M, Prado CM, Lieffers JR, et al. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl Physiol Nutr Metab 2008; 33: 997-1006
Elliott JA, Doyle SL, Murphy CF, et al. Sarcopenia: Prevalence, and impact on operative and oncologic outcomes in the multimodal management of locally advanced esophageal cancer. Ann Sur 2017; 266: 822-30
Antoun S, Birdsell L, Sawyer MB, et al. Association of skeletal muscle wasting with treatment with sorafenib in patients with advanced renal cell carcinoma: results from a placebo-controlled study. J Clin Oncol 2010; 28: 1054-60
Awad S, Tan BH, Cui H, et al. Marked changes in body composition following neoadjuvant chemotherapy for oesophagogastric cancer. Clin Nutr 2012; 31: 74-7
Dalal S, Hui D, Bidaut L, et al. Relationships among body mass index, longitudinal body composition alterations, and survival in patients with locally advanced pancreatic cancer receiving chemoradiation: a pilot study. J Pain Symptom Manage 2012; 44: 181-91
Tan BH, Birdsell LA, Martin L, et al. Sarcopenia in an overweight or obese patient is an adverse prognostic factor in pancreatic cancer. Clin Cancer Res 2009;1 5: 6973-9
Rutten IJ, van Dijk DP, Kruitwagen RF, et al. Loss of skeletal muscle during neoadjuvant chemotherapy is related to decreased survival in ovarian cancer patients. J Cachexia Sarcopenia Muscle 2016; 7: 458-66
Blauwhoff-Buskermolen S, Versteeg KS, de van der Schueren MA, et al. Loss of muscle mass during chemotherapy is predictive for poor survival of patients with metastatic colorectal cancer. J Clin Oncol 2016; 34: 1339-44
Lieffers JR, Mourtzakis M, Hall KD, et al. A viscerally driven cachexia syndrome in patients with advanced colorectal cancer: contributions of organ and tumor mass to whole-body energy demands. Am J Clin Nutr 2009; 89: 1173-9
Prado CM, Sawyer MB, Ghosh S, et al. Central tenet of cancer cachexia therapy: do patients with advanced cancer have exploitable anabolic potential? Am J Clin Nutr 2013; 98: 1012-9
Frontera WR, Hughes VA, Fielding RA, et al. Aging of skeletal muscle: a 12-yr longitudinal study. J Appl Physiol (1985) 2000; 88: 1321-6
Goodpaster BH, Park SW, Harris TB, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci 2006; 61: 1059-64
Antoun S, Baracos VE, Birdsell L, et al. Low body mass index and sarcopenia associated with dose-limiting toxicity (DTL) of sorafenib in patients with renal cell carcinoma. Ann Oncol 2010; 21: 1594-8
Prado CM, Baracos VE, McCargar LJ, et al. Body composition as an independent determinant of 5-fluorouracil-based chemotherapy toxicity. Clin Cancer Res 2007; 13: 3264-8
Prado CM, Lima IS, Baracos VE, et al. An exploratory study of body composition as a determinant of epirubicin pharmacokinetics and toxicity. Cancer Chemother Pharmacol 2011; 67: 93-101
Prado CM, Baracos VE, McCargar LJ, et al. Sarcopenia as a determinant of chemotherapy toxicity and time to tumor progression in metastatic breast cancer patients receiving capecitabine treatment. Clin Cancer Res 2009; 15: 2920-6
Shachar SS, Deal AM, Weinberg M, et al. Skeletal muscle measures as predictors of toxicity, hospitalization, and survival in patients with metastatic breast cancer receiving taxane-based chemotherapy. Clin Cancer Res 2017; 23: 658-65
Huillard O, Mir O, Peyromaure M, et al. Sarcopenia and body mass index predict sunitinib-induced early dose-limiting toxicities in renal cancer patients. Br J Cancer 2013; 108: 1034-41
Mir O, Coriat R, Blanchet B, et al. Sarcopenia predicts early dose-limiting toxicities and pharmacokinetics of sorafenib in patients with hepatocellular carcinoma. PLoS One 2012; 7: e37563
Sjøblom B, Grønberg BH, Benth J, et al. Low muscle mass is associated with chemotherapy-induced haematological toxicity in advanced non-small cell lung cancer. Lung Cancer 2015; 90: 85-91
Chemama S, Bayar MA, Lanoy E, et al. Sarcopenia is associated with chemotherapy toxicity in patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy for peritoneal carcinomatosis from colorectal cancer. Ann Surg Oncol 2016; 23: 3891-8
Barret M, Antoun S, Dalban C, et al. Sarcopenia is linked to treatment toxicity in patients with metastatic colorectal cancer. Nutr Cancer 2014; 66: 583-9
Massicotte MH, Borget I, Broutin S, et al. Body composition variation and impact of low skeletal muscle mass in patients with advanced medullary thyroid carcinoma treated with vandetanib: results from a placebo-controlled study. J Clin Endocrinol Metab 2013; 98: 2401-8
Valentine H, François G, Nora K, et al. Sarcopenic overweight is associated with early acute limiting toxicity of anti-PD1 checkpoint inhibitors in melanoma patients. Invest New Drugs 2017; 35: 436-41
Ravasco P, Monteiro-Grillo I, Vidal PM, et al. Cancer: disease and nutrition are key determinants of patients’ quality of life. Support Care Cancer 2004; 12: 246-52
Wheelwright S, Darlington AS, Hopkinson JB, et al. A systematic review of health-related quality of life instruments in patients with cancer cachexia. Support Care Cancer 2013; 21: 2625-36
Power D, Daly L, Ni Bhuachalla E, et al. Determinants of quality of life and survival in ambulatory oncology patients receiving chemotherapy. Journal of Clinical Oncology 2018; 36(15 suppl): 10120
Fearon KC, Voss AC, Hustead DS, Group CCS. Definition of cancer cachexia: Effect of weight loss, reduced food intake, and systemic inflammation on functional status and prognosis. Am J Clin Nutr 2006; 83: 1345-50
Andreyev HJ, Norman AR, Oates J, et al. Why do patients with weight loss have a worse outcome when undergoing chemotherapy for gastrointestinal malignancies? Eur J Cancer 1998; 34: 503-9
Dewys WD, Begg C, Lavin PT, et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med 1980; 69: 491-7
Hess LM, Barakat R, Tian C, et al. Weight change during chemotherapy as a potential prognostic factor for stage III epithelial ovarian carcinoma: A Gynecologic Oncology Group study. Gynecol Oncol 2007; 107: 260-5
Langius JA, van Dijk AM, Doornaert P, et al. More than 10% weight loss in head and neck cancer patients during radiotherapy is independently associated with deterioration in quality of life. Nutr Cancer 2013; 65: 76-83
Prado CM, Lieffers JR, McCargar LJ, et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol 2008; 9: 629-35
Tan BH, Brammer K, Randhawa N, et al. Sarcopenia is associated with toxicity in patients undergoing neo-adjuvant chemotherapy for oesophago-gastric cancer. Eur J Surg Oncol 2015; 41: 333-8
Sharma P, Zargar-Shoshtari K, Caracciolo JT, et al. Sarcopenia as a predictor of overall survival after cytoreductive nephrectomy for metastatic renal cell carcinoma. Urol Oncol 2015; 33: 339.e17-23
Fukushima H, Nakanishi Y, Kataoka M, et al. Prognostic significance of sarcopenia in patients with metastatic renal cell carcinoma. J Urol 2016; 195: 26-32
Meza-Junco J, Montano-Loza AJ, Baracos VE, et al. Sarcopenia as a prognostic index of nutritional status in concurrent cirrhosis and hepatocellular carcinoma. J Clin Gastroenterol 2013; 47: 861-70
Voron T, Tselikas L, Pietrasz D, et al. Sarcopenia impacts on short- and long-term results of hepatectomy for hepatocellular carcinoma. Ann Surg 2015; 261: 1173-83
Levolger S, van Vledder MG, Muslem R, et al. Sarcopenia impairs survival in patients with potentially curable hepatocellular carcinoma. J Surg Oncol 2015; 112: 208-13
Kim EY, Kim YS, Park I, et al. Prognostic significance of CT-determined sarcopenia in patients with small-cell lung cancer. J Thorac Oncol 2015; 10: 1795-9
Tamandl D, Paireder M, Asari R, et al. Markers of sarcopenia quantified by computed tomography predict adverse long-term outcome in patients with resected oesophageal or gastro-oesophageal junction cancer. Eur Radiol 2016; 26: 1359-67
van Vledder MG, Levolger S, Ayez N, et al. Body composition and outcome in patients undergoing resection of colorectal liver metastases. Br J Surg 2012; 99: 550-7
Malietzis G, Currie AC, Athanasiou T, et al. Influence of body composition profile on outcomes following colorectal cancer surgery. Br J Surg 2016; 103: 572-80
Miyamoto Y, Baba Y, Sakamoto Y, et al. Sarcopenia is a negative prognostic factor after curative resection of colorectal cancer. Ann Surg Oncol 2015; 22: 2663-8
Psutka SP, Carrasco A, Schmit GD, et al. Sarcopenia in patients with bladder cancer undergoing radical cystectomy: impact on cancer-specific and all-cause mortality. Cancer 2014; 120: 2910-8
Fukushima H, Yokoyama M, Nakanishi Y, et al. Sarcopenia as a prognostic biomarker of advanced urothelial carcinoma. PLoS One 2015; 10: e0115895
Cooper AB, Slack R, Fogelman D, et al. Characterization of anthropometric changes that occur during neoadjuvant therapy for potentially resectable pancreatic cancer. Ann Surg Oncol 2015; 22: 2416-23
Stene GB, Helbostad JL, Amundsen T, Set al. Changes in skeletal muscle mass during palliative chemotherapy in patients with advanced lung cancer. Acta Oncol 2014; 54: 340-8
Nattenmüller J, Wochner R, Muley T, et al. Prognostic impact of CT-quantified muscle and fat distribution before and after first-line chemotherapy in lung cancer patients. PLoS One 2017; 12: e0169136
Miyamoto Y, Baba Y, Sakamoto Y, et al. Negative impact of skeletal muscle loss after systemic chemotherapy in patients with unresectable colorectal cancer. PLoS One 2015; 10: e0129742
Daly LE, Ní Bhuachalla É, Power DG, Cet al. Loss of skeletal muscle during systemic chemotherapy is prognostic of poor survival in patients with foregut cancer. Journal of Cachexia, Sarcopenia and Muscle 2017: In press
Del Fabbro E, Reddy SG, Walker P, et al. Palliative sedation: when the family and consulting service see no alternative. J Palliat Med 2007; 10: 488-92
Bauer J. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN J Parenter Enteral Nutr 2002; 26: 1-138
Excellence NIfHaC. Nutrition support for adults: oral nutrition support, enteral tube feeding and parenteral nutrition. 2006
Aapro M, Arends J, Bozzetti F, et al. Early recognition of malnutrition and cachexia in the cancer patient: a position paper of a European School of Oncology Task Force. Annals of Oncology 2014; 25: 1492-9
Spiro A, Baldwin C, Patterson A, det al. The views and practice of oncologists towards nutritional support in patients receiving chemotherapy. British journal of cancer 2006; 95: 431-4
Healy LA, Ryan A, Doyle SL, et al. Does prolonged enteral feeding with supplemental omega-3 fatty acids impact on recovery post-esophagectomy: Results of a randomized double-blind trial. Ann Surg 2017; 266: 720-8
Temel JS, Abernethy AP, Currow DC, et al. Anamorelin in patients with non-small-cell lung cancer and cachexia (ROMANA 1 and ROMANA 2): results from two randomised, double-blind, phase 3 trials. Lancet Oncol 2016; 17: 519-31
Solheim TS, Laird BJA, Balstad TR, et al. A randomized phase II feasibility trial of a multimodal intervention for the management of cachexia in lung and pancreatic cancer. J Cachexia Sarcopenia Muscle 2017; 8: 778-88
 Figure 1(a) shows four male sarcopenic patients with identical skeletal muscle index (SMI) ranging across different BMI categories. Figure 1(b) shows three female patients with identical BMI but varying SMI. Muscle depicted in red in all images.(click to enlarge)
Figure 1(a) shows four male sarcopenic patients with identical skeletal muscle index (SMI) ranging across different BMI categories. Figure 1(b) shows three female patients with identical BMI but varying SMI. Muscle depicted in red in all images.(click to enlarge)