Peer support programmes in breast cancer: is there a role for online and telephone support systems?
Pre- and post-evaluation of a face-to-face facilitated peer support programme highlighted some concerns that women with breast cancer have with online and telephone support
Ms Sinead Power, PhD Student, Catherine McCauley School of Nursing and Midwifery, University College Cork and Prof Josephine Hegarty, Associate Professor, Catherine McCauley School of Nursing and Midwifery, University College Cork
The purpose of this study is to provide an insight into the views of women with breast cancer on alternative forms of peer support, such as online or telephone programmes. These findings have emerged from a pre- and post-evaluation of a face-to-face facilitated peer support programme, which was conducted in January 2009. The study formed part of preliminary PhD fieldwork exploring the area of peer support in breast cancer.
Background
Breast cancer is the most common form of cancer in women, accounting for over a quarter (28%) of the total in the WHO European Region.1 The physical and psychological effects of breast cancer include nausea and vomiting, fatigue, altered body image, social isolation, depression and disruption to family relationships.2-4
Peer support programmes for women with breast cancer were first initiated in the 1950s with the development of the Reach to Recovery Programme, which focused on the provision of support by survivors of breast cancer to women who were newly diagnosed with breast cancer.5,6 Recent reviews of support programmes for patients with cancer illustrate the fact that support programmes may be delivered to patients in different formats. These programmes include online, telephone or face-to-face programmes.7-9 For some individuals, participating in face-to-face peer support programmes may not be an option due to geographical or medical barriers.10 There is evidence in the literature to suggest that alternative forms of support, such as online or telephone support programmes, may be equally as beneficial to women with breast cancer as face-to-face programmes.11-13
The area of online support is of particular interest due to the dramatic increase in computer ownership and access to the internet in recent years.14,15 Participants in previous studies on online and telephone support identified the lack of face-to-face contact and difficulties with technology when availing of alternative forms of support.16-18
The study
Permission to conduct the study was granted by the local ethics committee. The board of trustees of the cancer support house also gave their approval for the study. Women with primary breast cancer (n = 8), who had expressed an interest in participating in a seven-week, face-to-face peer support programme in a local cancer support house, were invited to participate in pre- and post-programme focus group interviews. Those who expressed an interest in participating were given an information leaflet detailing the nature and purpose of the study. All of the women approached took part in the interviews and signed a consent form to confirm their agreement to participate. Participants were assured of their anonymity and were also made aware of the fact that they could withdraw their participation at any time.
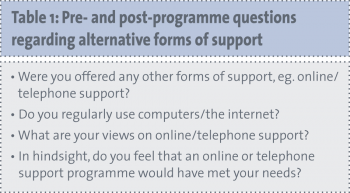
Both pre- and post-programme interviews were conducted in a quiet room in the researcher’s place of work. Both interviews were recorded and field notes were taken during the course of each interview. The data were transcribed verbatim by the researcher and were analysed through the use of thematic analysis. The questions asked in the pre- and post-programme interviews specific to alternative forms of peer support, such as telephone or online programmes, are detailed in Table 1.
(click to enlarge)
Key findings
Following analysis of the pre- and post-programme focus group questions, five key themes emerged regarding women’s receptiveness to alternative forms of peer support. These themes are detailed in Table 2. The five themes that emerged following analysis of the data will now be discussed and exemplars will be provided to illustrate the views of participants.
(click to enlarge)
Lack of face-to-face contact
The lack of face-to-face contact associated with telephone/online peer support programmes has already been identified within the literature.11,16,17 The findings of this study support that view. Participants were asked whether or not alternative forms of peer support would appeal to them. It is evident from the exemplars below that participants were not open to availing of telephone or online peer support programmes, even if they were made available to them. This was mainly due to the lack of face-to-face contact associated with such programmes. It is evident that this group of women considered the face-to-face component of peer support programmes to be of most importance to them.
“Something like online would be too impersonal for me, I much prefer face-to-face…there’s nothing like face-to-face…it’s the interaction between people…you don’t get that online…and especially with a small group of people.” (P.6)
“In a work situation, we had teleconferencing…I found that off-putting, not being able to see the person I was talking to…I found that quite hard… if it’s someone you know it’s fine…but with people you don’t know…it’s difficult…you can’t see their faces so you can’t see how they are reacting…as a result you don’t know how to pitch what you want to say…you don’t know…maybe they’re thinking ‘Oh what a load of rubbish!’.” (P.1)
Need to compartmentalise cancer
It is evident from the findings of this study that participants were determined to keep their cancer compartmentalised. This may have been a strategy they adopted to allow them to continue with their normal everyday lives. Some of the participants were fearful that by getting involved in an online or telephone support programme, they may not have been able to detach themselves from their cancer and that it would, in someway, take over their lives. This may be due to the asynchronous nature of the internet where one can log on at anytime of the day or night.
“I mean, we don’t want to be living, breathing cancer morning, noon and night...I feel that (refers to cancer support house) they would deal with that side of it for me…I’ll go up there if I want to go up there but I don’t want to be 24 hours thinking…cancer, cancer, cancer.” (P.7)
It is evident from the example above that this participant felt that attending the face-to-face programme in the cancer support house would allow her to somehow compartmentalise her cancer and enable her to carry on with her normal activities when not attending the cancer support house.
Fear of taking on the problems of others
Participants also voiced their concerns regarding getting involved in the problems of others while participating in online/telephone peer support programmes. These concerns may have emerged from the notion that the Internet is asynchronous and available to individuals at any time of the day or night. It is clear from the examples below that participants were more open to the structured support programme available in the cancer support house. There was a perception that the face-to-face programme would somehow protect them from getting involved in the problems and emotions of other group members.
“I think you have to keep it behind you to a degree. I’ll go when I want to…logging on, you know...listening to other people’s experiences...you can only take on your own experiences. You just have to turn a blind eye and say ‘right it’s a very sad story. I’m very sorry, but I have enough of my own problems to deal with at the moment’.” (P.1)
“There are counsellors there, you know (referring to cancer support house), they are trained to deal with the emotions of others…if someone got upset online…I wouldn’t know what to do.” (P.3)
Appeal of alternative forms of peer support
All of the participants in this study were of the view that alternative forms of support, such as online or telephone programmes, would be more acceptable to younger individuals with cancer. Participants expressed their caution regarding communicating online, for example, but acknowledged the fact that younger individuals may be more accustomed to and therefore more comfortable with communicating online.
“I think the next generation of cancer sufferers would be more into it. I probably would be a bit cautious about what I would say online…what I’d write online, blogs or whatever…I think the next generation would definitely be into it. Maybe we’re a bit…I mean, we didn’t grow up with it…I use it a good bit for work, pleasure, etc. but I think the next generation would use it more.” (P.3)
Alternative forms of support as a follow-on to face-to-face support
In the post-programme focus group interview, participants were asked about their views on alternative forms of support having completed the seven-week facilitated peer support programme. It is worthy of note that two participants expressed the view that telephone/internet support may be of use as a follow-up to traditional face-to-face programmes when relationships have been established.
“Maybe these types of supports would work for us now that we know each other…but certainly not at the beginning, when none of us knew each other.” (P.7)
“If I was in a situation where I needed support in the morning…I would most likely talk to one of these ladies rather than phone (Cancer Support House). I’d be more inclined to phone one of these women…because they know what it’s like…they’ve been through it…they understand.” (P.8)
The participants in this study were open to using alternative forms of support having established trusting relationships with other members of the group. These exemplars also demonstrate that participants would not be comfortable communicating with other individuals regarding their breast cancer without having first become acquainted with them face-to-face.
This suggests that a combination of face-to-face and alternative peer support programmes may be useful in supporting patients with breast cancer at different stages of their cancer journey.
Discussion
Following analysis of the pre- and post-programme interviews, it emerged that the participants in this study had reservations about availing of alternative forms of peer support via the telephone or the internet. These reservations emerged from concerns relating to the lack of face-to-face contact associated with online and telephone peer support programmes.
This finding concurs with the available literature where the lack of face-to-face contact was considered to be a drawback of telephone and online peer support programmes.16-18
Some of the participants in this study also identified the need to compartmentalise their cancer. There is evidence within the literature that individuals with a diagnosis of cancer are concerned with maintaining normality in their everyday lives.3,19,20 The participants in this study voiced the need to keep their cancer separate from their day-to-day lives.
Some of the participants felt that the asynchronous nature of the internet would mean that they would have difficulty ‘switching off’ from their cancer. Consequently, participants felt that taking part in the facilitated face-to-face peer support programme would enable them to separate their cancer from their everyday lives.
Within the findings of this study, the fear of taking on the problems of others emerged as a significant theme. Participants were concerned about protecting themselves from the problems of others. There was a perception that the emotional impact of cancer would be dealt with better in the face-to-face programme facilitated by trained professionals than online. This perception may stem from participants’ lack of understanding that many online programmes are facilitated by trained professionals.11,12
It is clear from the findings of this study that, initially, participants were not receptive to taking part in online or telephone peer support programmes, however, findings from the post-programme focus group interview indicate that the women were open to communicating online or via the telephone with fellow participants, now that relationships and bonds had developed between individuals.
This suggests that online or telephone support programmes may be of use to women who have taken part in face-to-face facilitated peer support programmes. Such programmes may be effective in enabling cancer survivors to avail of support from fellow survivors. This is an important finding in light of the increase in cancer survivorship in recent years.20,21
Within the post-programme focus group interview, it was suggested that online or telephone peer support may be more acceptable to younger individuals with cancer due to their reliance on computers and mobile phones for everyday communication. This is also a significant point due to the increase in cancer survivorship among young people in the 15-29-year age group within the past decade.18,21
Implications for practice
The findings of this study have important implications for those involved in the planning and implementation of peer support programmes in cancer.
In recent years, individuals have become more reliant on technology as a means of communication, thereby warranting further exploration of the potential advantages in developing online/telephone support programmes.
It is evident that individuals with cancer need to be provided with more information on how online and telephone peer support programmes operate, which may help to dispel any misconceptions and fears that could prove impediments to taking part in such programmes.
Online- and telephone-based peer support programmes may be of benefit if implemented as a follow-up to facilitated face-to-face programmes. These programmes may have an important role in enabling the increasing number of individuals surviving a diagnosis of cancer to avail of support from peers who have been exposed to a similar experience.
The participants in this study identified the fact that online or telephone peer support programmes may be more acceptable to younger individuals with cancer. This is an area that requires further exploration.
Limitations
The findings of this study provide valuable recommendations for the future development of peer support programmes in the area of breast cancer.
However, the study is not without its limitations. The relatively small sample size (n = 8) and the fact that the study was confined to women with breast cancer greater than 30 years old means that the findings may not be transferable to individuals less than 30 years old with a diagnosis other than breast cancer.
Acknowledgements
We wish to acknowledge the following people without whom this study would not have been possible: The eight women who gave freely of their time to take part in the pre- and post-focus group interviews; staff and volunteers at ARC House Cork, particularly Ellen, Fiona, Marie and Ann; Professor Joyce Fitzpatrick (Fulbright Professor) at the Catherine McCauley School of Nursing and Midwifery, Brookfield Health Sciences Complex, College Road, Cork, for her expert advice; and my fellow colleagues and members of the Irish Cancer Society (Steering Group Committee on building effective cancer support groups for Ireland) for their encouragement to date.
References
World Health Organisation, Regional Office for Europe. www.euro.who.int/en/what-we-do/health-topics/noncommunicable-diseases/cancer/news/news/2012/2/early-detection-of-common-cancers/breast-cancer
Boehmke MM, Dickerson SS. Symptoms, symptom experiences, and symptom distress encountered by women with breast cancer undergoing current treatment modalities. Cancer Nursing 2005; 28(5): 382-389
Power S, Condon C. Chemotherapy-induced alopecia: A phenomenological study. Cancer Nurs Pract 2008; 7(7): 44-47
Von A, Kang D. Correlates of mood disturbance in women with breast cancer: Patterns over time. J Adv Nursing 2008; 61(6): 676-689
Holland JC, Rowland JH. Handbook of psycho-oncology: Psychological care of the patient with cancer. Oxford University Press: New York, 1990
American Cancer Society. Reach to Recovery 2010 www.cancer.org/treatment/supportprogramsservices/reach-to-recovery
Hoey L, Ieropoli S, White V, et al. Systematic review of peer support programs for people with cancer. Patient Ed Counselling 2008; 70(3): 315-337
Gottileb BH, Wachala ED. Cancer Support Groups: A critical review of empirical studies. Psycho-Oncol 2007; 16(5): 379-400
Uden-Kraan C, Drossaert C, Taal E, et al. Coping with somatic illnesses in online support groups. Do the feared disadvantages really occur? Computers in Human Behaviour 2008; 24(2): 309-324
Reed L. Online support: A lifeline for women with breast cancer? Eur J Pall Care 2004; 11(6): 246-247
Hoybye MT, Johansen C, Tjornhoj-Thomsen T. Online interaction: Effects of storytelling in an internet breast cancer support group. Psycho-Oncol 2005; 14(3): 211-220
Giese-Davis J, Bliss-issberg G, Carson K, et al. The effect of peer counselling on quality of life following diagnosis of breast cancer: An observational study. Psycho-Oncol 2006; 15(11): 1014-1022
US Census Bureau. Computer and Internet use in the United States: 2003. Available online www.census.gov/
CSO. Census of Ireland 2011. Profile 4: The roof over our heads – Housing in Ireland. CSO 2012. Available online www.cso.ie/en/census/census2011reports/census2011profile4theroofoverourheads-housinginireland/
Sharf B. Communicating Breast cancer: Online support and empowerment on the Internet. Women and Health 1997; 26(1): 65-84
Curran VR, Church JG. Not alone: Peer support through audio teleconferencing for rural women with breast cancer. CMAJ 1998; 159(4): 379-381
Ekman I, Bergbom I, Ekman T, et al Maintaining normality and support are central issues when receiving chemotherapy for ovarian cancer. Cancer Nursing 2004; 27(3): 177-182
Grinyer A. Young people living with cancer: Implications for policy and practice. Open University Press: UK, 2007
Lieberman MA, Golant M, Giese-Davis J, et al. Electronic support groups for breast carcinoma: A clinical trial of effectiveness. Cancer 2003; 97(4): 920-925
Hewitt M, Greenfield S, Stovall E. From cancer patient to cancer survivor: Lost in transition. National Cancer Policy Board. National Academic Press: Washington, 2005
De P, Ellison LF, Barr RD, et al. Canadian adolescents and young adults with cancer: opportunity to improve coordination and level of care. CMAJ 2011; 183(3): E187-194
 (click to enlarge)
(click to enlarge)
