Recent advancements in HER2-positive breast cancer
The history of HER2-positive breast cancer has been revolutionised following the introduction of anti-HER2 therapies
Dr Giuseppe Gullo, Consultant Medical Oncologist, St Vincents University Hospital, Dublin and Prof John Crown, Consultant Medical Oncologist, St Vincents University Hospital, Dublin
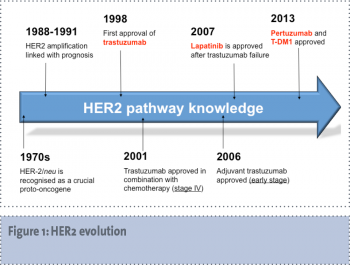
There is no doubt that few areas in medicine over the past decade have seen such meaningful progress, in both the degree of molecular knowledge and improvement of patients’ care, as the human epidermal growth factor receptor 2 (HER2) -positive breast cancer. In fact, despite the HER2/neu gene amplification or overexpression of the HER2 protein leading to a more aggressive phenotype and a poorer prognosis,1 the natural history of HER2-positive breast cancer has been revolutionised following the introduction of anti-HER2 therapies, the first of which was trastuzumab. It is increasingly evident that HER2-positive breast cancer patients treated with a systemic therapy incorporating anti-HER2 agents have an even better prognosis than the HER2-negative subgroup.
(click to enlarge)
HER2 as a therapeutic target
When trastuzumab was licensed in 1998 for use in pre-treated HER2-positive metastatic breast cancer patients, it was the first novel biological anticancer agent to be available for clinical use in a solid malignancy. Interestingly, initial clinical data did not appear as promising as it would prove to be at a later date for trastuzumab as a single agent; it produced an overall response rate of only 11%, approximately, in heavily pre-treated HER2-positive metastatic breast cancer patients.2 Moreover, very little was known at the time about the biological role and clinical relevance of HER2 as a crucial therapeutic target in breast cancer, and there was no other experience whatsoever with monoclonal antibodies in human malignancies, with the exception of rituximab for non-Hodgkin’s lymphomas.
Since then, HER2-positive breast cancer has become the most attractive and rewarding model for the development of targeted therapies and, even more importantly, a paradigm for the whole concept of the ‘translational’ bench-to-bedside continuum that is the fundament of modern translational oncology.
In 2006, HER2-positive breast cancer became the first human malignancy for which a monoclonal antibody was introduced as an essential part of the adjuvant treatment programme, on the base of an undisputable survival benefit. This miliary stone was set only eight years since the first approval of trastuzumab in the metastatic setting, a surprisingly short time for an agent with such an innovative mechanism of action.
Over the subsequent years, there has been an impressive acceleration in the degree of insight into the molecular aspects of HER2-positive breast cancer as well as a consolidation of the role of anti-HER2 agents across all the stages of the disease, from the neo-adjuvant setting to the multiple lines of therapy for advanced disease. This has led to the introduction of other HER2-targeting agents, such as the multi-tyrosine kinase inhibitor lapatinib, the chemo-immuno conjugate T-DM1 (trastuzumab emtansine) and, most recently, the monoclonal antibody pertuzumab. These agents have produced further incremental improvements in the outcome of HER2-positive breast cancer.
Over the past 12 months the results of important clinical trials on HER2-positive breast cancer have been presented, thus bringing the standard of care to an even greater level of advancement. Here we will discuss in detail the impact on clinical practice of two large randomised clinical trials: the BETH and the CLEOPATRA study, presented at the 2013 San Antonio Breast Cancer Symposium and at the 2014 ESMO Conference, respectively.
Therapy advances in early-stage HER2-positive breast cancer
The results of the phase III international BETH (bevacizumab with trastuzumab adjuvant therapy in HER2-positive breast cancer) study at a median follow-up of 38 months were presented at the 36th annual San Antonio Breast Cancer Symposium (SABCS) in December 2013.3 The BETH study was designed and conducted to investigate whether the addition of bevacizumab to two separate adjuvant chemotherapy-trastuzumab combination regimens would improve invasive disease-free survival (DFS) in patients with early-stage HER2-positive breast cancer.
The study had its rationale in the correlation between high levels of HER2 and high levels of VEGF within the tumour and poor prognosis. In fact, both have been identified as independent prognostic factors and together predict an even worse outcome.
In the BETH trial, a total of 3,509 women with HER2-positive breast cancer who had node-positive disease or high-risk, node-negative disease were enrolled to one of two cohorts: 3,231 were enrolled in cohort 1 (TCH: docetaxel/carboplatin/trastuzumab) and 278 patients were enrolled in cohort 2 (anthracycline/trastuzumab). Patients in cohort 1 received six cycles of TCH with or without bevacizumab followed by trastuzumab with or without bevacizumab for the rest of the 12-month treatment. Patients in cohort 2 received three cycles of trastuzumab plus docetaxel, followed by three cycles of 5-fluorouracil, epirubicin, cyclophosphamide, and finally trastuzumab with or without bevacizumab for up to 12 months.
The results of the study, presented by Dr Dennis Slamon of the UCLA Jonsson Comprehensive Cancer Center, showed that invasive DFS rates for HER2-positive breast cancer patients treated with TCH were 92% – both with and without bevacizumab. Therefore, regarding HER2, the BETH study has definitively answered that bevacizumab does not provide an additional benefit to the current treatment strategies for HER2-positive breast cancer (see Figure 2).
(click to enlarge)
Although this is an undoubtedly negative study for bevacizumab in HER2-positive breast cancer, the chemotherapy/trastuzumab control arm of the BETH study yielded a very high DFS rate, thus setting the bar very high for future studies and representing a hard mark to beat. In fact, this trial showed a significant improvement in invasive DFS at three years compared with the Breast Cancer International Research Group (BCIRG) 006 trial published in the New England Journal of Medicine in 2011,4 which showed an 86% invasive DFS rate for a similar patient group.
The BETH study found that invasive DFS was slightly higher among patients with node-negative disease (96%) compared with node-positive patients (88%), but bevacizumab did not improve outcomes for any subgroup. Of note, in the BCIRG 006 trial, the three-year invasive DFS rate was 85% for node-positive patients and 96% for node-negative patients.
The addition of bevacizumab in the BETH study resulted in higher rates of grade 3/4 adverse events. In the chemotherapy/trastuzumab treatment arms, only 8% of patients had a grade 3/4 adverse event compared with 27% of patients in the bevacizumab experimental arms (p < 0.0001). Hypertension was higher among bevacizumab-treated patients, with 19% of these patients experiencing a grade 3/4 hypertension event compared with 4% of patients in the chemotherapy/trastuzumab group (p < 0.0001). Bleeding, although rare, was higher among patients treated with bevacizumab (2% compared with < 1% for patients in the non-bevacizumab arm; p < 0.0001). Congestive heart failure was higher in the bevacizumab treatment arm (2.1% versus < 1%; P = 0.0621), as was proteinuria (1% versus < 1%; p < 0.0001) and gastrointestinal perforations (11 cases versus 1 case; P < 0.0001).
Implications for clinical practice
Following the presentation of the results of the BETH study, the debate remains open whether, on the basis of the striking results of the trial’s non-anthracycline-containing arm, TCH should be regarded as the combination of choice for treating women with HER2-positive breast cancer after surgery, regardless of tumour size or lymph node status. It has to be noted that although the BETH trial showed TCH results in similar efficacy and lower toxicity compared with anthracyclines, the trial was not specifically designed to compare the difference in outcomes of these two chemotherapy regimens when combined with trastuzumab.
It is well known that a small but defined number of patients who receive trastuzumab in combination with anthracycline can suffer cardiac dysfunction, including congestive heart failure. Substituting anthracyclines with docetaxel plus carboplatin results in similar efficacy without the toxicity, hence the clinical rationale for adopting the non-anthracycline containing regimen as a standard therapy. The results of both the BETH and BCIRG 006 trial results could indicate a potentially limited role for anthracyclines in adjuvant therapy for HER2-positive breast cancer patients. In fact, no single trial has clearly shown an incremental benefit with anthracyclines, as had been previously demonstrated in a pooled meta-analysis only.5 It would be incorrect to conclude that anthracyclines are not effective in HER2-positive breast cancer, however, they do not appear to add a clear incremental benefit.
Therapy advances in metastatic HER2-positive breast cancer
Trastuzumab was initially investigated in heavily pre-treated HER2-positive metastatic breast cancer as a single agent,2,6 and subsequently in combination with chemotherapy.7 These promising preliminary results led to the pivotal phase III study by Slamon et al, which demonstrated significant improvements in overall response as well as progression-free and overall survival in patients with HER2-positive metastatic breast cancer treated with chemotherapy and trastuzumab in the first-line setting.8
To date, the combination of trastuzumab and chemotherapy as first-line treatment of HER2-positive metastatic breast cancer has been investigated in other phase III clinical trials, all published between 2006 and 2013.9,10,11,12,13,14,15 The results from these trials have demonstrated an overall response rate ranging from 36-80%, with a time to progression between six and 15 months.
Of all the chemotherapeutic agents combined with trastuzumab in these trials, the most active were the taxanes and platinum compounds, with significant and exciting advances made in recent times with the introduction of pertuzumab.
Pertuzumab is a monoclonal antibody that binds to the HER2 extra-cellular domain at a different epitope to that of trastuzumab, such that both agents can be used in conjunction to achieve comprehensive blockade of HER2 signalling.16 This strategy has been the primary investigational focus of the phase III CLEOPATRA study,14,15 of which the updated overall survival data was presented at the ESMO 2014 Congress in Madrid in September.
In the CLEOPATRA study, 808 patients from 25 countries with HER2-positive metastatic, locally recurrent, or unresectable breast cancer with measurable or non-measurable disease were randomised to receive first-line docetaxel/trastuzumab/placebo or docetaxel/trastuzumab/pertuzumab. The addition of pertuzumab significantly improved overall survival (OS) for patients with HER2-positive metastatic breast cancer, providing a median 15.7-month increase.
The median OS of 56.5 months seen in the docetaxel/trastuzumab/pertuzumab arm has been defined as ‘unprecedented’ in first-line therapy for HER2-positive advanced breast cancer. The PFS in the pertuzumab arm was 18.7 versus 12.4 months in placebo arm (HR = 0.68; p < 0.0001). It is interesting to observe that the control arm of the CLEOPATRA study is essentially superimposable onto the docetaxel (100mg/m2)/trastuzumab arm of the M77001 study, published by Marty et al in 2005,17 which had shown a time to disease progression of 11.7 months. It is important to note that in July 2012, following a statistically significant improvement in OS on the second interim analysis (May 2012), the patients still on trastuzumab/placebo were offered crossover to pertuzumab.
Implications for clinical practice
Some clinically important points have to be highlighted and discussed regarding the CLEOPATRA study population. Firstly, adjuvant trastuzumab was administered to only 10% of the study population and this does not reflect the current clinical scenario where the vast majority of patients with early stage HER2-positive breast cancer receive trastuzumab for one year in the early setting. Secondly, it appears that a meaningful proportion of patients – nearly 30% – did not receive a further anti-HER2 agent with their subsequent lines of treatment at first disease progression and this is also not in keeping with the common practice in most countries. Thirdly, the CLEOPATRA study did not allow patients with ER-positive tumours to have endocrine therapy with the anti-HER2 therapy following the completion of docetaxel. Concomitant administration of pertuzumab/trastuzumab and endocrine therapy is feasible, as demonstrated in the APHINITY study in the adjuvant setting, so it is legitimate to wonder if the addition of endocrine therapy after chemotherapy ends can increase the benefit seen in women with HER2-positive/ER-positive disease.
The addition of pertuzumab to docetaxel/trastuzumab was not without additional toxicity. In fact, the safety data of the CLEOPATRA study showed more pronounced diarrhoea, rash, mucosal inflammation, pruritus, dry skin, and muscle spasm. No new safety concerns were seen with longer follow-up and there was no evidence of cumulative or late toxicity, including cardiac safety profile.
Trastuzumab emtansine (T-DM1)
In the second-line setting, the role of T-DM1 is now fully established following the presentation of the results of the EMILIA trial that showed a superiority of the chemo-immuno conjugate over the standard of care with capecitabine and lapatinib.18 The importance of the EMILIA trial is not limited to the improvements seen in its clinical endpoints but also the proof of concept that chemo-immuno conjugates can play a meaningful role in the treatment of breast cancer and possibly of other malignancies. Consequently, results are eagerly awaited from the phase III trial, MARIANNE, a randomised study of T-DM1 with or without pertuzumab compared with trastuzumab plus a taxane (docetaxel or paclitaxel) for first-line treatment of HER2-positive, progressive, or recurrent locally advanced or metastatic breast cancer.
Conclusions
Many impressive advancements have been made in the treatment of HER2-positive breast cancer over the last decade, marking this as a very exciting time for those involved in both basic and clinical research into this breast cancer subtype.
Examining the remarkable results of the control arm of the BETH trial, one must ask if it is realistic to imagine further improvements, especially for patients with node-negative disease? This is certainly a major challenge for the future of clinical research in HER2-positive breast cancer.
The scenario is remarkably different in the setting of advanced disease where, despite the improvements achieved with the CLEOPATRA and the EMILIA studies, the vast majority of patients still have incurable cancer and will eventually die from their disease.
Recently, durable complete remissions of HER2-positive overtly metastatic breast cancer following chemotherapy and anti-HER2 therapy have been systematically described.19 Regarding a meaningful minority of patients (approximately 9-10%), this subset of extremely trastuzumab-sensitive HER2-positive neoplasms could represent the ideal benchmark for the investigation of mechanisms of sensitivity/resistance to trastuzumab and the other anti-HER2 therapies. Further improvements in this setting can be expected by addressing key features of HER2-positive breast cancer linked to different sensitivity in term of hormone receptor status (positive versus negative), PIK3CA status (wild type versus mutant), and immune environment.
References
Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987; 235(4785): 177-182.
Baselga J, Tripathy D, Mendelsohn J, et al. Phase II study of weekly intravenous recombinant humanized anti-p185HER2 monoclonal antibody in patients with HER2/neu-overexpressing metastatic breast cancer. J Clin Oncol 1996; 14: 737-744.
Slamon DJ, Swain SM, Buyse M, et al. Primary results from BETH, a phase 3 controlled study of adjuvant chemotherapy and trastuzumab ± bevacizumab in patients with HER2-positive, node-positive or high risk node-negative breast cancer. Presented at: 2013 San Antonio Breast Cancer Symposium; December 10-14, 2013; San Antonio, TX. Abstract S1-03.
Slamon D, Eiermann W, Robert N, et al. Adjuvant trastuzumab in HER2-positive breast cancer. NEJM 2011; 365(14): 1273-1283.
Gennari A, Sormani MP, Pronzato P, et al. HER2 status and efficacy of adjuvant anthracyclines in early breast cancer: a pooled analysis of randomized trials. J Natl Cancer Inst 2008; 100(1): 14-20.
Cobleigh MA, Vogel CL, Tripathy D, et al. Multinational study of the efficacy and safety of humanized anti-HER2 monoclonal antibody in women who have HER2-overexpressing metastatic breast cancer that has progressed after chemotherapy for metastatic disease. J Clin Oncol 1999; 17(9): 2639-2648.
Pegram MD, Lipton A, Hayes DF, et al. Phase II study of receptor-enhanced chemosensitivity using recombinant humanized anti-p185HER2/neu monoclonal antibody plus cisplatin in patients with HER2/neu-overexpressing metastatic breast cancer refractory to chemotherapy treatment. J Clin Oncol 1998; 16(8): 2659-2671.
Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. NEJM 2001; 344(11): 783-792.
Robert N, Leyland-Jones B, Asmar L, et al. Randomized phase III study of trastuzumab, paclitaxel, and carboplatin compared with trastuzumab and paclitaxel in women with HER-2-overexpressing metastatic breast cancer. J Clin Oncol 2006; 24(18): 2786-2792.
Burstein HJ, Keshaviah A, Baron AD, et al. Trastuzumab plus vinorelbine or taxane chemotherapy for HER2-overexpressing metastatic breast cancer: the trastuzumab and vinorelbine or taxane study. Cancer 2007; 110(5): 965-972.
Inoue K, Nakagami K, Mizutani M, et al. Randomized phase III trial of trastuzumab monotherapy followed by trastuzumab plus docetaxel versus trastuzumab plus docetaxel as first-line therapy in patients with HER2-positive metastatic breast cancer: the JO17360 Trial Group. Breast Can Res Treat 2010; 119(1): 127-136.
Valero V, Forbes J, Pegram MD, et al. Multicenter phase III randomized trial comparing docetaxel and trastuzumab with docetaxel, carboplatin, and trastuzumab as first-line chemotherapy for patients with HER2-gene-amplified metastatic breast cancer (BCIRG 007 study): two highly active therapeutic regimens. J Clin Oncol 2011; 29(2): 149-156.
Andersson M, Lidbrink E, Bjerre K, et al. Phase III randomized study comparing docetaxel plus trastuzumab with vinorelbine plus trastuzumab as first-line therapy of metastatic or locally advanced human epidermal growth factor receptor 2-positive breast cancer: the HERNATA study. J Clin Oncol 2011; 29(3): 264-271.
Baselga J, Cortés J, Kim SB, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. NEJM 2012; 366(2): 109-119.
Swain SM, Kim SB, Cortés J, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA study): overall survival results from a randomised, double-blind, placebo-controlled, phase III study. Lancet Oncol 2013; 14(6): 461-471.
Scheuer W, Friess T, Burtscher H, et al. Strongly enhanced antitumor activity of trastuzumab and pertuzumab combination treatment on HER2-positive human xenograft tumor models. Cancer Res 2009; 69(24): 9330-9336
Marty M, Cognetti F, Maraninchi D, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005; 23(19): 4265-4274.
Verma S, Miles D, Gianni L, et al, for the EMILIA Study Group. Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. NEJM 2012; 367: 1783-179.
Gullo G, Zuradelli M, Sclafani F, et al. Durable Complete response following chemotherapy and trastuzumab for metastatic Her2+ breast cancer. Ann Oncol 2012: 23(8): 2204-2205
 (click to enlarge)
(click to enlarge)
