Many patients are diagnosed at an advanced stage of disease, which has historically been resistant to both chemotherapy and radiation. However there have been significant advances in treatment in the last decade. Optimisation of currently available agents and exploiting the efficacy of new therapies is critical
Dr MinYuen Teo, Research Registrar in Medical Oncology, Tallaght Hospital, Dublin and Dr Ray McDermott, Consultant Medical Oncologist, Tallaght Hospital, Dublin
Renal cell carcinoma (RCC) is the second most common urologic malignancy. Many patients are diagnosed at an advanced stage of disease, which has historically been resistant to both chemotherapy and radiation. However, management has undergone a paradigm shift in the last decade. A better understanding of disease biology has led to the introduction of small tyrosine kinase inhibitors (TKIs) targeting vascular endothelial growth factor (VEGF) and mammalian target of rapamycin (mTOR).
Sunitinib, pazopanib and bevacizumab, in combination with interferon, each have demonstrated efficacy in first-line therapy supported by level 1 evidence,1-4 while temsirolimus has been shown to be effective in poor-risk patients.5
Despite these new active therapies, the disease will inevitably progress and median overall survival remains in the range of 22 months.6 The next steps involve deepening our understanding of disease biology and optimisation of currently available agents.
Adjuvant therapy
In localised RCC, radical nephrectomy may be curative, however, relapses occur in 35-43%7 depending on the stage of disease. Features such as pathological tumour and nodal staging, size of tumour, nuclear grade and presence of histologic tumour necrosis have been recognised to influence the risk of recurrence.8
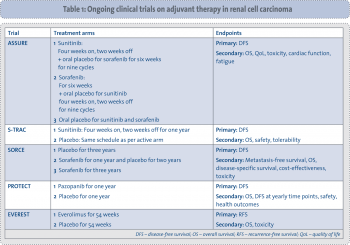
Adjuvant therapies after definite surgery with proven benefit to reduce recurrence are standard of care in cancers such as breast and colorectal.9,10 Prior studies examining the role of adjuvant immunotherapy with or without chemotherapy have been negative in renal cancer.11 The activity of VEGF TKIs and mTOR inhibitors in advanced disease has led to a number of major adjuvant studies: ASSURE (sunitinib versus sorafenib versus placebo for up to one year; NCT00326898); S-TRAC (sunitinib versus placebo for one year; NCT00375674); SORCE (sorafenib for one year versus three years versus placebo; NCT00492258); PROTECT (pazopanib versus placebo for one year; NCT01235962); and EVEREST (everolimus versus placebo for one year; NCT01120249) (see Table 1).
(click to enlarge)
Results are not yet available from any of these studies, however, they apply differing pathologic inclusion criteria to determine eligibility. This may complicate comparison of efficacy between agents, and also reflects the lack of a universally accepted definition of high-risk RCC.12 A recent analysis applied the differing entry criteria from these studies to over 1,300 patients from the nephrectomy registry of the Mayo Clinic and found that despite the variability in inclusion criteria, the studies had similar and relatively strong predictive accuracy for disease recurrence. Conversely, 6-18% of patients with a significant risk of recurrence were not eligible by these inclusion criteria.12
Cytoreductive nephrectomy
In the advanced disease setting, cytoreductive nephrectomy followed by interferon therapy was unequivocally shown to improve survival compared to interferon therapy only.13 Many observers proposed an immune-related mechanism although the precise mode of action remains unclear.14
Cytoreductive nephrectomy remains an effective palliative treatment option for tumour-related bleeding or intractable pain, however, the appropriateness of nephrectomy in the metastatic setting also depends on various patient and tumour-related factors.14 Relative contraindications include sarcomatoid histology, bulky osseous metastases, central nervous system or hepatic involvement and age over 75.14
Moreover, the role of cytoreductive nephrectomy in the era of active targeted therapies remains ill defined. Issues include the role of nephrectomy in improving survival in this era, the safety of surgery in anti-VEGF-treated patients, and the potential role of sunitinib and pazopanib as neoadjuvant therapy.
In a retrospective study, Margulis and colleagues found that pre-operative anti-VEGF therapy was safe and did not increase surgical morbidity or perioperative complications.15 However, these therapies appear to induce more shrinkage in the metastases rather than primary lesions,16,17 calling into question their role in disease downstaging.
Overall, the shrinkage of the primary lesion is in the order of 10%, which is insufficient to justify neoadjuvant therapy for downstaging.
A large multicentre analysis to identify prognostic factors for overall survival in patients treated with anti-VEGF therapies identified nephrectomy as a good prognostic indicator in univariate analysis but this significance was not retained in multivariate analysis.6
In a recently published retrospective study of over 300 patients, nephrectomy improved overall survival by 32% on multivariate analysis after controlling for other identified risk factors.18
Two currently-recruiting phase III trials aim to investigate the role of nephrectomy on survival in metastatic RCC treated with sunitinib (CARMENA; NCT00930033) and the role of delayed nephrectomy compared to immediate resection in patients treated with sunitinib (NCT01099423).
Current agents: combination
The three main classes of drugs used in the management of advanced RCC – immunotherapy, anti-VEGF agents and mTOR inhibitors – have differing modes of action. This has led to interest in combination therapies, exemplified by the recent success of such a strategy in breast cancer.19
In two large randomised phase III studies, bevacizumab – an antibody against VEGF – in combination with interferon has been shown to confer superior progression-free survival compared to interferon alone.1,3 Overall survival was not significantly different between arms but this was thought to be confounded by subsequent lines of active therapies. The toxicity of the combination is significant and may well be attributable to the interferon. Unfortunately, there are no data comparing bevacizumab monotherapy to the experimental arm in these studies.
Temsirolimus – an intravenous mTOR inhibitor given weekly – has also been combined with interferon in a poor-risk population. The combination was associated with a higher rate of toxicity and no greater activity than temsirolimus alone.5 Combining VEGF tyrosine kinase inhibitors such as sorafenib and sunitinib with interferon led to a high rate of toxicity, even at low doses.20
Attempts at combination of VEGF blockade and mTOR inhibition have also been met with limited success due to overlap in their toxicity profiles. The TORAVA study was a three-arm randomised phase II study pitting bevacizumab plus temsirolimus against sunitinib or bevacizumab plus interferon. The experimental arm reported inferior progression-free survival. Over 40% of patients stopped treatment secondary to toxicity, with a rate of grade 3 and 4 toxicity in excess of 70%.21
Ongoing trials such as INTORACT (NCT00631371), BeST (NCT00378703) and RECORD-2 (NCT00719264) are examining other combinations (see Table 2). The combination of bevacizumab with VEGF tyrosine kinase inhibitors is limited by a high rate of toxicities such as hypertension and proteinuria, as well as increased incidence of less common side-effects, such as micro-angiopathy, haemolytic anaemia and reversible posterior leukoencephalopathy syndrome.20
(click to enlarge)
Bevacizumab and interferon aside, the combination approach remains unproven as yet and has faced criticism for unacceptably high toxicity requiring dose reduction and uncertainty about true drug resistance upon progression.22
Current agents: sequencing
Due to the difficulties inherent in combining available agents, the sequential use of available agents has become standard care in everyday clinical practice. There is an accumulating evidence base derived from phase II and large randomised phase III studies including: the use of pazopanib after cytokines,4 sorafenib after immunotherapy in the TARGET study,23 everolimus as second or third-line therapy in the RECORD-1 study,24 and the recently published axitinib as second-line therapy in the AXIS study.25
Based on the available evidence, the principle question remains whether to use sequential VEGF inhibition, or a switch to mTOR inhibition following first-line anti-VEGF failure.
Moreover, the ideal sequencing of existing anti-VEGF TKIs remains uncertain. Although the target is the same, these drugs differ in their affinity for this target and also in their promiscuity for other targets. This is manifest in the toxicities associated with each VEGF TKI, which vary significantly. In addition to targeting VEGF, sorafenib also targets RAF kinase, which may be important in other cancer types.
Retrospective data have indicated that within a sequential regimen, progression-free survival can be improved by using sorafenib as first-line therapy followed by sunitinib,20, 26, 27 rather than the other way around. This strategy is currently being evaluated further in the randomised phase III SWITCH study (NCT00732914).
Data are more limited on sequential use of other VEGF TKIs. The AXIS study compared axitinib with sorafenib as second-line therapy and recruited over 700 patients. Fifty-four per cent of patients on each arm received prior sunitinib and reported progression-free survival of 4.8 and 3.4 months respectively,25 which was comparable to retrospective sorafenib data.27-29 Other anti-VEGF molecules which have shown activity as second-line therapy included linifanib30 and pazopanib;31 the latter is also the subject of an current phase II ICORG investigation (NCT01566747).
The largest dataset for mTOR inhibitors in sequence comes from the RECORD-1 study.32 Pre-planned subgroup analysis from the RECORD-1 study showed that everolimus demonstrated activity following either one or two lines of VEGF blockade33 with progression-free survival similar to that seen with axitinib in second-line use. There are limited data on the efficacy of temsirolimus following failure of VEGF blockade, mostly restricted to small retrospective studies.34,35 The largest series was reported by McKenzie and colleagues on 87 patients with intermediate-to-poor-risk renal cell carcinoma, with a time-to-progression of four months, suggesting activity.36
For the proportion of patients who retain a good performance status, management upon progression beyond available agents poses a significant challenge. Small retrospective studies suggest that anti-VEGF rechallenge following everolimus resistance may be effective,37,38 however, new agents with alternative mechanisms of action are required.
Refractory disease
Sunitinib and pazopanib are the most active single agents available for the management of advanced renal cell carcinoma in first-line treatment. Each confers a response rate of approximately 30% and disease stabilisation rates of 38-48%.2,4 However, up to a quarter of all patients treated with VEGF tyrosine kinase inhibitors have progressive disease at first evaluation. These patients have uniformly poor responses to second-line VEGF blockade or indeed mTOR inhibition, and overall survival remains poor.
Although this cohort contains many poor-risk patients and sarcomatoid tumours, approximately 50% of patients with primary refractory disease fall into good and intermediate risk groups. This suggests that the known clinical prognostic factors are not sufficiently robust to identify patients with primary refractory disease.39 Anecdotal efficacy of cytotoxic chemotherapy in this cohort has been reported40 and prospective studies for this substantial minority are needed.
New agents
Axitinib, a TKI for VEGFR-1, -2 and -3, is the latest agent added to the armamentarium of therapies against advanced RCC.25 Other anti-angiogenic agents in the advanced stage of development include tivozanib and dovitinib.41 The latter is of particular interest as it targets fibroblast growth factor receptor (FGFR) in addition to VEGF. FGFR is widely thought to be a tumour escape mechanism in response to sustained anti-VEGF therapy, and therefore responsible for the development of therapeutic resistance.42
Nonetheless, it is becoming apparent that approaches which go beyond targeting VEGF will be required to enhance outcomes for patients with this disease. Strategies under evaluation include inhibition of the Ang/Tie2 pathway, immunotherapy with CTLA-4 inhibition or anti-PD1 inhibition and vaccine development.43
Adjunctive therapies
Skeletal metastases affect up to one-third of all patients with metastatic renal cell carcinoma. In an analysis of over 800 patients, 32% of patients were afflicted with osseous metastasis, half of which were present at diagnosis and the remainder of which developed bony involvement during the course of their illness.44 It was estimated that each patient with bone metastasis experienced 2.4 skeletal-related events, most commonly bony pain necessitating radiotherapy (60.9%), fractures (20%) and malignant cord or nerve root compression (11%).44 Indeed, it has been suggested – based on analysis of over 200 cases of advanced disease – that osseous involvement by metastatic RCC is a poor prognostic indicator, predicting shorter progression-free survival and poorer overall survival.45
Bisphosphonates such as zoledronic acid have been shown in multiple tumour types to reduce skeletal-related events. In a subset analysis of renal cell cancer cases, which constituted 10% of the entire cohort, zoledronic acid reduced the average rate of skeletal-related events and significantly prolonged time to first event.46,47 Keizman and colleagues also reported that bisphosphonates in RCC might improve progression-free and overall survival in a retrospective study.48
Conclusion
The landscape of RCC has changed significantly since 2004, with the introduction of several active targeted therapies. As we move beyond the initial phase of familiarising ourselves with these new agents, their cytostatic properties and different side-effect profiles, larger questions have begun to present themselves.
Adjuvant therapy has historically been ineffective in RCC, and the reproducibility of the activity of targeted therapies in the adjuvant setting remains to be elucidated.
In the management of metastatic RCC, combination approaches have been confounded by limited efficacy and substantial toxicity. Sequential monotherapy has become the mainstay of day-to-day clinical practice, however, the correct sequencing remains uncertain. Primary refractory disease and osseous metastases have been recognised as poor prognostic indicators.
The treatment of advanced RCC appears set to become more complex with further anti-VEGF agents at an advanced stage, and new agents with different targets in development. While the goal of cure remains elusive, trials examining optimisation of existing agents and efficacy of new therapies represent a critical step forward.
References
Escudier B, Pluzanska A, Koralewski P et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase III trial. Lancet 2007; 370: 2103-2011
Motzer RJ, Hutson TE, Tomczak P et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. NEJM 2007; 356: 115
Rini BI, Halabi S, Rosenberg JE et al. Bevacizumab plus interferon alfa compared with interferon alfa monotherapy in patients with metastatic renal cell carcinoma: CALGB 90206. J Clin Oncol 2008; 26: 5422-5428
Sternberg CN, Davis ID, Mardiak J et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized phase III trial. J Clin Oncol 2010; 28(6): 1061-1068
Hudes G, Carducci M, Tomczak P et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. NEJM 2007; 356: 2271-2281
Heng DY, Xie W, Regan MM et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: Results from a large, multicenter study. J Clin Oncol 2009; 27(34): 5794-5799
Stephenson AJ, Chetner MP, Rourke K et al. Guidelines for the surveillance of localized renal cell carcinoma based on the patterns of relapse after nephrectomy. J Urology 2004; 172: 58-62
Leibovich BC, Blute ML, Cheville JC et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer 2003; 97: 1663-1671
Andre T, Boni C, Navarro M et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol 2009; 27: 3109-3116.
Peto R, Davies C, Godwin J et al. Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet 2012; 379: 432-444
Atzpodien J, Schmitt E, Gertenbach U et al. Adjuvant treatment with interleukin-2- and interferon-alpha2a-based chemoimmunotherapy in renal cell carcinoma post tumour nephrectomy: results of a prospectively randomised trial of the German Cooperative Renal Carcinoma Chemoimmunotherapy Group (DGCIN). Br J Cancer 2005; 92: 843-846
Kim SP, Crispen PL, Thompson RH et al. Assessment of the pathologic inclusion criteria from contemporary adjuvant clinical trials for predicting disease progression after nephrectomy for renal cell carcinoma. Cancer 2012: online 3 Jan
Flanigan RC, Salmon SE, Blumenstein BA et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. NEJM 2001; 345: 1655-1659
Abel EJ, Wood CG. Cytoreductive nephrectomy for metastatic RCC in the era of targeted therapy. Nature Reviews Urol 2009; 6: 375-383
Margulis V, Matin SF, Tannir N et al. Surgical morbidity associated with administration of targeted molecular therapies before cytoreductive nephrectomy or resection of locally recurrent renal cell carcinoma. J Urol 2008; 180: 94-98
Bex A, Blank C, Meinhardt W, van Tinteren H, Horenblas S, Haanen J. A phase II study of presurgical sunitinib in patients with metastatic clear-cell renal carcinoma and the primary tumor in situ. Urology 2011; 78: 832-837
Park I, Ahn Y, Park K et al. Does primary lesion have to be regarded as a target lesion when evaluating response in metastatic renal cell carcinoma (mRCC) treated with sunitinib? J Clin Oncol 2012; 30(5 Suppl) 2012; Abstr 425
Choueiri TK, Xie W, Kollmannsberger C et al. The impact of cytoreductive nephrectomy on survival of patients with metastatic renal cell carcinoma receiving vascular endothelial growth factor targeted therapy. J Urol 2011; 185: 60-66
Baselga J, Campone M, Piccart M et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. NEJM 2012; 366: 520-529
Porta C, Szczylik C, Escudier B. Combination or sequencing strategies to improve the outcome of metastatic renal cell carcinoma patients: A critical review. Crit Rev Oncol/Hematol 2011; in press
Negrier S, Gravis G, Perol D et al. Temsirolimus and bevacizumab, or sunitinib, or interferon alfa and bevacizumab for patients with advanced renal cell carcinoma (TORAVA): a randomised phase II trial. Lancet Oncol 2011; 12: 673-680
Escudier B, Eisen T, Stadler WM et al. Sorafenib in advanced clear-cell renal-cell carcinoma. NEJM 2007; 356: 125
Motzer RJ, Escudier B, Oudard Sp et al. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet 2008; 372: 449-456
Rini BI, Escudier B, Tomczak P et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase III trial. Lancet 2011; 378: 1931-1939
Merseburger AS, Simon A, Waalkes S, Kuczyk MA. Sorafenib reveals efficacy in sequential treatment of metastatic renal cell cancer. Expert Rev Anticancer Ther 2009; 9: 1429-1434
Porta C, Tortora G, Linassier C et al. Maximising the duration of disease control in metastatic renal cell carcinoma with targeted agents: an expert agreement. Medical Oncol; First Online July 2011
Dudek AZ, Zolnierek J, Dham A, Lindgren BR, Szczylik C. Sequential therapy with sorafenib and sunitinib in renal cell carcinoma. Cancer 2009; 115: 61-67
Sablin MP, Negrier S, Ravaud A et al. Sequential sorafenib and sunitinib for renal cell carcinoma. J Urol 2009; 182: 29-34
Tannir N, Wong Y, Kollmannsberger C et al. Phase II trial of linifanib in patients with advanced renal cell cancer (RCC) after sunitinib failure. J Clin Oncol 2010; 28(15 Suppl) 2010: Abstr 4527
Reeves JA, Spigel D, Daniel DB, Friedman EK, Burris HA, Hainsworth JD. Pazopanib in patients with metastatic renal cell carcinoma previously treated with sunitinib or bevacizumab: A Sarah Cannon Research Institute phase II trial. J Clin Oncol 2011; 29 (15 Suppl): Abstr 4659
Motzer RJ, Escudier B, Oudard Sp et al. Phase 3 trial of everolimus for metastatic renal cell carcinoma. Final results and analysis of prognostic factors 2010; 116: 4256-4265
Calvo E, Escudier B, Motzer RJ et al. Everolimus in metastatic renal cell carcinoma: Subgroup analysis of patients with 1 or 2 previous vascular endothelial growth factor receptor-tyrosine kinase inhibitor therapies enrolled in the phase III RECORD-1 study. Eur J Cancer 2012; 48: 333-339
Gerullis H, Bergmann L, Maute L et al. Feasibility of sequential use of sunitinib and temsirolimus in advanced renal cell carcinoma. Medical Oncol 2009; 27: 373-378
Grundbichler M, Mlineritsch B, Ressler S et al. Efficacy of temsirolimus after previous treatment with sunitinib, sorafenib or everolimus in advanced renal cell cancer. Oncol 2011; 80: 34-41
MacKenzie MJ, Rini BI, Elson P et al. Temsirolimus in VEGF-refractory metastatic renal cell carcinoma. Annals Oncol 2010; 22: 145-148
Grünwald V, Seidel C, Fenner M, Ganser A, Busch J, Weikert S. Treatment of everolimus-resistant metastatic renal cell carcinoma with VEGF-targeted therapies. Br J Cancer 2011; 105: 1635-1639
Zama IN, Hutson TE, Elson P et al. Sunitinib rechallenge in metastatic renal cell carcinoma patients. Cancer 2010; 116: 5400-5406
Heng DY, MacKenzie MJ, Vaishampayan UN et al. Primary anti-vascular endothelial growth factor (VEGF)-refractory metastatic renal cell carcinoma: clinical characteristics, risk factors, and subsequent therapy. Annals Oncol; First Online Nov 2011
Richey SL, Ng C, Lim ZD, Jonasch E, Tannir NM. Durable remission of metastatic renal cell carcinoma with gemcitabine and capecitabine after failure of targeted therapy. J Clin Oncol 2011; 29(8): e203-205
Gross-Goupil M, Massard C, Ravaud A. Targeted therapies in metastatic renal cell carcinoma: Overview of the past year. Curr Urol Reports 2011; 13: 16-23
Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumors. Cancer cell 2005; 8: 299-309
Pal SK, Williams S, Josephson DY, Carmichael C, Vogelzang NJ, Quinn DI. Novel therapies for metastatic renal cell carcinoma: efforts to expand beyond the VEGF/mTOR signaling paradigm. Molecular Cancer Therapeut 2012; 11: 526-537
Woodward E, Jagdev S, McParland L et al. Skeletal complications and survival in renal cancer patients with bone metastases. Bone 2011; 48: 160-166
Beuselinck B, Oudard S, Rixe O et al. Negative impact of bone metastasis on outcome in clear-cell renal cell carcinoma treated with sunitinib. Annals Oncol 2010; 22(4): 794-800
Lipton A, Zheng M, Seaman J. Zoledronic acid delays the onset of skeletal-related events and progression of skeletal disease in patients with advanced renal cell carcinoma. Cancer 2003; 98: 962-969
Rosen LS. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: A phase III, double-blind, randomized trial. The Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group. J Clin Oncol 2003; 21: 3150-3157
Keizman D, Ish-Shalom M, Pili R et al. Bisphosphonates combined with sunitinib may improve the response rate, progression free survival and overall survival of patients with bone metastases from renal cell carcinoma. Eur J Cancer 2012; Mar 10 Epub Ahead of Print
 (click to enlarge)
(click to enlarge)
