Repeat prescribing of strong opioids in Irish general practice
A general practice study has shown that strong opioids are most commonly prescribed for back or joint pain, and highlights the urgent need for Irish guidelines on opioid use in primary care
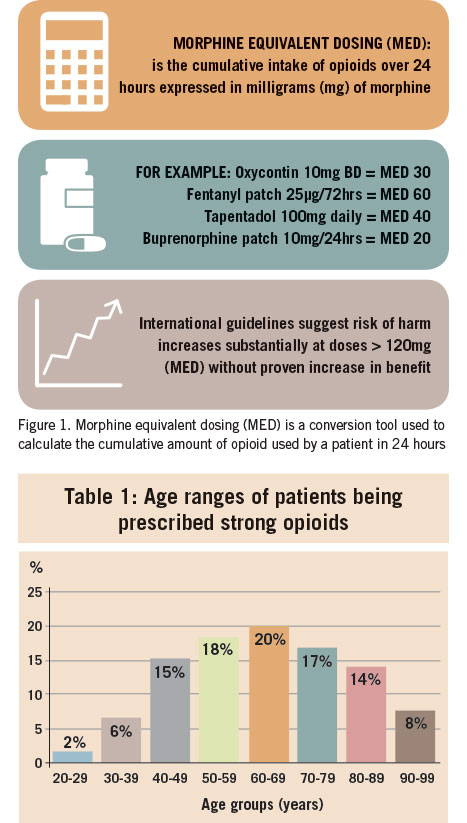
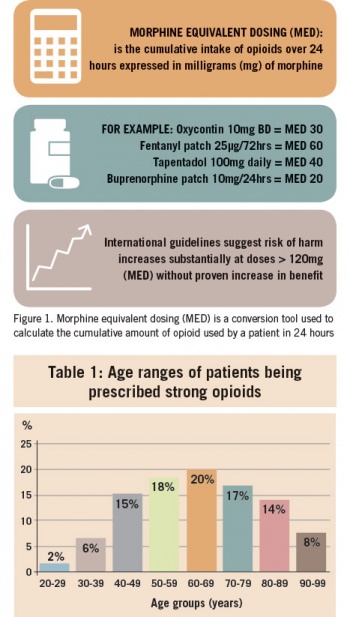
Internationally, a marked increase in opioid prescribing has coincided with a dramatic rise in opioid-related deaths and overdoses.1 Opioid analgesia can be effective for selected patients but evidence for its use in chronic non-cancer pain (CNCP) is lacking. American guidelines recommend that therapy should be maintained at low doses, defined as up to 40 morphine equivalent dosing (MED).2 MED is a conversion tool used to calculate the cumulative amount of opioid used by a patient in 24 hours.3 Higher MEDs, particularly those greater than 120, increase the risk of side-effects, overdose and death (see Figure 1).
In Ireland, prescriptions for opioids increased by almost 50% between 2009 and 2017.4 However, currently no official Irish guidelines exist for the management of CNCP. This leaves GPs in a vulnerable position when it comes to opioid prescribing.
Our study aimed to explore current opioid prescribing practice for CNCP in Irish general practice. Our primary outcomes were to identify whether opioid doses were escalating over time and by whom strong opioids were being prescribed. A secondary outcome was to identify the role of pain teams and to measure the prevalence of co-prescribing of other potentially harmful medications. This is the first study to describe recent trends in strong opioid prescribing in Irish general practice
Patient databases from four practices (two inner-city, one urban and one rural) were searched over a three-month period to identify adults receiving repeat prescriptions of strong opioids (defined as morphine, fentanyl, oxycodone, tapentadol, buprenorphine, dihydromorphine and meptazinol). A repeat prescription was defined as a prescription issued for three consecutive months. Nursing and residential home patients were excluded, as were patients with an active cancer diagnosis or active palliative care involvement.
(click to enlarge)
The information recorded for each patient included the indication for opioid treatment, initial prescribing source (eg. GP or other) and whether or not the patient had attended a pain team. The MED was calculated for each strong opioid prescription at two time-points: at initiation and currently, using validated conversion tools.5,6 Patient files were also reviewed for co-prescription of benzodiazepines, z-drugs, gabapentinoids (pregabalin and gabapentin) and weak opioids (codeine-containing medications and tramadol). Of note, weak opioids were excluded from the MED calculation.
Results
A total of 185 patients were included in the analysis. Of these, 111 (60%) were female and 74 (40%) were male. The youngest patient was 20 years old and the oldest was 97, with the median age being 66. Strong opiates were most frequently prescribed for those aged 60-69 years while those aged 20-29 years received the fewest prescriptions (see Table 1).
Indications for strong opioid prescriptions
The majority of prescriptions were initiated for lower back pain (44%) and joint pain (32%). Chronic pain syndromes such as fibromyalgia and chronic pelvic pain accounted for 5% of prescriptions, neuropathic pain for 4%, peripheral vascular disease for 4% and fracture for 4%.
In one patient’s case, there was no documented indication for opioid therapy.
Initiation of strong opioid prescription
GPs had initiated the strong opioid prescription in 120 (65%) cases. Pain teams had initiated 27 (15%) while 32 (17%) had been started by other specialties. Only 2% had been started in an emergency department.
For two patients, it was unclear from records where the opioid was initiated.
Pain team involvement
Of the 185 patients, 73 (39%) had attended a pain clinic while an additional 11 (6%) had been referred but were awaiting an appointment. A further 99 (54%) patients on strong opioids had never been referred to or attended a pain clinic. Two patients had been referred to the pain clinic by their GP but did not attend.
Morphine equivalent dose (MED)
Of the 185 patients assessed, 81 (43%) had their MED increased since initiation, 70 (37%) did not have their MED changed over the course of their treatment and 34 (18%) had their MED decreased.
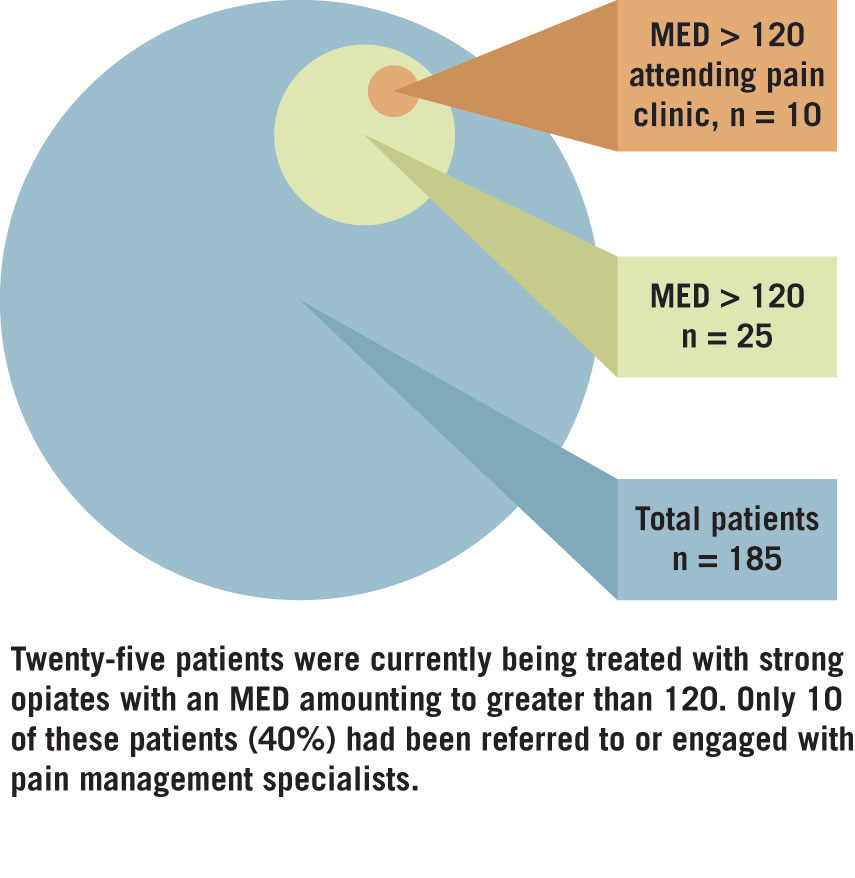
Twenty-five (13%) patients were being treated with strong opioids with an MED in the ‘hazardous’ range (120 or greater); however only 10 of these had attended a pain clinic (see Table 2).
Co-prescribed medications
In addition to receiving a prescription for a strong opioid, 133 (72%) patients were being co-prescribed at least one other medication with potential for sedation, overdose or dependence. Of the total prescriptions issued for these co-prescribed medications, the majority were for gabapentinoids (34%) and benzodiazepines (33%), followed by weak opioids (21%) and z-drugs (12%).
A modern dilemma
Providing safe, appropriate and effective management of CNCP is a dilemma facing modern medicine. This retrospective cross-sectional study which was prompted by the opioid crisis in the US and UK describes current trends in opioid prescribing in the Irish primary care setting.
Our results were consistent with previously published studies showing that opioids were prescribed more frequently in females, with the most common indications being lower back pain and joint pain.7,8
(click to enlarge)
This study highlights the potential of using MED calculators when prescribing opioids. MED provides an objective assessment of opioid exposure and is a useful tool in identifying those exposed to large opioid doses. Currently there is no accepted definition of opioid overprescribing but it has been shown that there is a clear increase in morbidity and mortality at MED greater than 120.9 MED may be used to track escalations in opioid dosages over time, to risk-stratify patients and to guide treatment and referral decisions, perhaps as an inbuilt MED calculator into practice software.
Pain specialists are becoming a cornerstone in chronic pain management; however, a minority of patients in this study had attended a pain clinic and the majority of opioid prescriptions had been initiated in primary care. It was suggested in 2013 by the ICGP that pain specialists should be involved once the MED has reached over 120, but in our study this had occurred in only 40% of cases.10 A clear referral pathway and identifiable treatment goals are required for optimum collaborative management of CNCP between primary and secondary care.
The fact that the vast majority of patients being prescribed strong opioids were also being co-prescribed at least one benzodiazepine, z-drug, weak opioid or gabapentinoid is testament to the complex nature of chronic pain while highlighting the need for caution, as combinations of these drugs have been repeatedly linked to a myriad individual and public harms, including dependence, diversion and death.11,12,13
Limitations of study
Several limitations of this study warrant consideration. We excluded nursing homes and residential care homes due to difficulty in accessing previous records and prescriptions. We did not attempt to relate opioid prescriptions with treatment effectiveness either in terms of measuring quality of life, pain control or functional ability.
Furthermore, we did not seek to identify which indications were associated with higher MED. Future research may consider effectiveness of treatment while identifying indications associated with downstream risk of sustained use and high dose exposure. It is also important to note when viewing the results of this study that weak opioids were not included in the MED calculation. One patient had an MED of 37, but when weak opioids were taken into consideration the combined MED increased to greater than 120. Furthermore, 18% had a reported decrease in MED since initiation but if calculated with weak opioids this may not have been the case.
Our study provides a snapshot of opioid dose exposure at two timepoints: at initiation and currently. It was not practical to record dose fluctuations over time. These limitations support the need for MED calculators when issuing prescriptions at patient level so that objective monitoring of treatment and awareness of hazardous levels can occur.
Conclusion
Management of CNCP is complex and patients are at risk of overtreatment and polypharmacy. There is an immediate need for Irish guidelines regarding opioid use in primary care. Collaborative management between GPs and pain specialists adopting a multimodal approach to the management of CNCP is the ultimate goal, with safe prescribing of opioids as part of a broader biopsychosocial approach.
References
Manchikanti L, Helm S II, Fellows B, et al. Opioid Epidemic in the United States. Pain Physician 2012;15(3l):9-38
Manchikanti L, Kaye AM, Knezevic NN et al. Responsible, Safe, and Effective Prescription of Opioids for Chronic Non-Cancer Pain: American Society of Interventional Pain Physicians (ASIPP) Guidelines. Pain Physician 2017 Feb; 20(2S):S3-S92
McDermott S. The rise of opiates: How Ireland’s ‘broken’ health service is behind a surge in prescription painkillers. 2018. thejournal.ie Date viewed 25/4/19 <http://jrnl.ie/4230482> __The figures in this article were based on data obtained under FOI. This data was obtained by us via the author and reviewed prior to quoting these figures in this article._
Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain2006;10:287-333
Serdarevic M, Striley CW, Cottler LB. Gender Differences in Prescription Opioid Use. Curr Opin Psychiatry 2017; 30(4): 238-246
Quinn, P. et al. Prescription opioid duration and dose: associations with substance use disorder events. The Journal of Pain , 2017; 18(4): S36-S37
Power C, Delargy I, Gregan P, Gallagher H: Guidelines for Opioid Prescribing in Chronic Pain. ICGP Summer School 2013
Sun EC, Dixit A, Humhreys K. Association between concurrent use of prescription opioids and benzodiazepines and overdose: retrospective analysis. BMJ 2017 Mar 14;356:j760. doi: 10.1136/bmj.j760
Gomes T, Greaves S, van den Brink W, Antoniou T, Mamdani MM, Paterson JM, et al. Pregabalin and the Risk for Opioid-Related Death: A Nested Case–Control Study. Ann Intern Med. 2018;169:732–734. doi: 10.7326/M18-1136
Zeng C, Dubreuil M, LaRochelle M. Association of tramadol with all-cause mortality among patients with osteoarthritis. JAMA 2019; 321(10): 969-982
 (click to enlarge)
(click to enlarge)