In modern Ireland it is simply unacceptable that every year young women and men are dying of preventable human papillomavirus (HPV)-driven cancers. We have overwhelming evidence that we can stop this from happening. The HPV vaccine is one of the outstanding scientific achievements in modern times, with the first dose administered in Australia in 2006.
If evidence-based medicine is our mantra then anecdotal information has no substance and no value. The positive results from this vaccine are staggering. Repeated clinical multicentre trials all around the globe have concluded with the same findings – this vaccine is highly effective and has an excellent safety profile.1,2,3
GPs in Ireland have an essential role to play in detecting, treating and preventing HPV-driven benign and malignant disease. This article will review the origins of the virus, the carcinogenic process, malignant and benign manifestations of HPV, oncological therapy and why the HPV vaccine is one of the safest vaccines ever produced.
Clinical case report
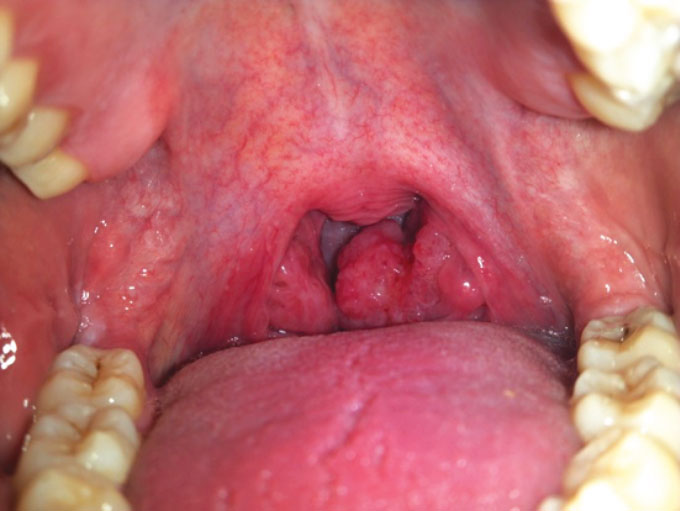
A 55-year-old patient identified an irregularity in his left tonsil and decided to monitor the tonsil with a series of ‘selfies’ without medical intervention. The initial image is from March 2013 but no help was requested until 27 months later when otalgia (referred pain from the glossopharyngeal nerve) and a gradual concern over the appearance of the tonsil prompted a consultation with the patient’s GP.
(click to enlarge)
(click to enlarge)
(click to enlarge)
(click to enlarge)
The patient was immediately referred to the head and neck service given the obvious appearance of the tonsil and concern over possible cervical nodal spread. The GP noted the patient was a non-smoker with occasional alcohol intake and no other significant medical issues. The patient worked in insurance and was married with three children.
The patient was reviewed in the head and neck clinic where a full history and examination was repeated, including an endoscopic visualisation of all mucosal sites of the laryngopharynx and a digital palpation of the tonsillar mass which confirmed a hard ulcerated lesion measuring over 4cm in size.
A biopsy was performed and a number of radiological investigations were requested. CT imaging of the neck and chest was performed and the patient was sent for a PET scan. A multidisciplinary team meeting confirmed T3 N1 oropharyngeal (tonsil) primary cancer with one ipsilateral cervical node with cancer dissemination. The tonsil histopathology reported a non-keratinising basaloid squamous cell carcinoma which was ‘p16’ positive.
These are the classic features of a viral-driven cancer caused by human papillomavirus. The patient was treated with concurrent chemo-radiotherapy and made a full recovery with no evidence of disease recurrence on repeated follow-up consultations.
What is human papillomavirus?
HPV are small, 50-55nm in diameter, non-enveloped double-stranded DNA viruses, which carry out their life cycle in either mucosal or cutaneous epithelia.
Over 200 types are known and more than 40 types are transmitted through sexual contact. HPV infection is very common and the vast majority of sexually active adults will have been exposed to HPV at some stage in their life.
The typical transmission for HPV is by having vaginal, anal or oral sex with someone who has the virus. It is most commonly spread during vaginal or anal sex. It is also possible to contract HPV without intercourse but through close skin to skin contact.
HPV causes cancers of the anogenital tract and in the reticulated tissue of the palatine and lingual tonsillar tissue in the head and neck. HPV also causes benign disease from simple warts to genital warts (HPV type 6 and 11) and recurrent respiratory papillomatosis of the larynx or trachea (see Figures 6 and 7).
(click to enlarge)
(click to enlarge)
A dozen HPV types (including types 16, 18, 31, and 45) are called ‘high-risk’ types. Co-factors such as cigarette smoke can also enhance the risk of such HPV-related cancers. HPV16 is the most dangerous oncogenic strain, causing the majority of cervical, anogenital and head and neck cancers.
Unfortunately, humans mount a poor immunological response to HPV. We have little immunological protection against a subsequent re-infection by the same HPV subtype strain and no additional protection to a different strain. After HPV exposure, approximately 70-80% of women seroconvert and it takes 8-12 months to detect specific antibodies. Response is typically low titre and avidity.
Men rarely seroconvert and if they do it is of no protective value. Approximately 5-10% of HPV infections become persistent and within months or years this may lead to premalignant or dysplastic change. Dysplasia is a permanent abnormal maturation of the epithelium. In the head and neck there is an approximate 30% conversion from high-grade dysplasia to invasive disease.
Worldwide burden of HPV disease
HPV is the most common sexually transmitted infection globally.4 Approximately 291 million women worldwide are carriers of HPV DNA, of which 32% are infected with the high-risk subtypes HPV16 or HPV18, or both. The Globocan data published in 2017 reported 630,000 HPV cancers globally per annum with 530,000 cervical cancer cases per year.4 Two-thirds of these cases are in the developing world and nearly half of the cervical cancers were diagnosed in women under 50 years of age. A shocking 266,000 women die of this preventable disease every year. Anogenital cancers (vulvar, vaginal, anal, penile) amounted to 68,000 cases per annum and 38,000 per annum head and neck cancers.4
In Ireland, the Irish Cancer Society has reported 420 HPV cancers per year between 2010 and 2014.5 Three hundred Irish women will be diagnosed with cervical cancer every year and 90 of these women will die from the illness. Overall, there are approximately 130 HPV deaths in Ireland per year and 6,500 pre-cancer HPV cervical procedures are performed; 1,843 anogenital warts were reported and treated in 2015 alone.6 These figures highlight the burden of HPV disease in this country and indicate the significant costs associated with therapy.
The International Journal of Cancer in 2017 tells us that of these 630,000 new HPV cases per annum, type 16 and 18 contributes 72.4%.4 That amounts to 460,000 people.
Years ago we dreamed of a ‘cancer vaccine’. It seemed a thing of the future; something aspirational but impossible. Thankfully due to the efforts of two exceptional scientists – Dr Jian Zhou and Prof Ian Frazer – we have a highly effective safe vaccine that covers type 16 and 18. To quote the Minister of Health in Australia “The jury’s not out (with this vaccine), the jury’s in!”
The head and neck cancer carcinogenic process
HPV-positive oropharyngeal squamous cell carcinoma (SCC) results in a non-keratinising ‘basaloid’ appearance. Infection and integration of high-risk HPV into host genomic material induces genomic instability in the host and also alters gene expression in the virus. When integrated, two oncoproteins, E6 and E7 are overexpressed. This disrupts normal growth control in response to environmental cues, or can dismantle cell cycle checkpoints that otherwise limit cell division or that induce cell suicide in response to DNA damage or oncogene activation. RB (retinoblastoma protein) and p53 are central to these processes.
HPV-positive tumours are more likely to have p53 degradation and RB inactivation with resulting p16 upregulation. P16 is a tumour suppressor protein. We test for p16 positivity in HPV-driven oropharyngeal cancers which in keeping with their unique non-keratinising basaloid histopathological features secures the diagnosis.
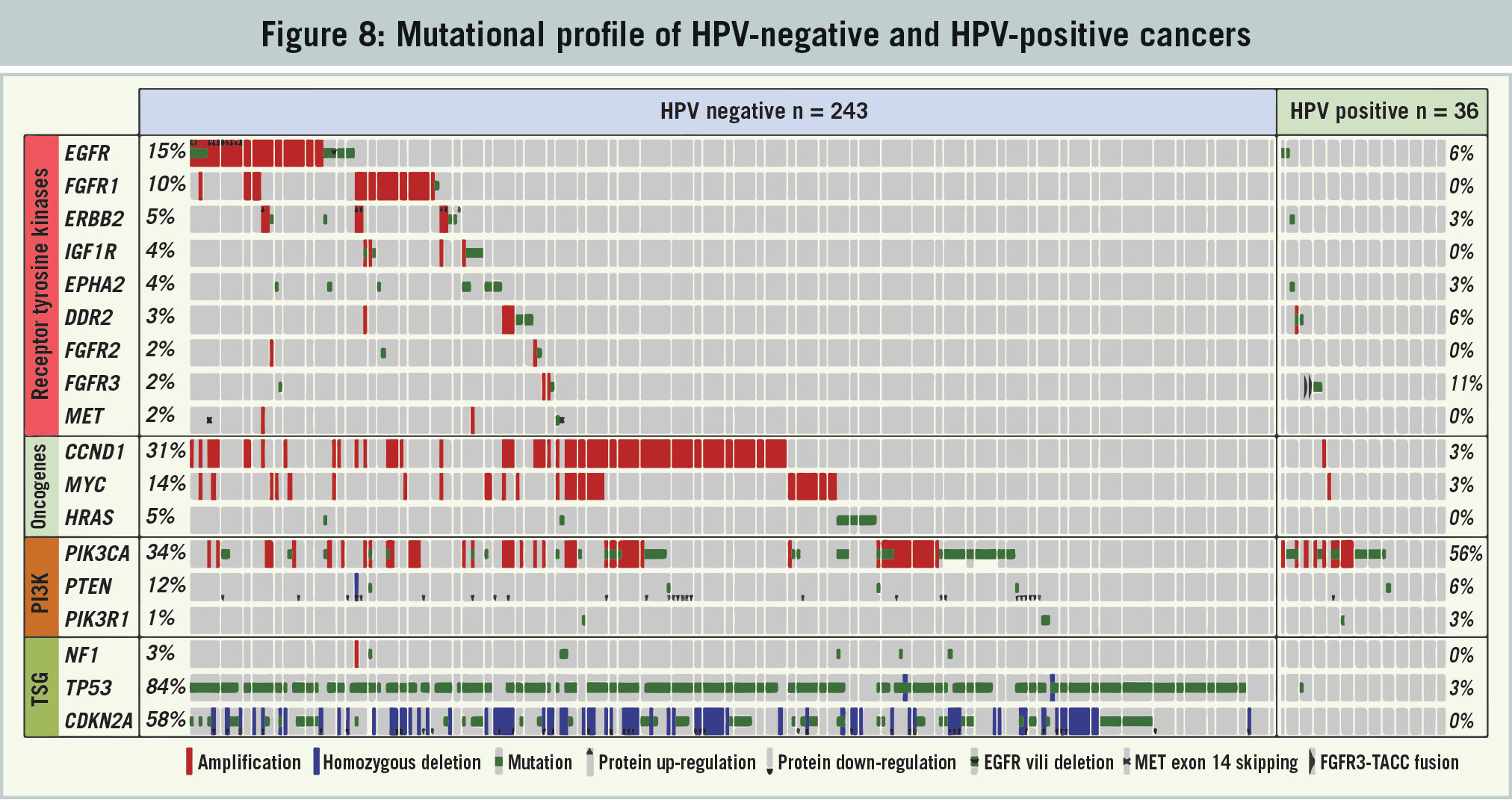
This is a viral carcinogenic squamous cell carcinoma process that is completely different to the chemical carcinogenic squamous cell carcinoma process from smoking and drinking, which are more commonly seen in the head and neck. Figure 8 illustrates the mutational expression of HPV-negative and HPV-positive oropharyngeal cancers. Every colour is a mutation and clearly HPV-positive SCC have far fewer mutations.
(click to enlarge)
Mutations result in a ‘smarter’ cancer, hence with a lesser mutational profile these HPV cancers respond in a more positive fashion to a cytotoxic agent and are highly responsive. Thus, patients who are p16 HPV positive have a clinical advantage. This could be appreciated in the clinical case report.
In the setting of standard (chemical carcinogenic) HPV- negative ‘common-or-garden variety’ SCC, the patient in the earlier case report would have died from rapid dissemination of disease, especially given the delay in oncological intervention.
What is also interesting is that this patient had cervical nodal dissemination. Nodal dissemination of oropharyngeal cancer occurs in up to 85% of HPV-positive and negative cases. In HPV-negative SCC patients, this reduces survival by 50% and is the most significant prognosticator. This notable drop in survival with cervical nodal dissemination is not appreciated in HPV-positive SCC and is a fundamental prognostic difference in these two diseases. It is interesting to note that by 2020 in the US, HPV-positive oropharyngeal SCC will surpass cervical cancer.
How does the HPV vaccine work?
The host’s immune response to HPV infection (humoral immunity, mainly IgG) is usually slow, weak and varies considerably among women. The HPV vaccine was developed as a result of the achievement of core technologies able to produce virus-like particles (VLPs). The vaccine is essentially a proteinacous shell (a HPV-type specific empty shell) of VLPs.
Recombinant DNA was used to generate VLPs capable of mimicking the natural virus and eliciting high-titers of virus neutralising antibodies. The vaccine is not infectious (contains no live virus) nor is it oncogenic. A rapid, potent, and sustained immunologic response is seen as a result of the administration of the quadrivalent vaccine (Gardasil) targeting HPV 6, 11, 16, and 18.
The longest follow-up of a clinical trial evaluating the efficacy, immunogenicity and safety of a licensed HPV vaccine to date was over 9.4 years.2 All vaccines remained seropositive to HPV16/18, with antibody titers remaining several folds above natural infection levels, as measured by ELISA, and there were no safety concerns.
There are two HPV vaccines available in Ireland. Gardasil, which is used in the HSE vaccination programme and therefore referred to in the rest of this article, protects against HPV types 6, 11, 16, 18, and is licensed from the age of nine years for the prevention of:
Premalignant genital lesions (cervical, vulvar and vaginal), premalignant anal lesions, cervical cancers and anal cancers causally related to certain oncogenic human papillomavirus (HPV) types
Genital warts (condyloma acuminata) causally related to specific HPV types.
The other available vaccine is Cervarix, which protects against HPV types 16 and 18, and is licensed from the age of nine years for the prevention of premalignant ano-genital lesions (cervical, vulvar, vaginal and anal) and cervical and anal cancers causally related to certain oncogenic human papillomavirus (HPV) types.
HPV vaccines are not licenced for the prevention of HPV-related head and neck cancers.
Is the HPV vaccine effective?
The HPV vaccine provides almost 100% protection from HPV types 6, 11, 16 and 18 if the doses are received at the correct intervals, and if it is given before you have an infection with these types.1 Australia introduced its national HPV vaccination programme in 2007 and over nine million doses of the vaccine have been given to girls and young women. Studies have shown early signs of the vaccine’s success, including a 77% reduction in HPV types responsible for almost 75% of cervical cancer, an almost 50% reduction in the incidence of high-grade cervical abnormalities in girls under 18 years of age and a 90% reduction in genital warts in heterosexual men and women under 21 years of age.7
When we look at real world evidence, a study in 20161 that reported results from observational studies from January 2007 through February 2016 to identify the impact or effectiveness of 4vHPV vaccination on infection, anogenital warts, and cervical cancer or pre-cancerous lesions, showed the impressive impact of vaccination, especially when we know that the full potential of this vaccine has not been realised to date.
Over the last decade, the impact of HPV vaccination in real-world settings has become increasingly evident, especially among girls vaccinated before HPV exposure in countries with high vaccine uptake.7 Maximal reductions of approximately 90% for HPV 6/11/16/18 infection, approximately 90% for genital warts, approximately 45% for low-grade cytological cervical abnormalities, and approximately 85% for high-grade histologically-proven cervical abnormalities have been reported.
Where HPV vaccination programmes have been implemented effectively, the benefits are already very apparent. Several countries that have introduced HPV vaccines to their immunisation programme have reported a 50% decrease in the incidence rate of uterine cervix pre-cancerous lesions among younger women.
In contrast, the mortality rate from cervical cancer in Japan, where HPV vaccination is not proactively recommended, increased by 3.4% from 1995 to 2005 and is expected to increase by 5.9% from 2005 to 2015. This acceleration in disease burden is particularly evident among women aged 15-44 years.4
(click to enlarge)
Is the HPV vaccine safe?
The World Health Organization (WHO) Global Advisory Committee for Vaccine Safety (GACVS) has never reported safety concerns with the HPV vaccine.8 They have reviewed the evidence on the safety of Gardasil vaccine on seven occasions – in 2007, 2008, 2009, 2013, 2014, 2015, 2017. As part of the 2017 review, 79,697 serious adverse events were investigated and the conclusion reached was that HPV vaccines are considered to be extremely safe.9
However no vaccine or drug is 100% safe. Concerns about the vaccine fall into four main categories; chronic fatigue, complex regional pain syndrome, postural orthostatic tachycardia syndrome and autoimmune disease. Millions of girls have been investigated in pre- and post-licensure investigations and it is consistently reported there is no evidence these syndromes are associated with HPV vaccination. The numbers of patients presenting with these disorders is similar in vaccinated and non-vaccinated populations. Correlation never has and never will prove causation.10,11,12
Since the HPV vaccination programme started in 2010 the Health Products Regulatory Authority in Ireland has received 1,082 reports of suspected adverse reactions/events associated with its use. It must be noted an adverse event is not a side-effect.13 These 1,082 adverse events were investigated and the majority of these reports have been consistent with the types of effects known to occur with the vaccine, as described in the product information.
The most common adverse events reported were considered mild. For serious adverse events reported, there has been no unusual pattern or clustering that would suggest that the events were caused by the HPV vaccine. The HPRA received 18 reports which included the term ‘chronic fatigue syndrome’, 10 reports included the term ‘post-viral fatigue’ and five reports included ‘autoimmune disorder’. It has been proven in multiple studies that these conditions are not associated with this vaccine. One large European study published in the BMJ found no evidence supporting associations between exposure to the HPV vaccine and autoimmune, neurological, and venous thromboembolic adverse events in almost one million adolescent girls.12
An international review of HPV vaccine safety in observational studies between 2006-2015 investigated serious adverse events, such as adverse pregnancy outcomes, autoimmune diseases, including Guillain-Barre syndrome, multiple sclerosis, anaphylaxis, venous thromboembolism and stroke. No increase in the incidence of these events was found compared with background rates.3
The WHO has noted previously that policy decisions based on weak evidence leading to lack of use of safe and effective vaccines can result in real harm with women and men being left vulnerable to HPV driven cancers.8 Continued pharmacovigilance is essential. Adverse events reported to the HSE need to be thoroughly investigated to maintain the public’s confidence in this vaccine. Patients and families deserve that at the very least.
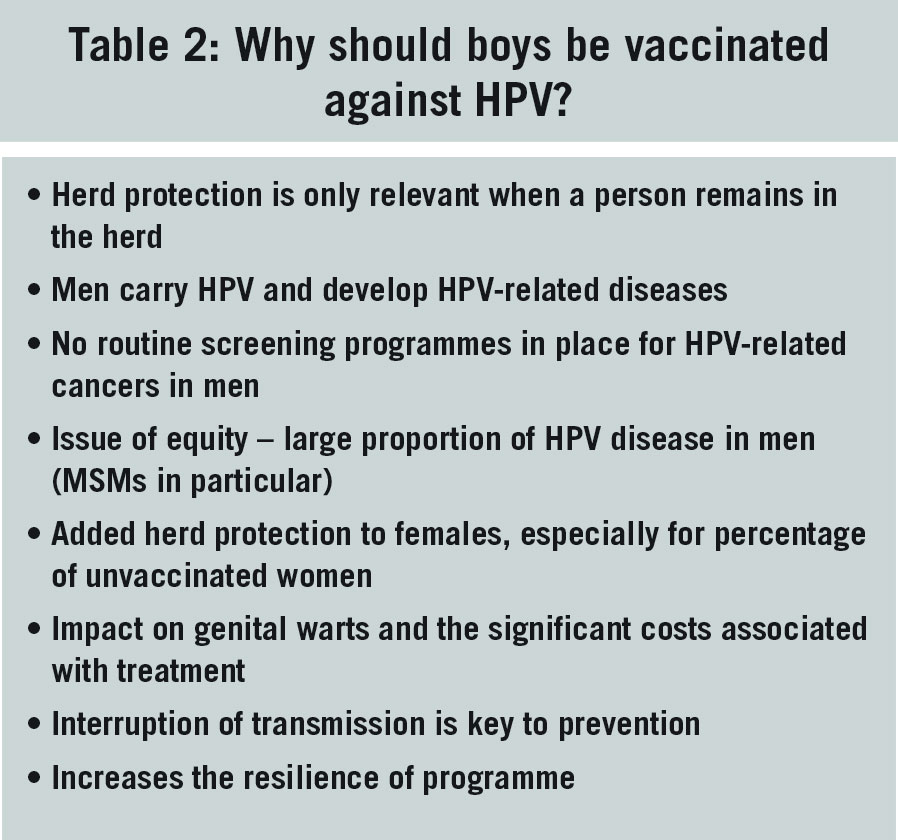
The HSE has established an excellent vaccination programme for young girls. Gender-neutral vaccination (girls and boys) is now required immediately so that the full benefits of the vaccination programme can be realised. With demonstrated efficacy, cost-effectiveness, and safety, universal HPV vaccination of all young, adolescent girls and boys should be a national health priority (see Table 2).
(click to enlarge)
Conclusion
To date, some 220,000 Irish girls have safely received the HPV vaccine. All girls less than 15 years of age at the first dose require two doses of the HPV vaccine given at least six months apart.
All girls aged 15 years and older at the first dose require three doses of the HPV vaccine – the first two doses given at least six months apart and the third dose given at least three months after the second dose. From October 2016, the HPV vaccine is available through HIV clinics to HIV-positive men and women under 26 years of age and from January 2017, the HPV vaccine is available through STI services to MSM aged under 26 years of age.
HPV vaccination rates in 2014-15 were 89.6%. This fell in dramatic fashion to an estimated 50% in 2016-17.14 There has been a grave injustice to those children who have missed out on this vaccine and where at all possible catch-up schedules should be used to protect them.
The 2018 Cochrane review Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors concludes: “There is high-certainty evidence that HPV vaccines protect against cervical pre-cancer in adolescent girls and women who are vaccinated between 15 and 26 years of age.”15
Anecdotal misinformation can have significant negative consequences and the statistical reality of evidence-based medicine is that some of the children not receiving this vaccine will die of preventable HPV diseases. Vaccination levels for this year are estimated to be 61.7% and this recovery in vaccine numbers is attributed to the excellent work of the Irish National Immunisation Office. This is still far below where we need to be. The GP is at the frontline and has an essential role in promoting the positive impact this vaccine is having worldwide. We must protect our children and vaccinate our boys and girls.
References
Garland S, Kjaer S, Munoz N, et al. A Systematic Review of 10 Years of Real-world Experience. Clinical Infectious Diseases, 2016; 63(4): 519–527,https://doi.org/10.1093/cid/ciw354
Naud PS, Roteli-Martins C, De Carvalho N, et al. Sustained efficacy, immunogenicity, and safety of the HPV-16/18 AS04-adjuvanted vaccine. Final analysis of a long-term follow-up study up to 9.4 years post-vaccination. Hum Vaccin Immunother. 2014; 10(8): 2147–2162. Published online 2014 Jun 19. doi: 10.4161/hv.29532
Vichnin M, Bonanni P, Klein NP, et al. An Overview of Quadrivalent Human Papillomavirus Vaccine Safety: 2006 to 2015. Pediatr Infect Dis J. 2015 Sep;34(9):983-91. doi: 10.1097/INF.0000000000000793
de Martel C, Plummer M, Vignat J, Franceschi S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int J Cancer 2017; 141(4): 664-670 doi: 10.1002/ijc.30716. Epub 2017 Jun 8.
Latest figures on HPV-caused cancers highlight urgent need for increased investment to prevent unnecessary deaths. Irish Cancer Society, https://www.cancer.ie/about-us/news/latest-figures-hpv-caused-cancers-highlight-urgent-need-increased-investment-prevent#sthash.dS4ucSuD.dpbs
Lee L, Garladn S. Human papilomavirs vaccination: the population impact. Published online 2017 Jun 12. doi: 10.12688/f1000research.10691.1
World Health Organisation: Immunisation, Vaccines and Biologicals: Human Papillomavirus (HPV). http://www.who.int/immunization/diseases/hpv/en/
WHO Global Vaccines Safety. Safety update on HPV vaccines 2017. http://www.who.int/vaccine_safety/committee/topics/hpv/June_2017/en/
Feiring B, Laake I, Bakken IJ, et al. HPV vaccination and risk of chronic fatigue syndrome/myalgic encephalomyelitis: A nationwide register-based study from Norway. Vaccine 2017; 35(33): 4203-4212
European Medicines Agency. HPV vaccines: EMA confirms evidence does not support that they cause CRPS or POTS. November 2015, accessible on: http://www.ema.europa.eu/docs/en_GB/document_library/Press_release/2015/11/WC500196352.pdf
Arnheim-Dahsltrom L, Pasternak B, Svanstrom H, Sparen P, Hviid A. Autoimmune, neurological, and venous thromboembolic adverse events after immunisation of adolescent girls with quadrivalent human papillomavirus vaccine in Denmark and Sweden: cohort study. BMJ 2013; 347 doi: https://doi.org/10.1136/bmj.f5906
HPSC HPV Immunisation Uptake Statistics. Accessible on http://www.hpsc.ie/a-z/vaccinepreventable/vaccination/immunisationuptakestatistics/hpvimmunisationuptakestatistics/
Arbyn M, Xu L, Simoens C, Martin-Hirsch P. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. The Cochrane Library. DOI: 10.1002/14651858.CD009069.pub3
 (click to enlarge)
(click to enlarge)