The ASCO practice guidelines regarding thrombosis and malignancy have recently been updated to incorporate new research
Dr Derek Power, Consultant in Medical Oncology, Cork University Hospital, Cork and Dr Aine O'Reilly, Medical Oncology Registrar, Department of Medical Oncology, Mercy University Hospital, Cork
The effects of malignancy on the haemostatic state are far-reaching and can range from haemorrhage to thrombosis. Armand Trousseau first described the association between thrombosis and cancer over 150 years ago. He recognised that a local malignancy could produce thromboembolic effects in distant sites and that local inflammatory or mechanical processes couldn’t explain this phenomenon. That simple observation was the first attempt to characterise the relationship between malignancy and thrombosis.
The molecular mechanisms by which tumour cells, mediators of the microenvironment and oncogenes impact on the homeostatic process and promote a hypercoagulable state are complex. Recent data has focused on the activation of the prothrombotic mechanism by tumour cells as a means of neovascularisation and metastases formation. Platelet-derived growth factor (PDGF) and tumour-derived micro particles are major areas of interest.1
Epidemiology
Venous thromboembolic events (VTE) are common among patients with cancer and result in significant morbidity and mortality. Data suggests that oncology patients have between a four-fold and seven-fold increased risk of VTE compared to the general population. Varying patient-related, cancer-related and treatment-related factors contribute to variability in published rates of VTE. In a recent retrospective analysis of 17,284 ambulatory patients undergoing chemotherapy in the US for a range of malignancies, Khorana and colleagues reported a VTE rate of 12.6%.
The authors noted that the higher VTE rate in this study, as compared to previous studies, may be explained by the unselected nature of this cohort compared to the highly selected patients enrolled in clinical trials.2
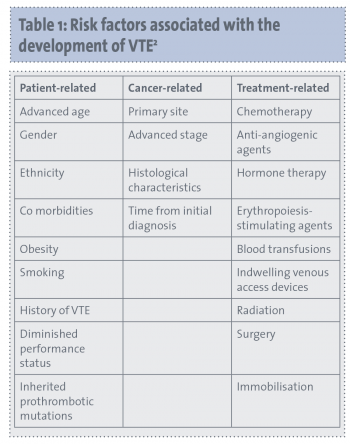
Recognised risk factors associated with the development of VTE are presented in Table 1. In the population studied by Khorana et al, pancreatic cancer and gastric cancer were associated with high rates of VTE, 19.2% and 15.8%, respectively. Patients were more likely to develop VTE early in their treatment, with 18.1% of events occurring within one month of initiation of treatment. Chemotherapeutic agents that were platinum-based, had erythropoiesis-stimulating properties or that were anti-angiogenic were associated with a higher risk of VTE.
(click to enlarge)
Treatment
The recommended treatment for VTE in oncology patients is low-molecular-weight heparin (LMWH), both for the initial 5-10 days of treatment and for six months following diagnosis. Anticoagulation beyond this may be warranted in the setting of metastatic disease or with high-risk chemotherapeutic regimens but these decisions are largely patient specific.3 LMWH has been shown to be more effective in treatment of VTE than unfractionated heparin. Unfractionated heparin is generally reserved for patients with renal impairment.4,5
Vitamin K antagonists, historically, are impractical for use in oncology patients given the high rates of vomiting and the potential for drug-drug interactions that can require frequent monitoring of the international normalised ratio (INR). Newer anticoagulants are currently being investigated for treatment and prophylaxis of VTE. Such agents include both parenteral and oral factor Xa inhibitors (direct and indirect) and novel direct oral thrombin inhibitors.6 Overall, the data regarding new anticoagulants in oncology patients is limited and requires further investigation and validation.
Incidental VTE
Staging radiological investigations frequently diagnose incidental, largely asymptomatic VTE in oncology patients. A prevalence of incidental pulmonary embolism (PE) as high as 3% has been reported and various publications have retrospectively noted that incidental PEs account for 35-44% of diagnosed PEs.3,7-9
It is currently recommended that incidental VTE be treated in the same manner as symptomatic VTE.
Prophylaxis of oncology patients
The American Society of Clinical Oncology (ASCO) recently published updated recommendations regarding prophylactic anticoagulation in oncology patients (see Table 2).3
(click to enlarge)
In medically unwell inpatients with active malignancy and other risk factors for VTE, in the absence of bleeding risks or contraindication, ASCO recommends the use of prophylactic anticoagulation. This recommendation is based on observed results from three randomised control trials of general medical inpatients which allowed for enrolment of oncology patients.
Two of the studies – CERTIFY (Certoparin for thromboprophylaxis in medical patients) and CERTAIN (Certoparin versus unfractionated heparin for the prevention of thromboembolic complications in acutely ill medical patients) – compared rates of VTE in patients randomised to receive a low-molecular-weight heparin (LMWH) or unfractionated heparin.10,11 EXCLAIM (Extended prophylaxis for venous thromboembolism in acutely ill medical patients with prolonged immobilization) examined the use of extended prophylaxis with enoxaparin.12 Cancer-specific results were not reported in any of these trials and, to date, no randomised control trial has evaluated the role of prophylactic anticoagulation in ambulatory or hospitalised oncology patients.
ASCO recommends that patients with active malignancy in the perioperative setting should undergo prophylactic anticoagulation in the absence of bleeding risk or contraindication. In patients with high-risk features undergoing abdominal or pelvic surgery, prophylaxis should be continued for up to four weeks post operatively.
The use of anticoagulation in ambulatory oncology patients is controversial. Two randomised control trials have examined prophylactic anticoagulation in a heterogeneous group of oncology patients. Anticoagulation with nadroparin, a LMWH, was investigated in PROTECHT (Prophylaxis of thromboembolism during chemotherapy trial), a double-blind, randomised controlled trial (RCT) where 1,150 patients with lung, gastrointestinal, pancreatic, breast, ovarian, or head and neck cancers were randomised to receive daily nadroparin or placebo. Within the treatment group and placebo group, the rate of VTE was 2% and 3.9%, respectively (p = 0.02).13
Anticoagulation with semuloparin, an ultra-LMWH, was investigated in the recent SAVE-ONCO trial, a double-blind RCT, where 3,212 patients with lung, pancreatic, gastric, colorectal, bladder or ovarian cancer were randomised to receive semuloparin or placebo.14 Within the treatment group and placebo group, the rate of VTE was 1.2% and 3.4%, respectively, representing a relative risk reduction of 64%.14
Given the low event rates in these studies, the ASCO guidelines currently do not recommend routine prophylactic anticoagulation of ambulatory oncology patients. A number of studies have evaluated the use of routine prophylactic anticoagulation in oncology patients with specific pathologies. Though higher event rates have been reported in homogeneous populations, such as pancreatic cancer, the current ASCO recommendation is that decisions regarding prophylactic anticoagulation in high-risk malignancies be made on a case-by-case basis.
Risk assessment
Identifying patients who are at a high risk of developing VTE, and would thus benefit from prophylactic anticoagulation, is a topic of much interest. The ASCO 2013 practice guideline update regarding thrombosis recommends that all patients should undergo a risk assessment for thrombosis prior to initiation of treatment.
The Khorana model is often reported in assessing thrombosis. This model has also been validated in many series.15 It takes into account five easily available clinical and laboratory parameters for prediction of VTE (see Table 3). These five variables were initially derived from a prospective, observational study of 2,701 patients undergoing treatment for a range of malignancies (breast, lung and colorectal primaries accounted for over 60% of patients). Patients were stratified into high-risk, intermediate-risk and low-risk groups based on these variables, with reported VTE rates of 7.1%, 1.8% and 0.8%, respectively. This model was then validated in a cohort of 1,365 similar patients with reported VTE rates of 0.3% in the low-risk group, 2% in the intermediate group and 6.7% in the high-risk group.
(click to enlarge)
The Vienna Cancer and Thrombosis Study (Vienna-CATS), a prospective and observational cohort study, validated the Khorana risk score in a cohort of 819 patients with a range of malignancies (breast, lung and colorectal primaries accounted for 45% of primaries).16 Using the original stratification, 17.7% of patients in the high-risk group (score > 3) developed VTE, and 1.5% of patients in the low-risk group (score 0) developed VTE. The authors sub-classified the intermediate group into patients with a score of 1 or 2, with VTE rates of 3.8% and 9.6%, respectively.
The Khorana index was applied to the patients of the SAVE-ONCO and showed greater risk reduction in the high-risk group (5.4% VTE rate in semuloparin treated patients, 1.5% VTE rate in the placebo group) than in the low-risk group (1% VTE rate in semuloparin treated patients, 1.3% VTE rate in the placebo group). The Khorana index has since been further validated and its predictive value in specific cancer types is being examined.
A number of studies have attempted to improve upon the predictive value of the Khorana score by taking into account biomarkers associated with VTE risk. The Vienna-CATS study modified the original Khorana score to include measurements of d-dimer and soluble P-selectin. In the newly defined high-risk group (score ≥ 5) 35% of patients developed VTE while only 1% of those in the low-risk group (score 0) developed VTE. Tissue factor and tissue factor expression as micro particles has not been shown to be a predictor of thrombosis.17 A host of other biomarkers are currently being investigated for their predictive value. These studies require further validation before general use.
Conclusion
VTE is common in patients with cancer and impacts significantly on treatment, morbidity and mortality. The ASCO practice guidelines regarding thrombosis and malignancy have recently been updated to incorporate new research in the areas of novel anticoagulants, prophylactic anticoagulation and risk stratification for VTE. Current guidelines recommend the use of LMWH in treatment of VTE and favour prophylactic anticoagulation in medically unwell inpatients with other risk factors for VTE, and in the perioperative setting. Though decisions regarding prophylactic anticoagulation of ambulatory oncology patients are still on an individual basis, ASCO recommends using validated risk-assessment models such as the Khorana index to aid in the decision- making process.
Future studies should focus on further investigation of novel anticoagulants in the cancer-specific population and validation of novel biomarkers in VTE prediction
References
Beleva E, Grudeva-Popova J. From Virchow’s triad to metastasis: Circulating hemostatic factors as predictors of risk for metastasis in solid tumors. J BUON 2013; 18: 25-33.
Khorana AA, Dalal M, Lin J, et al. Incidence and predictors of venous thromboembolism (VTE) among ambulatory high-risk cancer patients undergoing chemotherapy in the United States. Cancer 2013; 119: 648-655.
Lyman GH, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2013; 31: 2189-2204.
Akl EA, Labedi N, Barba M, et al. Anticoagulation for the long-term treatment of venous thromboembolism in patients with cancer. Cochrane Database Syst Rev: CD006650; 2011.
Leizorovicz A, Siguret V, Mottier D, et al. Safety profile of tinzaparin versus subcutaneous unfractionated heparin in elderly patients with impaired renal function treated for acute deep vein thrombosis: The Innohep(R) in Renal Insufficiency Study (IRIS). Thromb Res 2011; 128: 27-34.
Prandoni P, Dalla Valle F, Piovella C, et al. New anticoagulants for the treatment of venous thromboembolism. Minerva Med 2013; 104: 131-139.
Dentali F, Ageno W, Becattini C, et al. Prevalence and clinical history of incidental, asymptomatic pulmonary embolism: A meta-analysis. Thromb Res 2010; 125: 518-522.
Lyman GH, Kuderer NM, American Society of Clinical Oncology. Prevention and treatment of venous thromboembolism among patients with cancer: The American Society of Clinical Oncology Guidelines. Thromb Res 2010; 125 Suppl 2: S120-127.
O’Connell CL, Boswell WD, Duddalwar V, et al. Unsuspected pulmonary emboli in cancer patients: Clinical correlates and relevance. J Clin Oncol 2006; 24: 4928-4932.
Riess H, Haas S, Tebbe U, et al. A randomized, double-blind study of certoparin versus unfractionated heparin to prevent venous thromboembolic events in acutely ill, non-surgical patients: CERTIFY Study. J Thromb Haemost 2010; 8: 1209-1215.
Schellong SM, Haas S, Greinacher A, et al. An open-label comparison of the efficacy and safety of certoparin versus unfractionated heparin for the prevention of thromboembolic complications in acutely ill medical patients: CERTAIN. Expert Opin Pharmacother 2010; 11: 2953-2961.
Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: A randomized trial. Ann Intern Med 2010; 153: 8-18.
Agnelli G, Gussoni G, Bianchini C, et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: A randomised, placebo-controlled, double-blind study. Lancet Oncol 2009; 10: 943-949.
Agnelli G, George DJ, Kakkar AK, et al. Semuloparin for thromboprophylaxis in patients receiving chemotherapy for cancer. NEJM 2012; 366: 601-609.
Khorana AA, Kuderer NM, Culakova E, et al. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008; 111: 4902-4907.
Ay C, Dunkler D, Simanek R, et al. Prediction of venous thromboembolism in patients with cancer by measuring thrombin generation: Results from the Vienna Cancer and Thrombosis Study. J Clin Oncol 2011; 29: 2099-2103.
Hernandez C, Orbe J, Roncal C, et al. Tissue factor expressed by microparticles is associated with mortality but not with thrombosis in cancer patients. Thromb Haemost 2013; 110(3). [Epub ahead of print]
 (click to enlarge)
(click to enlarge)

