A six-month audit of patient follow-up after commencement of prophylaxis post blood-borne virus exposure was completed
Dr Jack Lambert, Consultant in Infectious Diseases and Genitourinary Medicine, Mater Misericordiae University Hospital, Dublin, Dr Emma Pringle, Third-Year GP Trainee, North Dublin City GP Training Scheme, Dublin, Ms Rachel Howard, Clinical Nurse Specialist (Infectious Diseases), Mater Misercordiae University Hospital, Dublin and Dr Tomas Breslin, Emergency Medicine Consultant, Mater Misercordiae University Hospital, Dublin
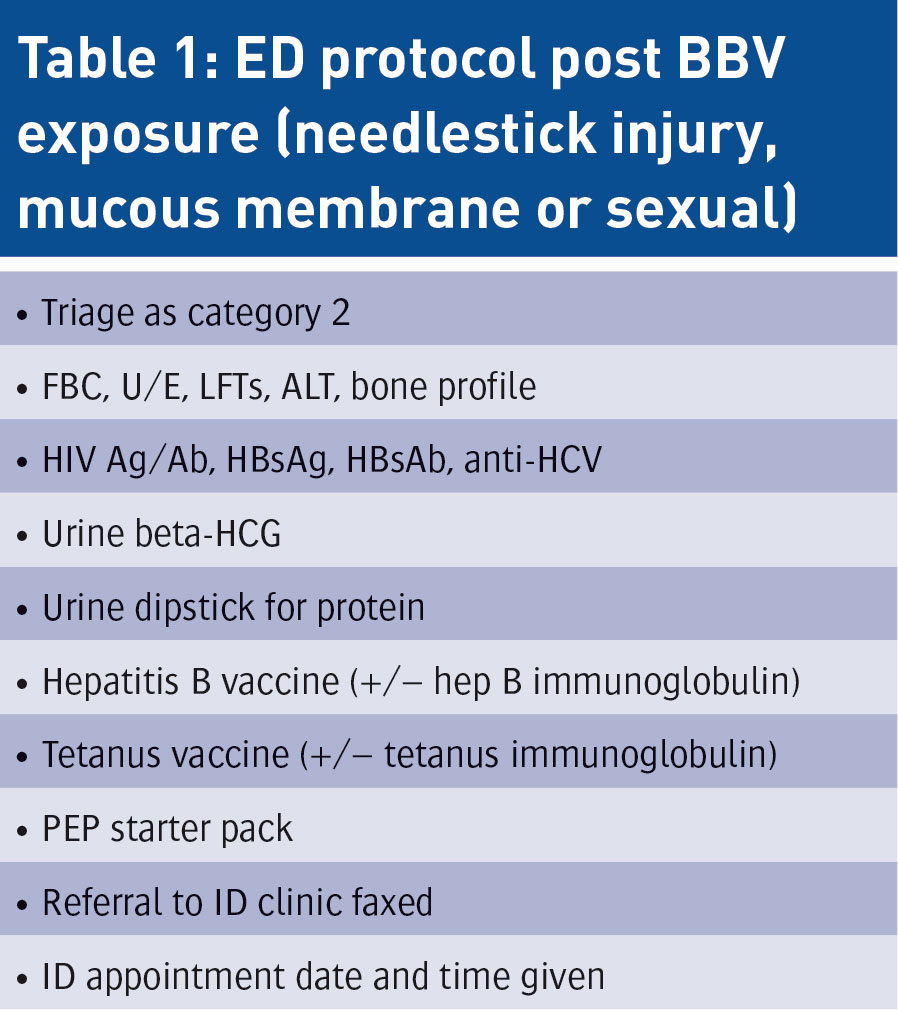
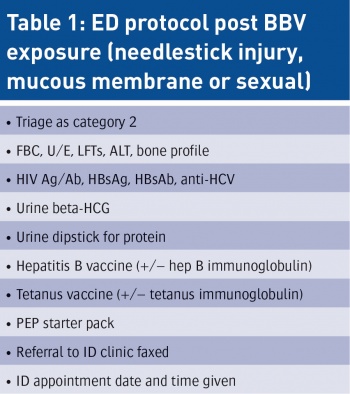
Patients who present with a needlestick injury (NSI), mucous membrane exposure or sexual exposure to possible blood-borne viruses (BBV) are managed as per protocol in the emergency department (ED). This protocol has been developed as per the HSE EMI Toolkit ‘Guidelines for the emergency management of injuries’.1 Patients should be triaged as category 2 in the ED to ensure that they are seen urgently and commenced on post-exposure prophylaxis (PEP) as soon as possible after exposure (must be within 72 hours).
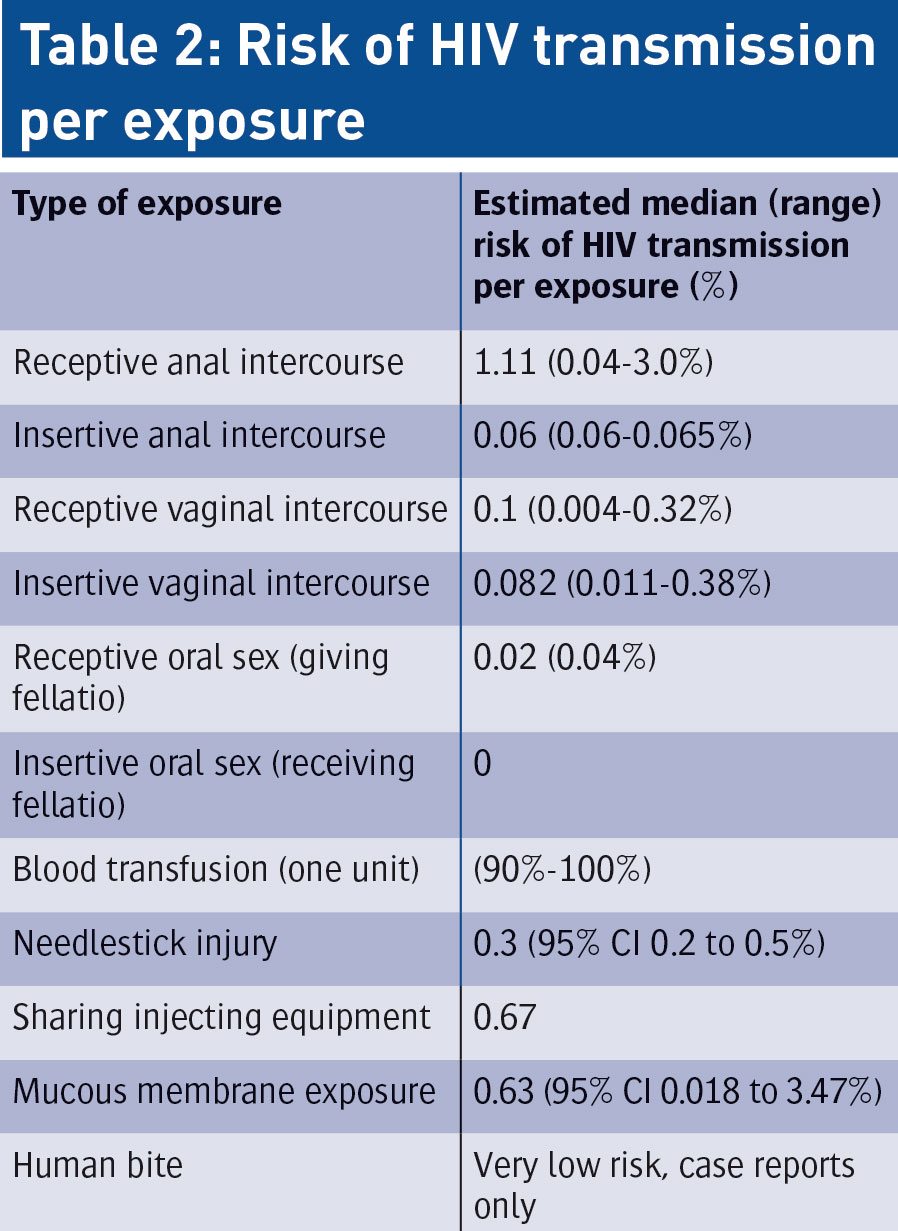
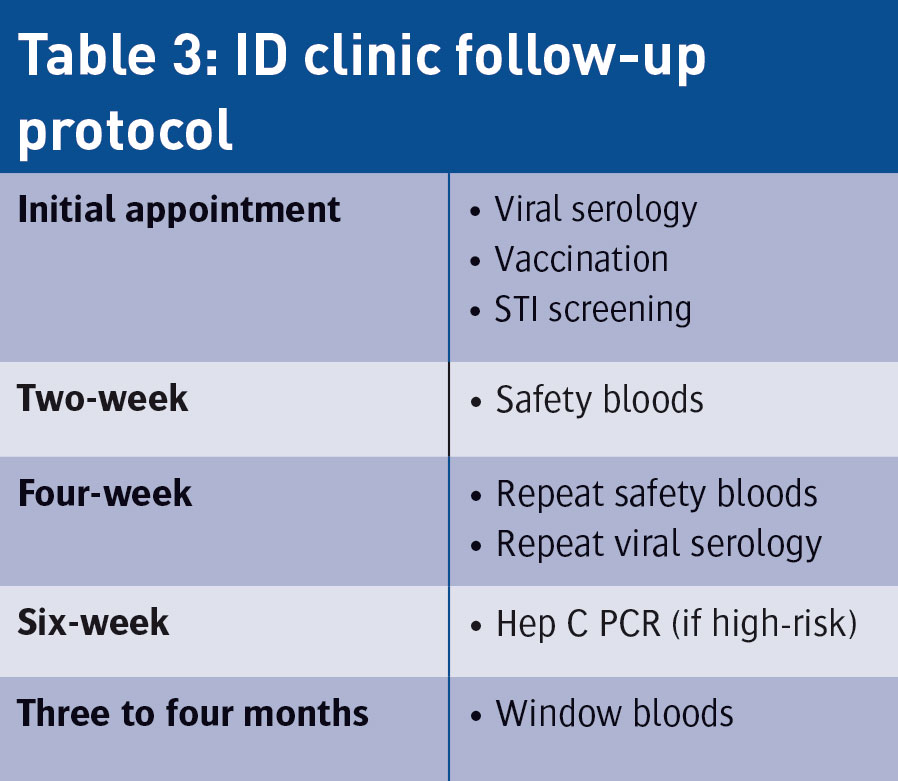
Evidence has shown that the sooner PEP is commenced, the more effective it will be in preventing BBV transmission.2 A hepatitis B vaccination is given as well as tetanus vaccination in the case of needlestick injuries and human bites. Patients are commenced on a five-day PEP starter pack. They are informed of the utmost importance of attending infectious diseases (ID) follow-up for counselling regarding serology results and estimation of the risk2 of transmission of BBV for their exposure. At an ID appointment, a decision to continue PEP for a further 23 days (to complete 28 days in total) or stop treatment is made depending on estimation of risk for exposure.2
Introduction
We were concerned that there was a high rate of non-attendance and loss of patients to follow-up in our institution. An audit was conducted of patients who did not attend for appointments after being commenced on PEP. The aim was to determine the exact number of patients that did not complete follow-up, consider possible explanations for this and to discuss ways of improving the attendance rate.
Method
This was a six-month retrospective audit of all patients commenced on PEP for BBV exposure in ED. Patients were identified from filed PEP starter pack prescriptions from January 1 to July 1, 2014 which were available from the hospital pharmacy. Patient ED records, electronic records (patient centre) and laboratory results were reviewed. An Excel sheet was created noting 10 categories: age, gender, triage category on ED card, type of BBV exposure, hepatitis B vaccination, tetanus immunisation, referral to ID clinic, attendance at initial ID appointment, attendance at four-week follow-up and attendance for window bloods. Patients were contacted by telephone using the numbers provided at initial ED registration.
(click to enlarge)
(click to enlarge)
Results
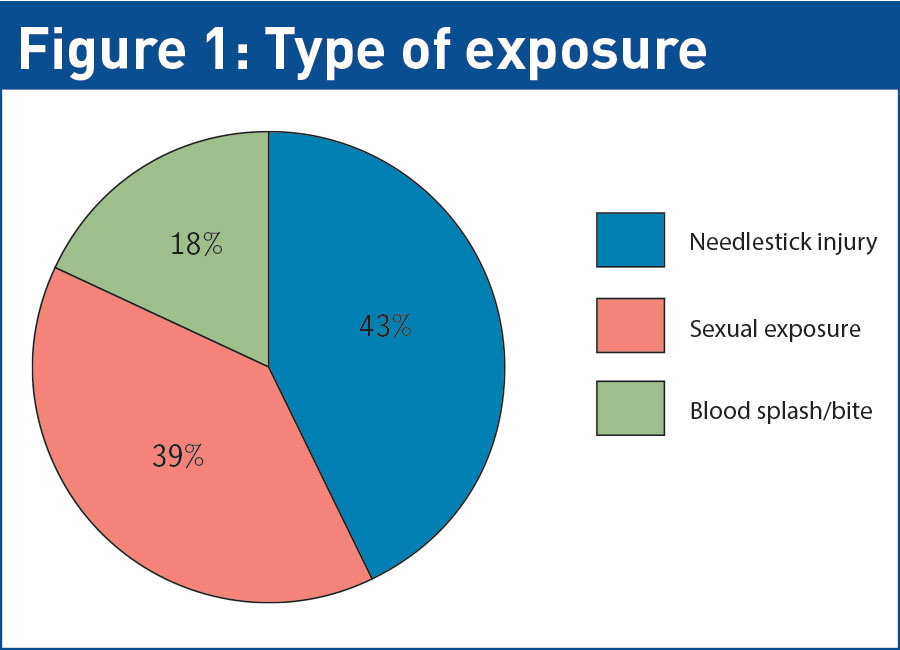
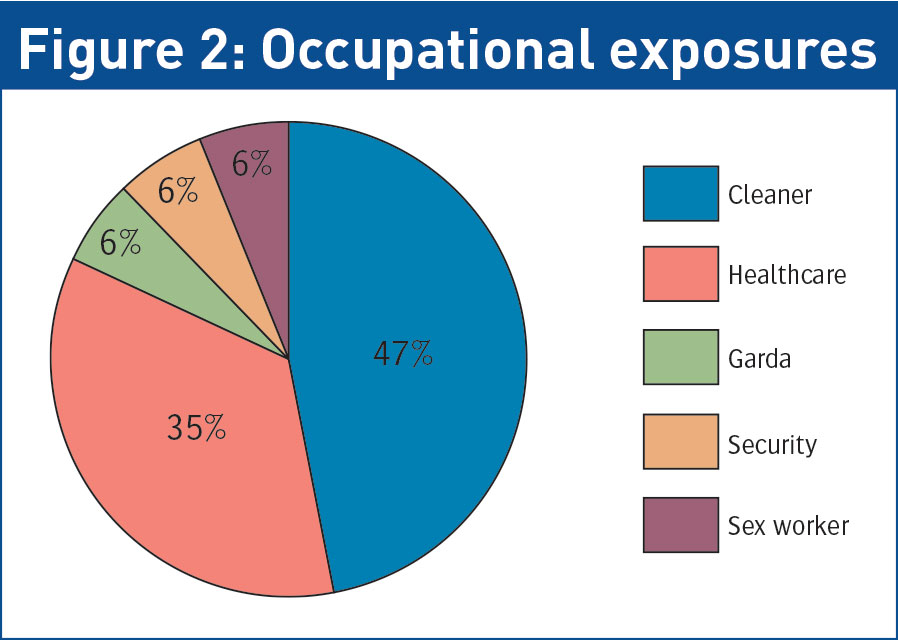
Fifty-four patients were commenced on five-day PEP starter packs between January 1 and July 1 2014. Of these, 70% were male, representing two-thirds of the cohort (n = 38). The mean age was 32 years, with the range being from 20 to 61 years. In total, 24 patients had obtained NSI; 21 presented post-sexual exposure and nine were commenced on PEP post-mucous membrane exposure, either from human bite or blood splash injuries. It is important to emphasise that almost all human bites do not require any follow up for HIV or hepatitis C.3 Included in our audit were extreme cases which are the exception to the rule. It was noted that 17 patients had been exposed to BBVs during occupational incidents: eight cleaners, six healthcare workers, one security guard, one member of An Garda Siochana and one sex worker.
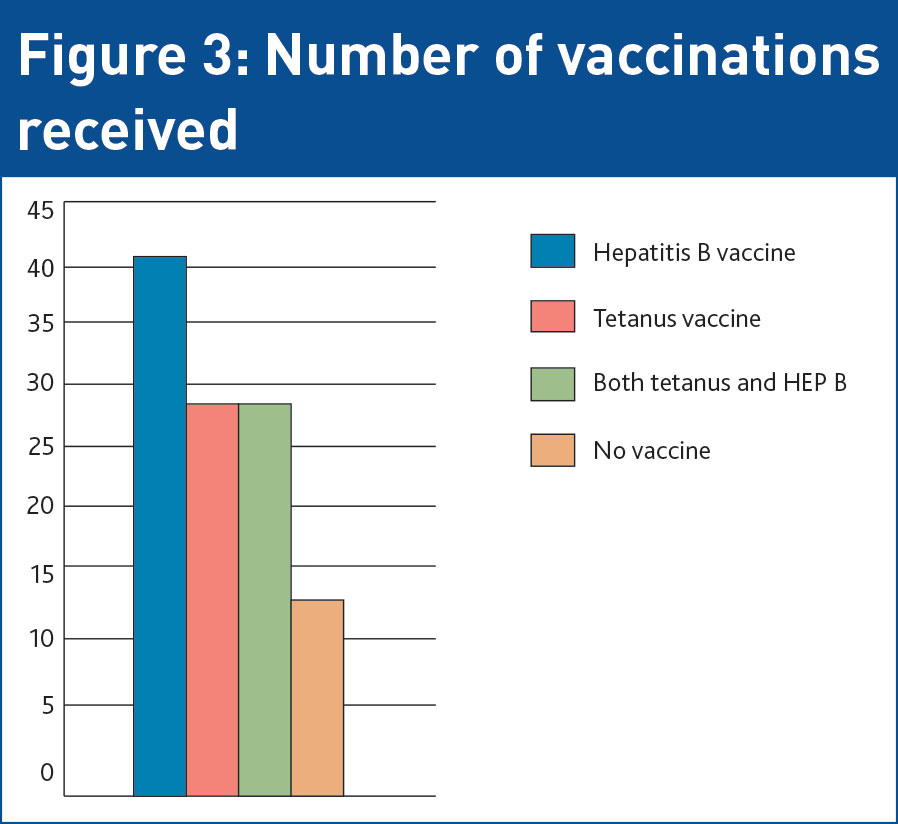
At presentation, 48 patients were triaged as category 2 (89%), three as category 3 and three as category 4. In total, 42 patients (78%) received hepatitis B vaccination. Of the 12 patients who did not, three were healthcare workers who would have completed hepatitis B vaccination prior to commencing their post. Overall, five others received hepatitis B immunisation in the past. This meant four patients who presented and had not been vaccinated previously did not receive hepatitis B injection.
A total of 31 patients received tetanus immunisation. Of the 23 patients who did not, four had been vaccinated previously, however, there was no documentation in each case of whether this had been in the previous 10 years.4 Of the 19 patients who did not receive tetanus vaccine, and where there was no documentation regarding prior immunisation, six had presented with NSIs and one with a human bite. All four other patients who had sustained human bites received tetanus vaccines. In total, 16 patients presenting with needlestick injuries received tetanus (67% of NSIs).
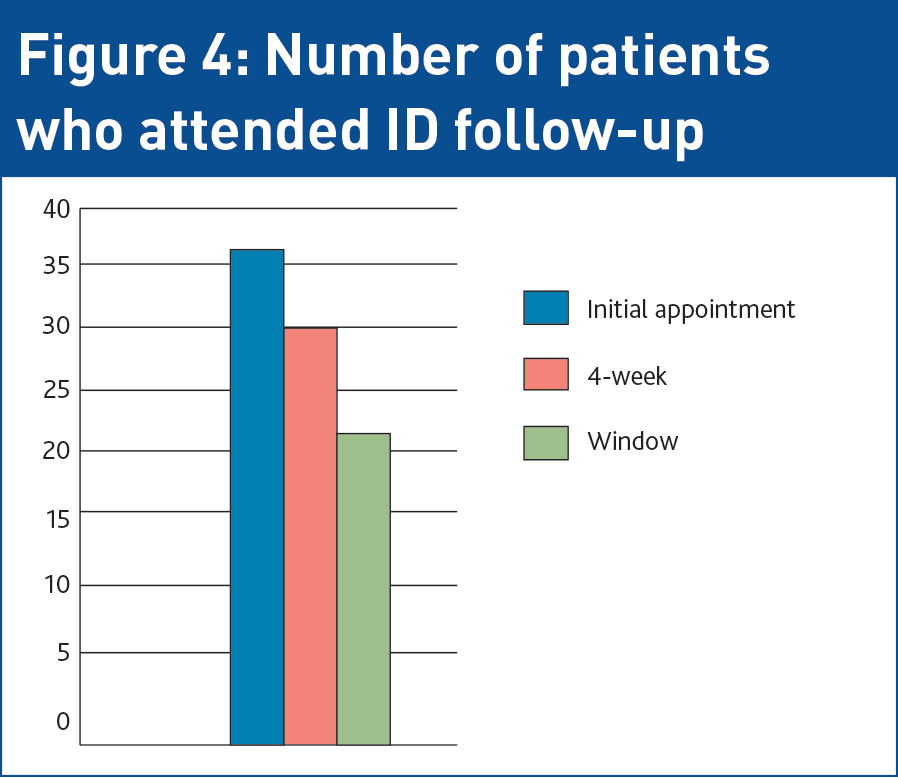
Of the 54 patients commenced on PEP starter packs in ED post-BBV exposure, 52 were referred for ID outpatient follow-up. There were two healthcare workers who were referred to occupational health. Of the 52 patients referred to ID clinic, 38 attended their initial follow-up appointment, 31 attended at one-month and 23 attended all ID appointments, completing window blood follow-up. This meant 14 patients did not receive any follow-up. There was one patient who was newly diagnosed on initial HIV serology testing at zero months. He was found to be both antigen and antibody positive, indicating transmission resulted from a previous exposure. No other episodes of seroconversion were noted, either for HIV or hepatitis C. There were two incidental findings of syphilis, which were subsequently treated and followed up in the STI clinic. Both of these were in the men who have sex with men category.
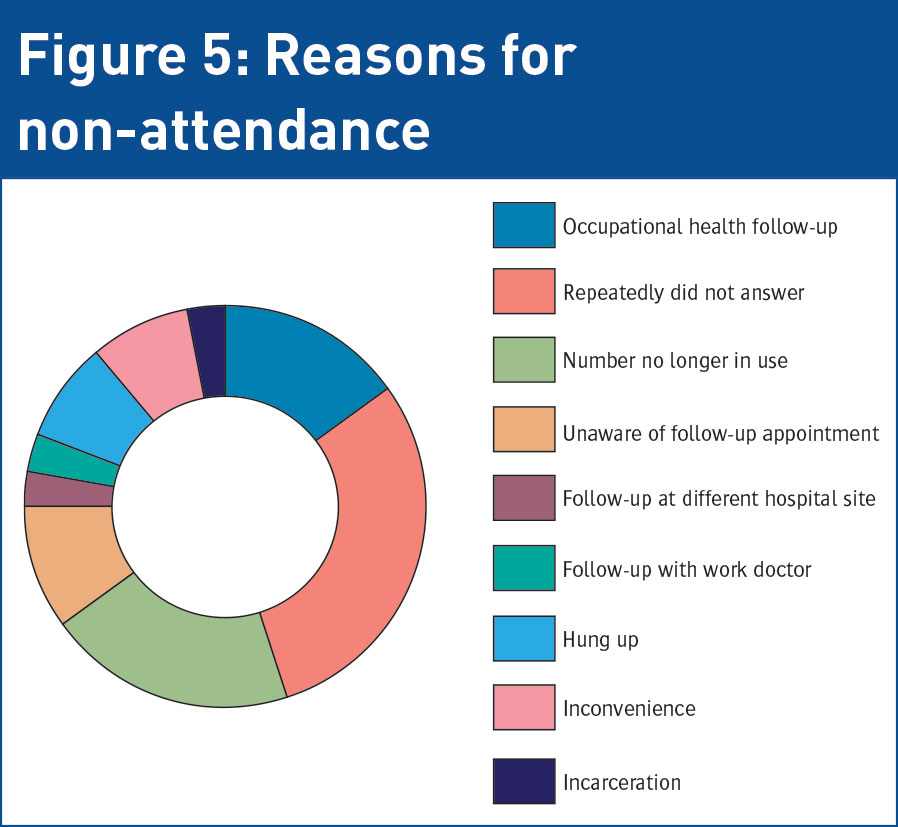
Overall, 14 patients did not attend any follow-up appointments. A further 14 attended at least once but did not complete their follow-up. These patients were contacted by telephone to establish the reason for non-attendance and to determine ways in which attendance rates could be improved. Of these 14 patients, four were healthcare workers who arranged follow-up with occupational health. Three patients said they were not informed about a follow-up appointment and one who was advised to have repeat viral serology with their general practitioner in six months time. An ID referral form was completed for this patient on electronic patient records. There was one patient whose care was transferred to and completed at a different, more convenient hospital site, one patient attended with their work doctor and nine repeatedly did not answer; five telephone numbers were no longer in use, two patients hung up when the reason for contact was disclosed, two patients discussed how they had been too busy to attend and found it difficult to arrange travel to the clinic, and one patient had since been incarcerated. Follow-up and window bloods have since been arranged for two of these patients who agreed to attend.
(click to enlarge)
(click to enlarge)
(click to enlarge)
(click to enlarge)
Discussion
Almost one-third of possible exposures to blood-borne viruses occurred during occupational incidents, most of these outside of the healthcare setting. Further training regarding health and safety, needlestick injury prevention and use of personal protective equipment may be beneficial, particularly for cleaners and council workers.
Another concern was that more than half of patients presenting post-NSI did not receive tetanus or hepatitis B vaccination. Re-evaluation of the ID referral form revealed documents involving many unnecessary instructions and information requirements. Emergency medicine physicians are under immense pressure to see as many patients as possible in a shift. If protocols are too detailed and time-consuming, it may result in doctors abandoning the protocol and adopting a sub-therapeutic approach, which was witnessed in a number of cases. This audit highlighted that a revised protocol and referral process must be developed in order to assist ED personnel in the management of patients requiring PEP. This is currently underway.
A significant number of patients were commenced on PEP post-sexual exposure. The current ‘Think Contraception’ campaign raises awareness regarding the need for condoms or oral contraceptive pills to prevent unwanted pregnancy but perhaps more attention should be focused on using barrier protection to avoid sexually transmitted disease and virus transmission.
Regarding ID clinic follow-up, the attendance rate was worryingly low at only 49%, with 14 patients receiving no follow-up at all. The fact that three patients were reportedly not informed about clinic follow-up again emphasises the need for a more transparent management plan, with the priority being clinic follow-up as soon as possible. This will enable the ID team to administer vaccinations if not done so in the ED.
Overall, four patients did not attend appointments for convenience reasons. A possible avenue to address this could be to liaise with patients’ GPs from the outset. After an initial ID clinic review, where risk estimation, counselling regarding possible positive results and a decision whether or not to continue PEP is made, care could be transferred back to the community for safety and window bloods. It is recognised that patients often would prefer if their GP was not aware that they had been treated with PEP, particularly in the case of sexual exposure. A possible route to overcome this could be to create a discharge document, with the indication for PEP not disclosed, indicating that the patient requires safety and window bloods. This would have the added benefit of reducing both ID clinic numbers and waiting lists, while returning the gate-keeper role to the GP and allowing continuity of care.
This audit highlighted that despite modern computerised hospital systems and protocols, patients are still being lost to essential follow-up in our healthcare system. We need to continue to strive towards improved communication between secondary and primary care in order to optimise the management of our patients.
 (click to enlarge)
(click to enlarge)