Hypertension is a leading risk factor for cardiovascular mortality and may be a complex diagnosis
Dr AnneMarie O'Flynn, Cardiology Specialist Registrar, Department of Epidemiology and Public Health, University College Cork and Dr Patricia Kearney, Senior Lecturer, Department of Epidemiology and Public Health, University College Cork
The World Health Organization estimates that raised blood pressure causes 51% of stroke deaths and 45% of coronary heart disease deaths worldwide.1 However, many people still remain undiagnosed and of those who are diagnosed many are poorly controlled. Traditionally, blood pressure is measured in the clinical setting by a trained professional and a diagnosis of hypertension is made based on this. However, the diagnostic landscape is changing and is certainly becoming increasingly complex.
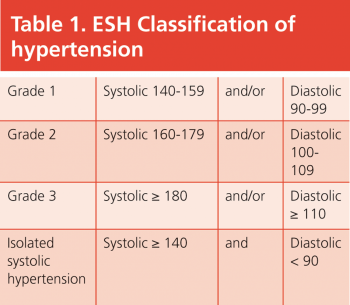
The 2007 European Society of Hypertension (ESH) guidelines2 define hypertension as an office or clinic blood pressure of greater than or equal to 140/90 and classify it as seen in Table 1.
(click to enlarge)
So what then of this changing landscape?
Firstly, there is home blood pressure monitoring (HBPM). There are now many devices available for patients to buy, including finger, wrist and arm devices.
It has been recommended, however, that only those that measure blood pressure at the upper arm be used as they have been shown to be the most reliable in clinical practice and research.3
Device validation, cuff size and patient education are other important considerations. Patients should take measurements in a seated position after several minutes rest and should monitor their blood pressure for seven days with at least two morning and two evening measurements. The readings of the first day should be discarded and the average of the other readings should be taken to guide clinical decision-making.3 It is important to note that the threshold for diagnosis of hypertension based on HBPM is lower than that for office blood pressure. The recommended systolic threshold is 130-135 with a diastolic threshold of 85.
Let us now consider ambulatory blood pressure monitoring (ABPM). ABPM provides information on blood pressure over a 24 or 48-hour period and in particular gives important information on the night-time blood pressure. As for HBPM, the use of validated devices and appropriate cuff sizes is important.
Patients should be advised to carry out their normal activities while being monitored and, if possible, should keep a diary and document their activities, as well as the times they go to bed at and get up. This allows accurate distinction to be made between the daytime and night-time periods. The thresholds for diagnosis of hypertension using ABPM are also lower than those for office blood pressure and are outlined in Table 2.
(click to enlarge)
The 2007 European Society of Hypertension guidelines recommend ABPM be considered in the following situations:
Considerable variability of office blood pressure is found over the same or different visits
High office blood pressure is measured in those at otherwise low cardiovascular risk
Marked discrepancy between blood pressure values measured in the office and at home
Resistance to drug therapy is suspected
Hypotensive episodes are suspected, particularly in the elderly and diabetic patients
Office blood pressure is elevated in pregnant women and pre-eclampsia is suspected.
However, the National Institute for Health and Clinical Excellence (NICE) in the UK went beyond this in 2011 and recommended that if the clinic blood pressure is 140/90 or higher, ABPM should be offered to confirm the diagnosis of hypertension.4 They classified hypertension based on ABPM as follows:
Stage 1 – daytime average ≥ 135/85mmHg
Stage 2 – daytime average ≥ 150/95mmHg.
The guideline did not grade hypertension beyond stage 2 as they felt it would not have any impact on treatment stratification or clinical decision-making.
Hodgkinson et al published the results of a systematic review and meta-analysis on the relative effectiveness of clinic blood pressure measurements and HBPM compared to ABPM in the British Medical Journal in 2011.5 They concluded that treatment decisions based on clinic or home blood pressure alone might result in over-diagnosis of hypertension. However, they did stress that a cost-effectiveness analysis was essential at the time.
Lovibond et al subsequently published in the Lancet on the cost-effectiveness of options for the diagnosis of hypertension in primary care and concluded that ABPM would reduce misdiagnosis and save costs.6 To summarise, it was felt that the increased costs related to ambulatory monitoring are counterbalanced by cost savings from better targeted treatment.
As well as improving our diagnostic power ABPM provides information on night-time blood pressure and the patterns observed:
Nocturnal dipping – a fall of 10% or more in the night-time blood pressure
Non-dipping – a fall of less than 10% in the night-time blood pressure
Reverse dipping – a rise in the nocturnal blood pressure
Extreme dipping – a fall of greater than 20% in the night-time blood pressure
Nocturnal hypertension – a night-time blood pressure greater than or equal to 120/70.
The night-time blood pressure has been shown to have the greatest prognostic significance. If we rely on clinic or HBPM for diagnosis we will miss the important information which nocturnal readings give us. Chronotherapy involves the administration of anti-hypertensive drugs in the evening in order to lower the night-time blood pressure. It is too early to recommend such a strategy as yet but there are studies which suggest it may have a benefit.7,8
Of course the reason we wish to diagnose hypertension is so we may treat it and reduce the risk of a future cardiovascular event.
Therefore total cardiovascular risk should be estimated for all patients diagnosed with hypertension using one of the available risk assessment tools such as SCORE. For instance, it may be appropriate to use a non-pharmacological strategy as a first step in somebody with grade 1 hypertension at otherwise low cardiovascular risk, while somebody at high cardiovascular risk should be prioritised for anti-hypertensive therapy.
Another consideration is the assessment of subclinical target organ damage, as evidence of same will further guide treatment. The ESH and NICE both recommend that a formal assessment of cardiovascular risk as well as an examination for subclinical target organ damage be carried out. Causes of secondary hypertension must also be considered in particular cases.
“The great importance of arterial hypertension or the conditions associated with it, as a widespread and apparently increasing cause of disability and death, is a self-evident incentive to investigation. At the same time it must be recognised that our knowledge of the subject is in a very confused state, as respects its phases of aetiology, mechanism and treatment.” This quotation from the Journal of the American Medical Association in 19209 demonstrates how long physicians and scientists have been investigating and treating hypertension.
We have come a long way since then, but newer technology and greater knowledge have certainly brought with them increased complexity.
Mancia G, De Backer G, Dominiczak A et al. ESH-ESC Task Force on the Management of Arterial Hypertension. 2007 3. ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension. J Hypertens 2007; 25(9): 1751-1762
Parati G, Stergiou G, Asmar R et al. On behalf of the ESH Working Group on Blood Pressure Monitoring. European Society of Hypertension guidelines for blood pressure monitoring at home: a summary report of the Second International Consensus Conference on Home Blood Pressure Monitoring. Journal of Hypertension 2008; 26(8): 1505-1526
http://guidance.nice.org.uk/CG127
Hodgkinson J, Mant J, Martin U et al. Relative effectiveness of clinic and home blood pressure monitoring compared with ambulatory blood pressure monitoring in diagnosis of hypertension: systematic review. BMJ 2011; 342: d3621
Lovibond K, Jowett S, Barton P et al. Cost-effectiveness of options for the diagnosis of high blood pressure in primary care: a modelling study. The Lancet 2011; 378(9798): 1219-1230
Hermida RC, Ayala DE, Mojón A, Fernández JR. Bedtime dosing of antihypertensive medications reduces cardiovascular risk in CKD. J Am Soc Nephrol 2011; 22(12): 2313-2321
Zhao P, Xu P, Wan C, Wang Z. Evening versus morning dosing regimen drug therapy for hypertension. Cochrane Database Syst Rev 2011; 10: CD004184
Allen FM. Arterial Hypertension. JAMA 1920; 74(10): 652-655
 (click to enlarge)
(click to enlarge)
