Head and neck cancer is the sixth most common cancer, with about 640,000 new cases each year worldwide. This year, July 27 marked ‘World Head and Neck Cancer Day’. Ireland joined the international movement of 53 countries to increase awareness and promote education and training in the diagnosis, treatment, outcomes, and research of head and neck cancer. More than 54,000 new cases of head and neck cancer were projected in the US in 2014. In Ireland this figure is in excess of 600 new cases per year. If we include thyroid cancer this figure rises to over 800. Projected numbers of incident cases, based on population projections 2015 to 2040 from the National Cancer Registry, indicate female case numbers will increase by 46% to 128% and male cases by 66% to 108%.
The head and neck region is an anatomically diverse region of the body that is composed of soft tissue, bones, skin, and a variety of glands and organs. Cancers may develop in several areas of this region, including the larynx, mouth, throat, thyroid, salivary tissue (parotid gland), lymphatic tissue, nose and sinuses.
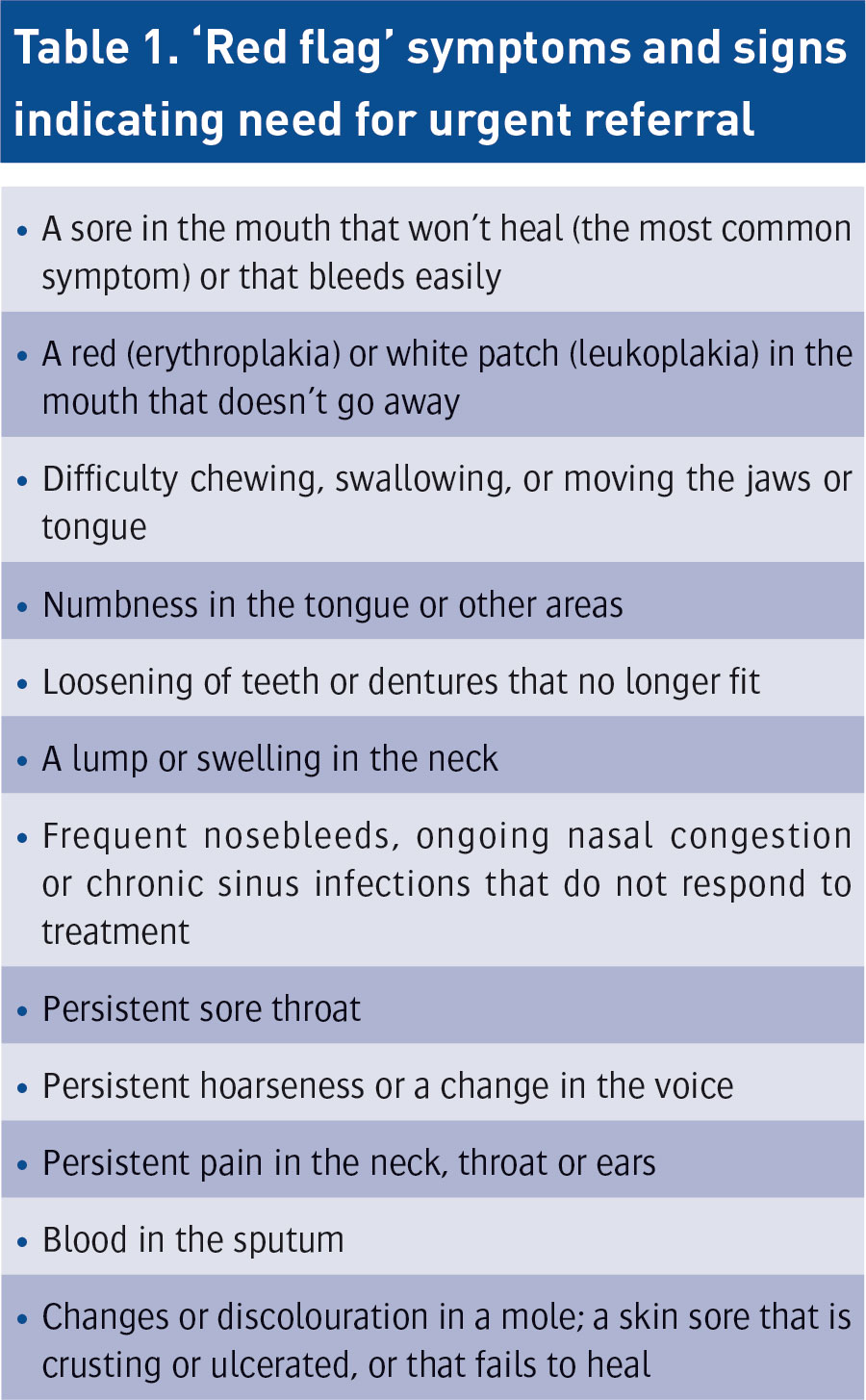
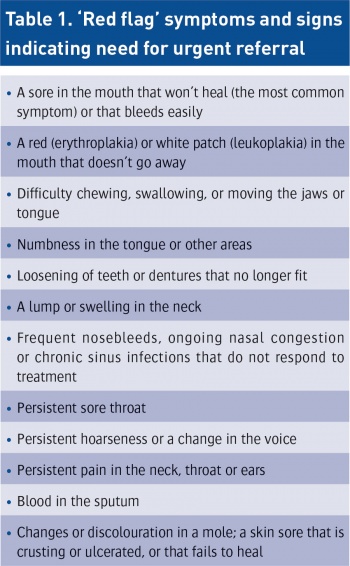
Some head and neck diseases, eg. thyroid cancer, have an excellent prognosis however, unfortunately, two-thirds of all our squamous cell cancer patients present with advanced disease at the time of diagnosis. If these patients fail our first-line of therapy, their prognosis is often very challenging. Like any great science, medicine depends on the delivery and dissemination of knowledge to drive progress. Initial clinical consultations with patients involve a thorough history and detailed examination in an effort to define the clinical problem. Patients with cancers of the head and neck have a large variety of symptoms and signs according to the subsite of the disease. Table 1 highlights the main ‘red flag’ symptoms and signs indicating the necessity for urgent referral.
Head and neck cancers often advance quickly and given the anatomical complexity of the region, they frequently impinge or invade the patient’s airway. This highlights the need for effective and efficient therapy for all these patients. The head and neck has essential functional roles including talking, breathing, smell, vision, hearing, chewing, swallowing and our aesthetic appearance. Therefore, any therapeutic intervention carries significant potential morbidity. Surgery of the head and neck incorporates many different techniques and skills.
(click to enlarge)
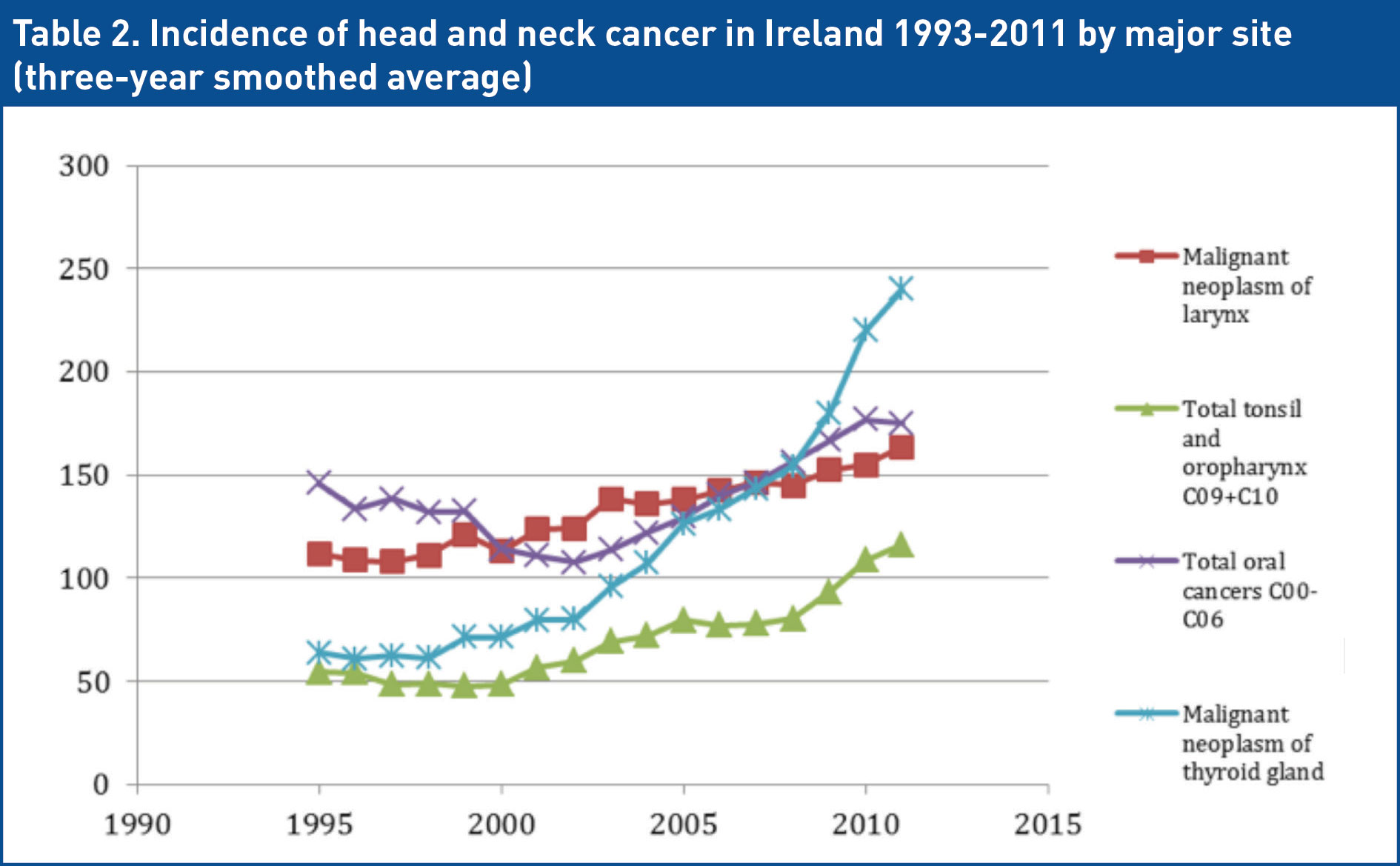
Department of Otolaryngology Head and Neck Surgery (RCSI) and National Cancer Registry (NCR)
National Head and Neck Cancer Audit 1993-2011(click to enlarge)
Anatomical subsites
Larynx
Laryngeal cancer is the second most common type of head and neck cancer. An estimated 12,000 new cases of laryngeal cancer are diagnosed in the US each year. The Department of Otolaryngology at the Royal College of Surgeons in Ireland has, in conjunction with the National Cancer Registry, recently completed a national laryngeal cancer audit between 1997 to 2007. A total of 1,409 cases of laryngeal cancer occurred over the 10-year period. The vast majority of Irish laryngeal cancers occur in men. In 2012, 161 cases were reported. Despite improvements in smoking cessation, the numbers are on the rise. The most common symptoms of laryngeal cancer include hoarseness, a lump in the neck (due to an enlarged lymph node), ear pain and difficulty swallowing.
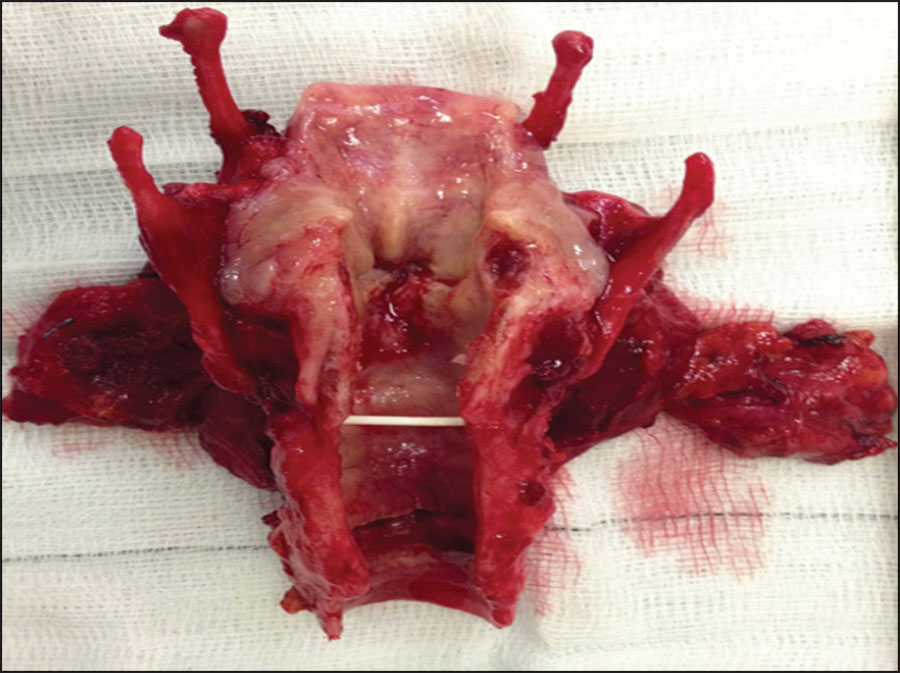
Figure 1. Total laryngectomy for a transglottic T4 SCC cancer(click to enlarge)
Thyroid cancer
An estimated 37,000 people are diagnosed with thyroid cancer each year in the US. Women are nearly three times more likely to develop a thyroid tumour than men. Unlike many other types of cancer, which are more common in older people, thyroid cancer occurs mainly in adults between the ages of 20 and 55. The Department of Otolaryngology at RCSI has, in conjunction with the National Cancer Registry, recently completed a national thyroid cancer audit between 1998 to 2012 where papillary thyroid cancer (PTC) was identified as the dominant subtype representing 49% of thyroid cancer in 1998 increasing to 86% in 2012. In the 2010 to 2012 time period, Irish people were 3.7 times more likely to be diagnosed with PTC than in 1994 to 1996. The dramatic increase in the incidence of thyroid cancer is largely driven by the over diagnosis of papillary thyroid cancer.
In the US, it is estimated that 87% of the PTC cancers now detected are under 2cm in size. Furthermore, 49% are under 1cm in size. What we are witnessing in Ireland and around the world is increased exposure to this subclinical disease reservoir via ultrasonographic screening and radiological investigations for separate pathologies. In Ireland, results from our recent audit with the NCR, confers a five, 10 and 15 year survival of 98.7%, 98.2% and 98.2% respectively. These results correlate with international statistics. The 2014 British Thyroid Association guidelines are an excellent set of recommendations which are considerably more conservative in their approach to well differentiated thyroid cancer and hopefully will reduce the over diagnosis and over treatment of this disease.
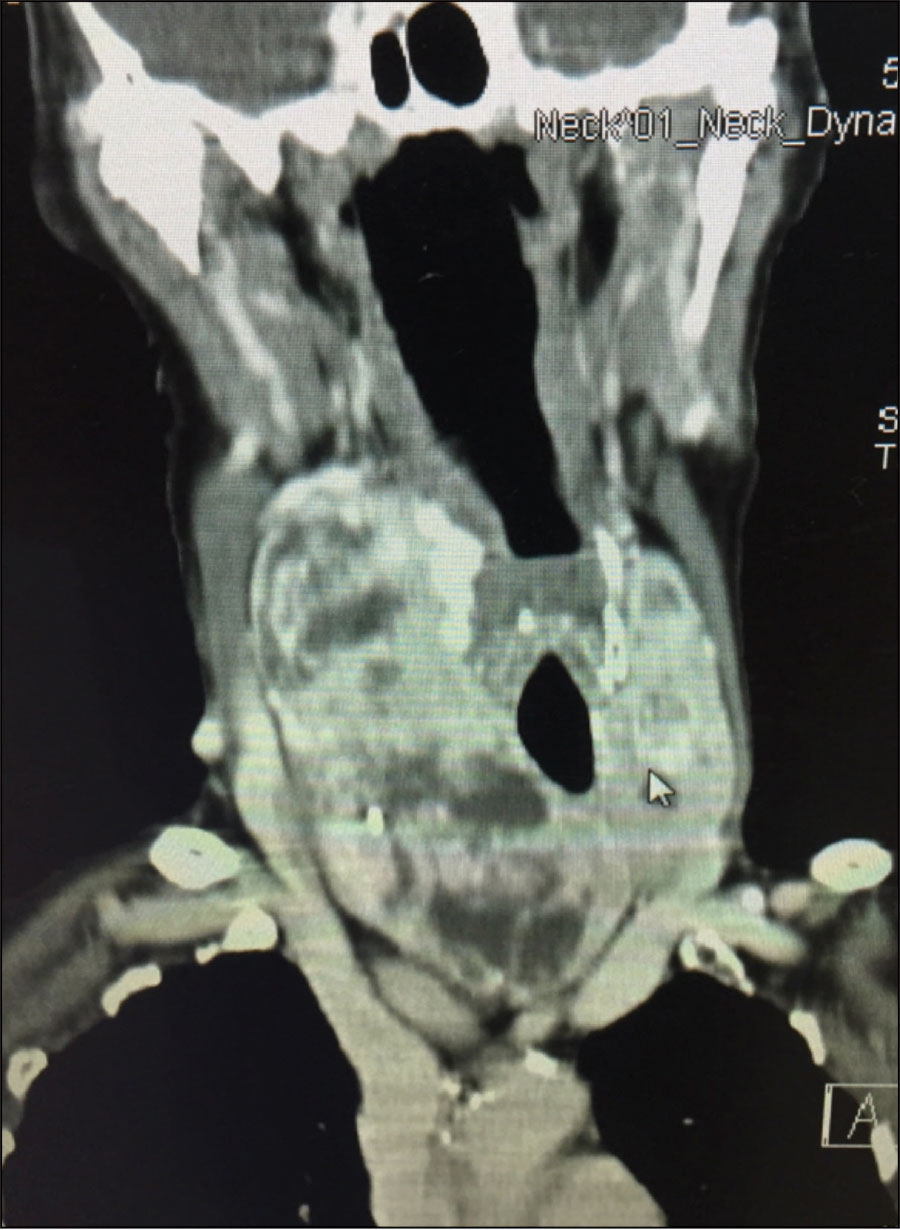
Figure 2. Large well differentiated thyroid cancer in the setting of a multinodular goiter(click to enlarge)
Oral
Oral cancer can begin in the lips, the gums, the retromolar region, the inside of the lips and cheeks, the floor and roof (hard palate) of the mouth and the front of the tongue. Most oral cancers arise in the tongue, the lip, the floor of the mouth and the minor salivary glands. In 2012, 159 cases of oral cavity cancer were reported.
Many oral cancers are found incidentally during a routine dental examination and the ‘Mouth Cancer Awareness Day’ in September highlights the role dentists and general practitioners have in the detection of early oral cancers. Most of these cancers can be cured if discovered early. The most common symptoms include:
A sore or lump on the lip or in the mouth that does not heal
A white and/or red patch on the gums, tongue or cheeks (these white or red areas may also be dysplastic
Unusual or persistent bleeding, pain or numbness in the mouth
Swelling that causes dentures to fit poorly or become uncomfortable.
Skin
Skin cancers are broken into melanoma, non-melanoma (basal cell carcinoma – BCC and squamous cell carcinoma – SCC) and neuroendocrine (Merkel cell). Melanomas are the most aggressive. Signs include a mole that has changed in size, shape, colour, has irregular edges, has more than one colour, is itchy or bleeds. Melanoma staging is now focused on the lesion thickness and ulceration. Of these cancers, 85% are stage 1 or 2.
Of the non-melanoma skin cancers the most common form is a BCC, of which 80% occur in the head and neck. These grow slowly and can damage the tissue around it but rarely disseminate or cause death. It often appears as a painless raised area of skin that may be shiny with small blood vessels running over it or may present as a raised ulcer.
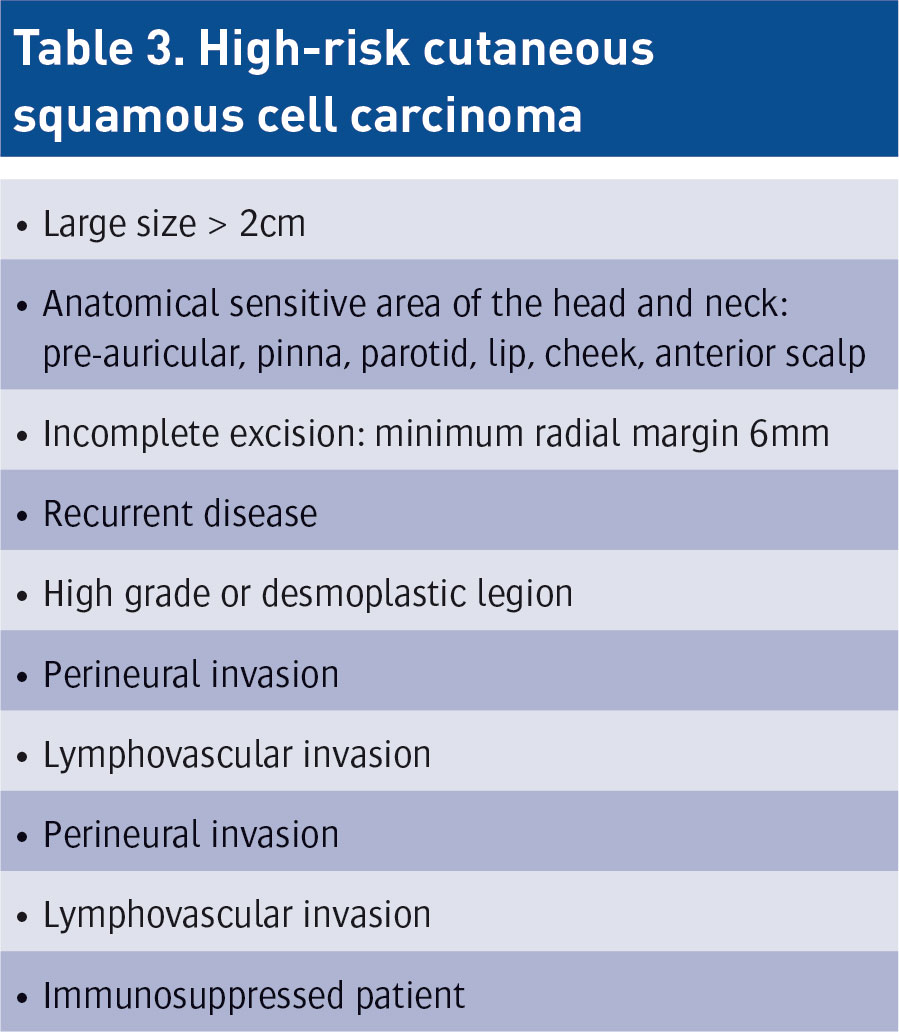
SCC is more likely to spread. It usually presents as a hard lump with a scaly top but may also form an ulcer. High-risk squamous cell carcinomas of the head and neck must be recognised as a separate disease to standard cutaneous squamous cell carcinoma. High-risk SCC includes all of the risk factors in Table 3.
(click to enlarge)
Nasal cavity and paranasal sinus cancer
Each year, approximately 2,000 people in the US are diagnosed with cancer in the mucus-producing tissues that line the nasal cavity and the paranasal sinuses. More than half of nasal cavity and paranasal sinus cancers occur in the maxillary sinuses; fewer cancers develop in the nasal cavity and in the ethmoid sinuses.
These cancers arise more frequently in people who are exposed to wood and metal dusts, asbestos, paint fumes, and air pollution. Symptoms of these head and neck cancers may include persistent nasal congestion, chronic sinus infections that do not respond to antibiotic treatment, frequent headaches or sinus pain, swelling of the eyes, and reduced sense of smell.
Pharynx (throat cancer) and oropharyngeal cancer
Pharyngeal tumours include cancer of the nasopharynx, the oropharynx and the hypopharynx. Each year in the US, an estimated 11,800 people develop pharyngeal cancers. Odynophagia, dysphagia, neck mass, persistent pain and referred otalgia pain are the common presentations.
The oropharynx is located behind the mouth and includes the base of the tongue, the soft palate and the area around the tonsils. Smoking and chewing tobacco and heavy alcohol use are the most common risk factors for oropharyngeal cancer, but there is evidence that a diet low in fruits and vegetables is clearly linked to this form of head and neck cancer. Prior infection with human papillomavirus (HPV) is also a particularly strong risk factor for this cancer site.
Symptoms of oropharyngeal cancer may include a lump in the neck or throat, persistent sore throat, hoarseness, difficulty swallowing and ear and/or jaw pain.
(click to enlarge)
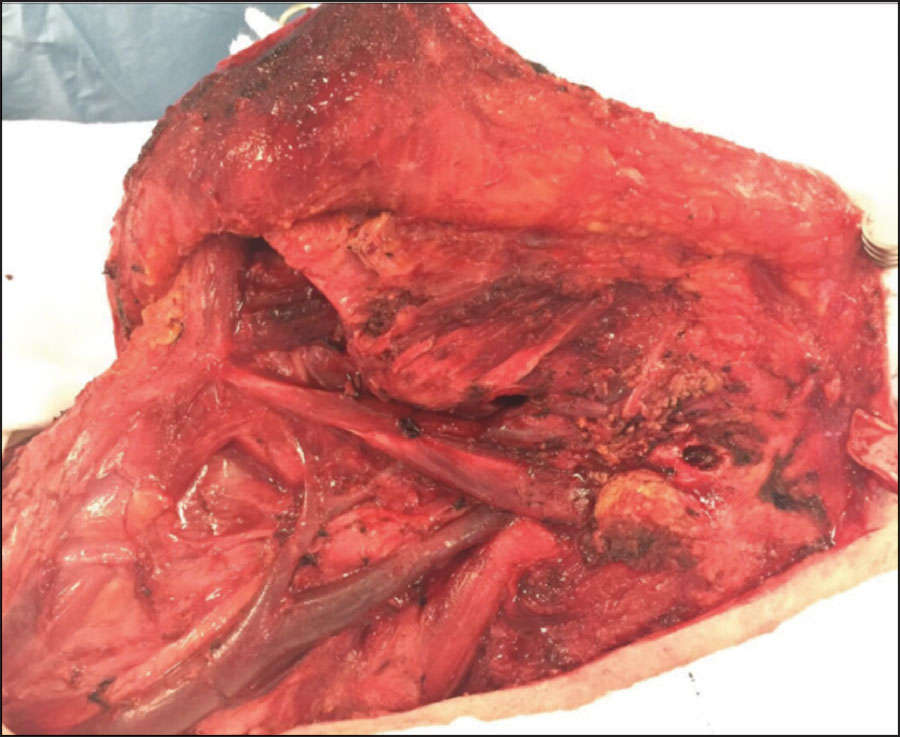
Figures 3 and 4. High grade cutaneous SCC with dissemination and into parotid and cervical lymphatics(click to enlarge)
Risk factors – smoking, alcohol and HPV
Head and neck cancers form after an accumulation of genetic events, which are accelerated by genomic instability related to carcinogen, or cancer causing exposures, particularly tobacco and alcohol. The link between cancer and cigarette smoking is now indisputable. Both alone and in synergy with alcohol, these risk factors are the consistent findings within the social history of the majority of our patients. Tobacco use and alcohol consumption account for an estimated 74% of cancers of the head and neck.
On a cellular level, tobacco exposure is associated with increased rates of p53 mutations. Mutations in p53 have been associated with decreased overall survival and increased recurrence of disease because of decreased therapeutic response.
Human papilloma virus (HPV) is a well-documented carcinogenic risk factor in the context of cervical cancer. Although there are more than 100 types of HPV, only a small number of these are considered carcinogenic. One type, HPV 16, is responsible for the vast majority (more than 90%) of HPV head and neck cancers. HPV causes a distinct subset of HPV positive head and neck cancers that arise in the lymphoid tissues of the palatine and lingual tonsils of the oropharynx. Patients with a HPV driven oropharyngeal cancer are predominantly male, within the 50 to 60-year-old age group and often without a smoking history.
HPV is a sexually transmitted infection. Although it is difficult to delineate which specific behaviours confer the greatest risk of oral HPV infection and HPV-head and neck cancers, oral sexual behaviours are believed to be the primary mode of transmission. The proportion of oropharyngeal cancers attributable to HPV in the US rose from 16% in the 1980s to near 80% in the past decade. We are seeing a similar pattern emerge in Ireland.
HPV positive tumours are significantly more responsive to therapy than HPV negative cancers because there are fewer mutations present within the viral carcinogenic cancers compared to the classical chemical carcinogenic (smoker/drinker) tumours. Therefore, having a HPV positive tumour brings with it a survival advantage compared to classical cancers in this region. Despite the overwhelming evidence supporting the role of HPV in the aetiology of oropharyngeal cancer, it has not been conclusively linked to other cancers, namely oral cancer or larynx cancer.
HPV vaccination
In Ireland, we have an excellent HPV vaccination programme to reduce the risk of cervical cancer for girls. Vaccination is most effective in childhood or early adolescence, prior to the initiation of sexual activity and exposure to HPV. Vaccination against HPV can be administered in two forms. HPV 16 and 18 are the vaccine types for the bivalent vaccine, and HPV 6, 11, 16 and 18 are the vaccine types for the quadrivalent vaccine. By the end of 2013, more than 144 million doses of the quadrivalent vaccine and about 41 million doses of the bivalent vaccine had been distributed worldwide. WHO’s Global Advisory Committee on vaccine safety has reviewed safety data for both vaccine types on a number of occasions, most recently in March 2014. These reviews continue to affirm HPV vaccines as highly immunogenic, safe and effective.
The incidence of HPV positive head and neck cancer is now expected to exceed cervical cancer incidence in the US by 2020 and therefore the role of vaccination is essential. It is imperative that we now introduce a vaccination programme for Irish boys as some of our international counterparts have done to protect both girls and boys against the oncogenic dangers of this virus both in the cervix and the oropharynx.
A multidisciplinary approach
Decision-making in the treatment of any head and neck cancer patient is made with input of the multidisciplinary team (MDT). The MDT includes ear, nose and throat (ENT) head and neck surgeons, radiation oncologists, maxillofacial surgeons and allied dental experts, neuro-radiologists, pathologists, medical oncologists, physiotherapists, speech and language therapists, nutritionists and oncology nursing specialists. Successful treatment of patients with head and neck cancer is predicated on MDT strategies to maximise oncologic control and minimise the impact of therapy on form and function. Contemporary oncology follows evidence-based medicine, in other words, statistically proven therapeutic modalities published in peer-review journals. Anything beyond that is simply reckless and dangerous.
Overall, some head and neck cancers have an excellent prognosis. Early detection is the key with urgent referral to a head and neck cancer service. In Beaumont Hospital we run a rapid access service every Thursday afternoon. On a Friday morning we have our main head and neck cancer clinic. All suspected cancer referrals to any subsite of the head and neck are dealt with in an efficient manner with full MDT evidenced-based decision making and therapeutic strategy.
References
Rettig E, D’Souza G. Epidemiology of Head and Neck Cancer. Surg Oncol Clin N Am 2015; 24(3): 379-396
Georgopoulos R, Liu JC. Examination of the patient with head and neck cancer. Surg Oncol Clin N Am 2015; 24(3): 409-421
O’Neill JP, Shaha AR. Nutrition management of patients with malignancies of the head and neck. Surg Clin North Am 2011 Jun; 91(3):631-639
O’Neill CB, O’Neill JP, Atoria CL et al. Treatment complications and survival in advanced laryngeal cancer: a population-based analysis. Laryngoscope 2014 Dec; 124(12): 2707-13
Clump D, Bauman J, R Ferris. Cancer of the Oropharynx. Surg Oncol Clin N Am 2015; 24(3): 509–520
Mydlarz W, Weber R, Kupferman M. Cutaneous malignancy of the head and neck. Surg Oncol Clin N Am 2015; 24(3): 593-613
Montero P, Patel S. Cancer of the Oral Cavity. Surg Oncol Clin N Am 2015; 24(3): 491-508
 (click to enlarge)
(click to enlarge)