The Irish Helicobacter pylori Working Group (IHpWG) was recently set up with the express aim of improving eradication rates by determining the optimum treatment protocol
Dr Neil O’Morain, Specialist Registrar in Gastroenterology, Tallaght Hospital, Dublin and Prof Deirdre McNamara, Associate Professor Gastroenterology and Director TAGG Research Centre, Tallaght Hospital/TCD, Dublin
Helicobacter pylori has not gone away. An estimated 35% of Irish adults will test positive for Helicobacter pylori (H. pylori), making it still one of the commonest infections encountered in Ireland. It is associated with significant disease including peptic ulcers and gastric cancer. While the global prevalence of this hardy bacteria is decreasing, the management of H. pylori has become increasingly challenging. Eradication rates are decreasing in the face of increasing antibiotic resistance, and issues with patient compliance persist.
Europe-wide consensus guidelines have been developed over the past three decades to inform best practice treatment protocols. There is, however, a growing understanding that key treatment recommendations should be informed by local antibiotic resistance patterns. H. pylori eradication therapies should aim to eradicate infection in at least 90% of treated patients, however this target is not being met. Irish eradication rates have steadily decreased over the past decade, with resistance to individual antibiotics reportedly as high as 50% in certain areas.
The Irish Helicobacter pylori Working Group (IHpWG) was recently set up with the express aim of improving eradication rates by determining the optimum treatment protocols for an Irish population. The IHpGW paid particular attention to Irish resistance rates and antibiotic availability. By raising awareness once more of this, at times, forgotten bacterium, it is hoped that physician and patient engagement can be augmented and efforts focused on improving eradication rates, thus avoiding the negative consequences of untreated or undiagnosed H. pylori.
What is Helicobacter pylori?
H. pylori is a flagellated gram negative bacillus which is acquired in childhood. Humans are the only host and it is spread from person to person, usually from parent to offspring, however children can spread it among themselves via oral-oral route. Most individuals infected remain asymptomatic but there are serious complications associated with the infection, such as peptic ulcer disease (PUD) and gastric cancer. The majority of peptic ulcers are caused by this bacterium, and H. pylori has been recognised as a group 1 human carcinogen for gastric adenocarcinoma. Effective treatment of this infection is important to avoid these complications.
The European Helicobacter Pylori Study Group (EHSG), founded in 1987, has set out a series of guidelines to recommend who, when and how to treat this infection. The guidelines, named after the Dutch city of Maastricht where the first edition was compiled, is now on its fifth edition, reflecting the evolving complexity of H. pylori. The IHpWG recently published the first Ireland-specific guidelines based on local antibiotic resistance patterns. These guidelines are the result of a multidisciplinary collaboration between Irish and European gastroenterologists, microbiologists, pathologists and scientists.
A number of consensus statements outline their approach to the detection and treatment of this fastidious bacterium. There are 15 statements in total covering topics ranging from diagnosis, treatment, post-eradication testing, antimicrobial susceptibility testing and rescue therapy. The following statements have been selected to highlight recent changes in treatment protocols, as well as key components of eradication strategies that will be of particular interest to general practitioners and general physicians.
(click to enlarge)
Statement 1: All patients with symptoms related to the upper gastrointestinal tract should be tested for H. pylori
On the basis of the links between H. pylori infection and ulcers, gastric cancer and MALT (mucosa-associated lymphoid tissue) lymphoma, H. pylori detection and treatment is recommended in all symptomatic patients. A ‘test and treat’ policy is recommended for individuals presenting to a family practitioner with symptoms of dyspepsia under the age of 50 as it is unlikely these patients would have developed gastric cancer. H. pylori-associated gastric cancer usually presents in the seventh and eight decade.
The recognition, diagnosis and treatment of H. pylori has resulted in a dramatic decrease in the incidence of peptic ulcer disease.
More recently the Maastricht guidelines have suggested a ‘search and treat’ approach which includes searching for and treating patients with a positive family history (first degree relative) of gastric cancer, aged at least 45, and presenting with alarm symptoms such as weight loss, dysphagia, overt gastrointestinal bleeding, abdominal mass or iron-deficiency anaemia.
Statement 2: The urea breath test is the recommended non-invasive test for H. pylori
Non-invasive tests for H. pylori include the urea breath test (UBT), the stool antigen test and serology. Recent data from the Irish healthcare setting indicate infection rates of 36-37% among patients referred for the UBT and 19-36% among patients referred for endoscopy. The UBT involves the ingestion of 13C or 14C-labelled urea. If present, the H. pylori enzyme urease converts the C-labelled urea into labelled carbon dioxide, which is detected in a breath sample.
Fasting for at least four hours before testing is recommended. The UBT is easy to perform and accurate, with reported sensitivities and specificities of 88-96% and 93-100%, respectively and is the recommended non-invasive test for H. pylori where available. Crucially, all patients referred for UBT must be off all proton pump inhibitors and antibiotics for two weeks prior to the test.
Local evidence from Ireland demonstrates inferior results using the stool antigen test compared with the UBT, with a sensitivity of 62%. Serology is useful in epidemiological studies but not useful in practice as it takes a considerable time for antibody levels to fall and a serology test needs to be validated locally. UBT is therefore the non-invasive test of choice in detecting H. pylori infection.
Statement 3: A combination of histology taken from the antrum and corpus and a rapid urease test are recommended for invasive H. pylori testing
An alternative invasive test to detect H. pylori involves biopsy sampling at gastroscopy for histological sampling and rapid urease testing. Biopsies for culture and sensitivity can also be taken at this time. The rapid urease test is dependent on the bacteria releasing urease which induces a colour change in a specific medium. A positive result can be detected within 30 minutes of endoscopy. This was the method of choice prior to the development of the non-invasive options and remains the gold standard.
Biopsy sampling for the bacteria should always be performed when a gastroscopy is undertaken. To account for the patchy distribution of H. pylori, histological sampling for H. pylori diagnosis should include an antrum biopsy (2-3cm in front of the pylorus) and a corpus biopsy.
Statement 6: Post-eradication testing must be performed. If gastroscopy is not required, a urea breath test is recommended for post-eradication testing
As eradication rates for H. pylori are decreasing and symptoms are not a good indicator of treatment success, post-eradication testing must be performed. Testing for H. pylori eradication should be performed at least four weeks following the completion of any therapy for H. pylori. The UBT is considered the best option for confirmation of H. pylori eradication.
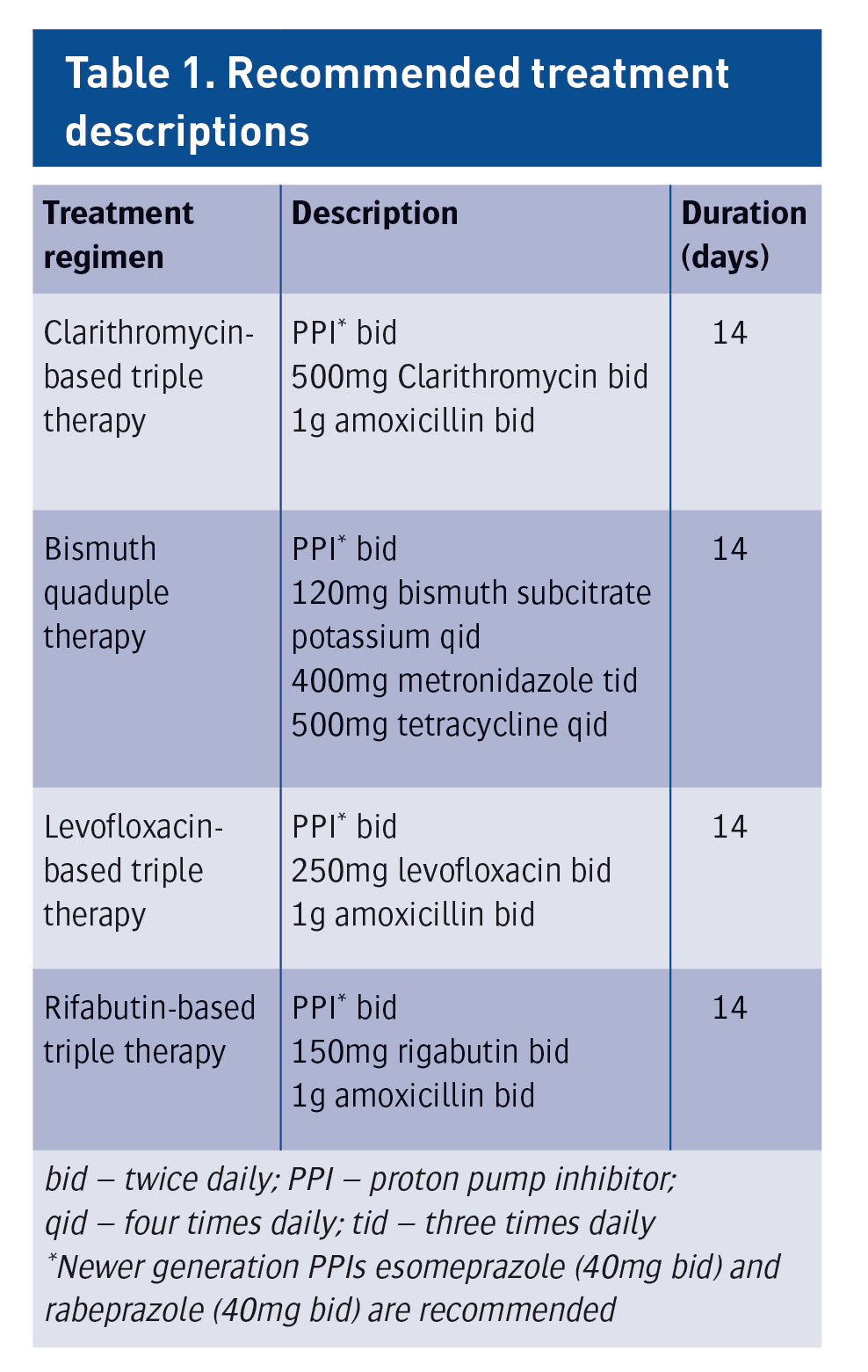
Statement 8: Standard triple therapy for a duration of seven days can no longer be recommended
Recent data from Irish studies suggest an eradication rate of 57% for clarithromycin-based seven day triple therapy. The most recent Maastricht guidelines suggest a net therapeutic gain from extending the treatment period to two weeks. This the most significant change in the treatment paradigm, and these guidelines now reflect that with a 14-day triple therapy preferred.
Statement 9: 14-day clarithromycin-based triple therapy with a high-dose proton pump inhibitor is recommended. Bismuth quadruple therapy for 14 days is an alternative if available
Numerous factors contribute toward treatment failure, including high bacterial load, low gastric pH and impaired mucosal immunity; however, treatment failure is largely associated with the emergence of antibiotic-resistant H. pylori and with poor patient compliance. Several strategies have been shown to improve the success rate of standard triple therapy. Many meta-analyses and recent observational studies have shown that increasing the duration of first-line triple therapy enhances eradication success, with treatment durations of 14 days showing the most effective eradication. The recommended first-line triple therapy therefore consists of a clarithromycin-based therapy for 14 days.
Persistent H. pylori infection should be treated with levofloxacin-based second-line therapy. An alternative option is a bismuth-based quadruple therapy, however the availability of bismuth in Ireland is limited at present. It is important not to repeat a failed treatment. If first-line treatment has failed, proceed to the second-line combination. If second-line treatment fails, a referral should be made for gastroscopy with culture and sensitivity sampling. Treatment can then be tailored according to antibiotic susceptibilities. Treatment protocols may change in the future according to antibiotic resistance patterns. The IHpWG will continue to monitor resistance patterns and advise accordingly.
Due to very high resistance rates, metronidazole is no longer a recommended therapy option for penicillin-sensitive patients. Amoxicillin may be replaced with metronidazole for penicillin-allergic patients, either combined with clarithromycin (first line) or levofloxacin (second line).
(click to enlarge)
Embracing new technology
The IHpWG recently launched the new smartphone based application ‘H. pylori Care’. This app was developed as a guideline for diagnosis and treatment of H. pylori in adult patients in Ireland based on available data. This free-to-download and easy-to-access app provides up-to-date information for both clinician and patient. It is hoped that by enhancing awareness of the challenges facing H. pylori eradication in Ireland today via this new app, treatment success rates will improve. The app can be accessed as follows:
 (click to enlarge)
(click to enlarge)