Assessment tools are widely used in medicine of old age and particularly in the nursing home setting, where their use seems to be increasing noticeably. An understanding of what these tools measure and how they are devised can help the GP get a better understanding of concerns raised by nursing staff and provide an objective measurement of a patient’s decline or improvement over time. Below is a brief description of some of the more common assessment tools used in Irish nursing homes.
Nutrition
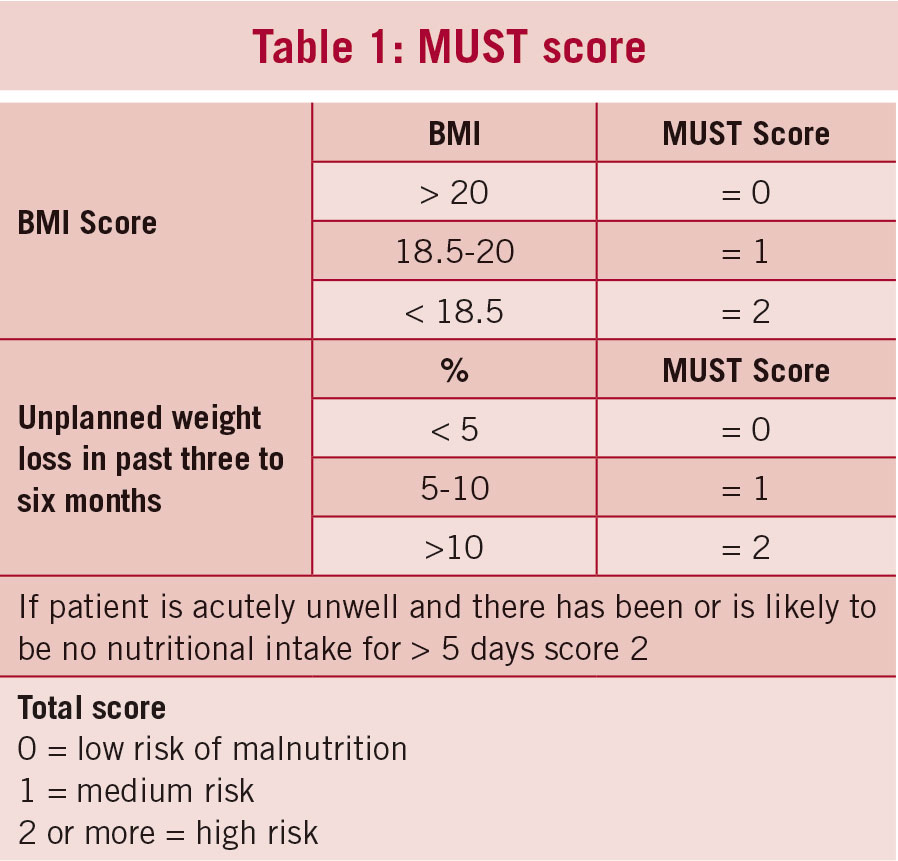
The MUST score (malnutrition universal screening tool) is now in widespread use and is usually part of the nutritional assessments of nursing home residents required under HIQA. It is very easy to learn and apply and has therefore proved popular with staff. It attempts to assess the risk of malnutrition by applying a score to BMI, unplanned weight loss and recent acute illness (see Table 1). A score of 2 or more suggests a high risk of malnutrition and in most policies would involve a referral to a dietician and a plan of action to address weight loss.
(click to enlarge)
Limitations of the score are that it is sometimes very difficult to accurately assess the height of nursing home residents and therefore get a reliable BMI. An unrelated issue is that in some elderly patients with dementia or incurable chronic disease, weight loss is inevitable.
There is sometimes a feeling that the nursing home is ‘failing’ the resident when weight loss continues despite efforts to reverse this. The GP and dietitian may have a role in moving the focus of care away from attempting to reverse inevitable weight loss and instead on to issues which have a greater impact on the quality of life of the patient.
Activities of daily living
The original Barthell Index was designed to measure the level of disability among patients with neuromuscular and musculoskeletal conditions receiving inpatient rehabilitation. It is now, however, widely used in nursing homes and other elderly care settings as a global assessment of a resident’s ability to function independently. The original index was measured in steps of five points to give an overall score out of 100.
The version used in most nursing homes is a modified one which scores patients out of 20 on a variety of areas including mobility, toilet use, dressing, feeding, bladder and bowel. As long as the index is applied consistently, it can provide a very useful guide to functional deterioration or improvement in a nursing home patient’s independence.
The index is open to observer error and ideally should be carried out by the same individual when comparing scores over time. Patients can be scored in the Barthel Index by asking them to score themselves, by observation or by testing the patient on the various activities. The reliability of the index has been shown to be weakest where patients score themselves, especially if they have any degree of cognitive impairment.1
Depression
Most GPs will be familiar with the Geriatric Depression Scale, which is a 15-item questionnaire used to help diagnose depression in older people. Although it is considered to be useful in patients with an MMSE score of 14 or better, care is required when applying it to patients in a nursing home setting. Questions such as ‘Have you dropped many of your activities and interests?’ or ‘Do you often get bored?’ may be answered in the positive not because of depression, but because the individual can no longer get to their local bridge club meetings or they don’t find the daily activities in the nursing home particularly stimulating.
Similarly the question ‘Do you think it is wonderful to be alive now?’ is a little difficult to ask patients who you suspect are having difficulty adjusting to life in a nursing home. Despite these reservations, it can be a useful tool for both community-based and nursing home patients and should only take five to 10 minutes to complete.
As the name suggests, The Cornell Scale for Depression in Dementia (CSDD) is a scoring tool designed for those with dementia but who can at least communicate basic needs. The scale is commonly used in Irish nursing homes and the GP may be asked to review a patient with scores of 12 or more out of a possible 38.
Scores are determined by a combination of observations made by the main carer and interview with the patient. Observation of symptoms and signs should be made by care staff in the week prior to the test being carried out. As with other scores based on observation rather than patient responses, it is prone to observer error and ideally should therefore be carried out by the same nurse on each occasion.
Falls
Predicting the likelihood of a fall in a nursing home resident can be a bit like predicting Irish weather, but a variety of risk scores have been devised and used. There is poor evidence to support the use of these assessment tools and recent NICE guidelines on falls in elderly patients favoured a multifactorial assessment of elderly patients rather than the use of scoring systems.2
HIQA however, demands these are used as part of falls risk assessments and currently the STRATIFY and FRASE assessment tools appear to be the ones generally in use in Ireland. Indeed, both of these assessment tools are recommended in Nursing Home Ireland’s advisory document on the assessment and care of nursing home patients.3
STRATIFY (St Thomas risk assessment tool in falling elderly inpatients) measures five risk factors for falls including past history of falls, patient agitation, visual impairment, need for frequent toileting and transfer ability and mobility. It also incorporates two items on the Barthel’s Index covering transfer and mobility allowing these to be reused in STRATIFY. A score of two or more indicates a high risk of falls. In general, nursing homes will get on with the job of minimising the risk of falls in patients deemed at high risk, but GPs may be asked to sign off on particular measures.
FRASE (falls risk assessment scale for elderly) scores patients on 27 factors likely to increase their risk of falls, including age, gait, sight, hearing and balance. It also includes extra marks for those on sedative medication or antihypertensive agents, reflecting the evidence that these agents increase falls significantly in this group of patients. Patients with scores of greater than 12 are considered at high risk of falls and this should trigger fall prevention measures.
Pain
Diagnosing the presence and intensity of pain in patients with cognitive impairment can be very difficult and yet it is central to the management of many symptoms including anorexia, agitation and challenging behaviour.
There is a plethora of pain assessment scales available, but the Abbey Pain Scale is one of a number that can be used in patients who are unable to verbalise symptoms. The score is based on observations by the care staff looking at six areas including facial expression, vocalisation and behavioural change.
Like other scores, it is prone to observer error and the time interval since analgesic medication was administered needs to be recorded. Patients with a persistent score of eight or more out of a possible 24 should be reviewed.
Not surprisingly, more detailed assessment tools score more favourably when compared with the Abbey Pain Scale and in particular the PAINAD (pain assessment in advanced dementia) is an alternative which fared better in a recent systematic review.4
Conclusion
Assessment tools and scores should only be used as an aid to diagnosis and not relied upon entirely to arrive at a particular conclusion. The opinion of a good carer or nurse who knows the patient well can often be more valuable. They can however, prove useful in tracking changes in mood, pain or function over time.
If you wish to comment on this article or join an online discussion group for GPs involved in nursing homes please contact the author at Email: brianmeade@iol.ie with your ICGP membership number.
References
Sainsbury A et al. Age and Ageing 2005; 34: 228-232
NICE guidelines [CG161]. Falls in older people: assessing risk and prevention. June 2013 nice.org.uk/guidance/qs86
Assessment and Care Planning Integrated Resident Record and Policy Documentation Set. Nursing Homes Ireland, as accessed on
www.nhi.ie/doc.php?id=144
Zwakhalen S et al. Pain in elderly people with severe dementia: A systematic review of behavioural pain assessment tools BMC Geriatr. 2006; 6: 3
 (click to enlarge)
(click to enlarge)