A team at a major Dublin hospital evaluated lipid management post ACS and found much room for improvement
Dr Issam Altnji, Cardiology Regristrar, St James's Hospital, Dublin, Dr Naief Almagal, Cardiology Registrar, St James's Hospital, Dublin, Dr Suleiman Suleiman, Specialist Registrar in Cardiology, St James's Hospital, Dublin, Dr Myles McKittrick, Cardiology Registrar, St James's Hospital, Dublin, Dr Anna Hayes, Senior House Officer, St James's Hospital, Dublin and Dr Caroline Daly, Professor of Cardiology, St James's Hospital, Dublin
Patients with acute coronary syndrome (ACS) are at high risk of recurrent cardiovascular events.1 Lipid-lowering therapy plays a vital role in secondary prevention post ACS; however, many patients fail to achieve their target lipid goals.
The European guideline recommendation is to re-evaluate low-density lipoprotein (LDL) cholesterol four to six weeks following ACS to determine whether a reduction of at least 50% from baseline and a goal of LDL-C < 1.4mmol/L (< 55mg/dL) has been achieved.1
Objectives
The objective of this study was to evaluate the performance of a large Irish interventional cardiology centre in lipid measurement following the initiation of high-intensity statin therapy and to establish whether patients’ lipid profiles were assessed within a guideline-directed recommendation.
Data samples
The retrospective audit focused on patients admitted to St James’s Hospital Cardiology Department from June 2022 to September 2022. The sample size of 158 patients was determined based on all eligible individuals within the specified timeframe.
Inclusion criteria encompassed patients diagnosed with acute coronary syndrome (ACS), including ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), or unstable angina (UA).
Data collection
Data collection involved a comprehensive review of biochemical databases and medical notes for patients admitted to St James’s Hospital Cardiology Department. Demographic details like age, gender, and mode of admission were compiled. A three-question survey was created to gather information on lipid assessment after discharge, recommendations for lipid evaluation and target goal timing, and patient education on checking lipid profiles:
• Was the LDL checked after discharge in four to six weeks?
• Was there any recommendation in the discharge summary about the LDL target and timing of evaluation?
• Have you been told to check your lipid profile in four to six weeks’ following discharge?
Two survey questions were clarified through direct telephone communication with patients for accuracy.2 The discharge electronic patient record system and all data were entered for tabulation and analysis. This facilitated the comparison of information to identify potential trends or patterns in the dataset.
Data analysis
Data were first expressed as frequency (%), and the percentage of patients attaining the required LDL ranges of 0.05 significance level was calculated. Analysis was undertaken by IBM SPSS Statistics for Windows, version 23.
Zhao et al argue that Pearson Chi-Square is appropriate where there is a need for robustness and flexibility when handling multiple data sets.3 Therefore, the test was applied to calculate the association between lipid assessment and the three categories of ACS (STEMI, NSTEMI, and UA). P-values of < 0.05 were considered statistically significant. Moreover, a re-audit will be commenced to assess for improvement in our centre’s performance and standards.
Standard guidelines
Standard procedures for optimal lipoprotein cholesterol reduction management involve re-assessing LDL-cholesterol four to six weeks post-discharge following acute coronary syndrome (ACS). This ensures the effectiveness of lipid-lowering therapy and identifies patients needing treatment adjustments.4
Monitoring therapy adherence, counselling, and patient education are essential to enhance understanding of therapy benefits. Regular follow-up appointments assess patient progress and allow for treatment plan adjustments.5 Close collaboration among healthcare providers, sharing patient information and updates, ensures a co-ordinated approach to lipid management.6 Adhering to these guidelines optimises LDL-cholesterol management, reducing cardiovascular risk and improving patient outcomes.
Results
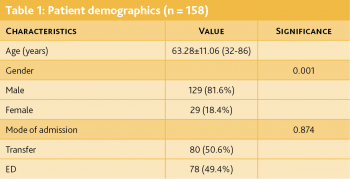
The age of the participants ranged from 32 to 86 years with a mean age of 63.28 years. The majority of patients were male (81.6% versus 18.4%, p < 0.001). The mode of admission was transfer (TF) (50.6%) or via the emergency department (ED) (49.4%) with no significant statistical difference between them (p = 0.874) (see Table 1).
(click to enlarge)
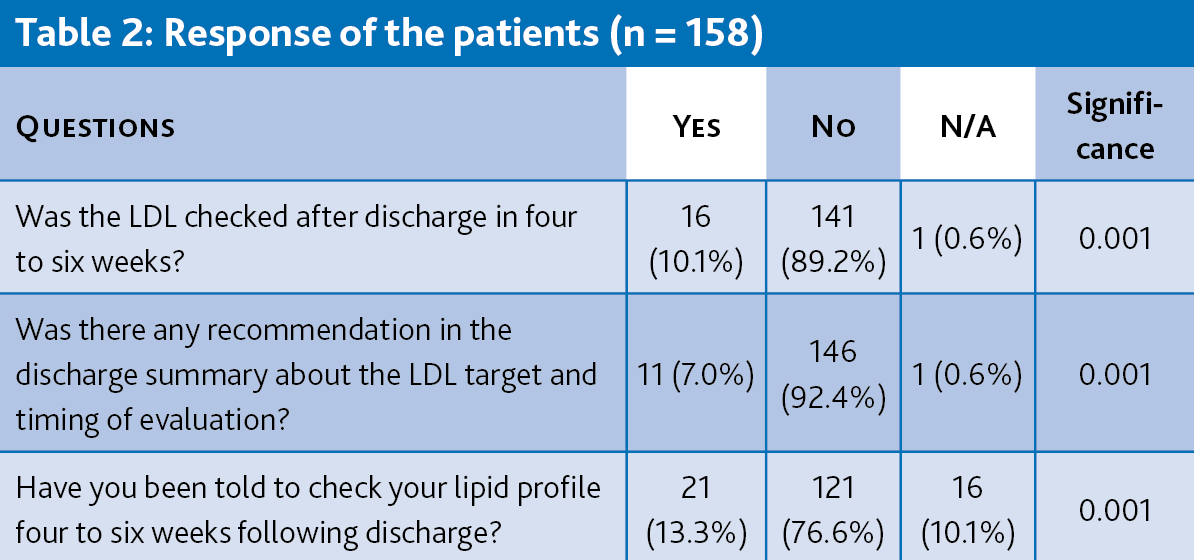
Lipid assessment after discharge four to six weeks post-sentinel event was only observed in 16 (10.1%) patients; recommendations regarding the timing of lipid evaluation and target goal was revealed in 11 (7.0%) patients, while 21 patients reported that they were only instructed to check their lipid profile in four to six weeks (13.3%) (see Table 2).
(click to enlarge)
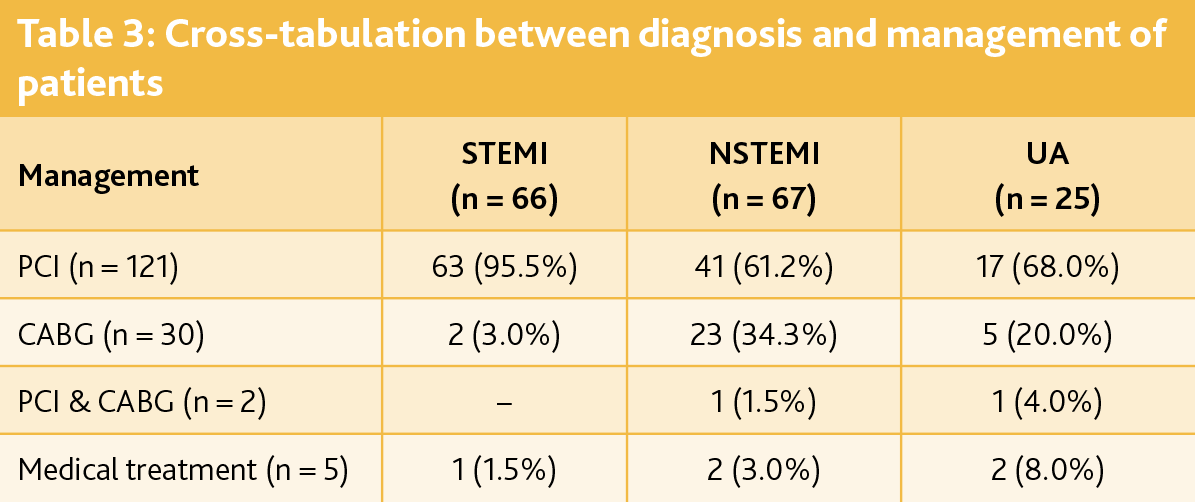
Unstable angina (UA) made up 16% of the presenting cause, with the majority of patients being divided equally between Non-ST-elevation and ST-elevation myocardial infarction (NSTEMI and STEMI) -42.4% and 41.8% respectively. A total of 121 patients underwent percutaneous coronary intervention (PCI) (76.6%); 30 were deemed to have coronary disease that subsequently required coronary artery bypass grafting (CABG) (19.0%); medical treatment was reserved for five (3.2%) patients, and two patients needed both PCI and CABG (1.3%)
As expected, most STEMI patients were managed by primary PCI (95.5%) with only 3.0% requiring CABG and one case being conservatively managed with medical treatment alone (1.5%); 61.2% of NSTEMI patients were treated by PCI, 34.3% by CABG, 3.0 % by medical management and only one patient undertook combined PCI and CABG.
The management of UA patients can also be seen in Table 3, which posits that re-audits are necessary during lipid-lowering therapies while seeking secondary prevention.7 Moreover, this enhances constant evaluation for improvement in the centre’s performance and standards of care.
(click to enlarge)
Discussion
This retrospective study conducted at St James’s aimed to assess lipid management practices following the initiation of high-intensity statin therapy in patients with acute coronary syndrome (ACS). The findings revealed a significant gap in adherence to European guidelines, with only 10.1% of patients having their LDL cholesterol re-evaluated within the recommended four to six weeks post discharge. Recommendations for LDL target and evaluation timing were inadequately reflected in discharge summaries (7.0% adherence), while 13.3% reported being advised to check lipid profiles within the specified period.
The study emphasises the need for improvement in lipid management practices to enhance patient quality of care and adherence to guidelines. Previous research underscores the vital role of lipid-lowering therapy in secondary prevention post-ACS, emphasising the importance of achieving target LDL cholesterol levels and monitoring within guideline-directed timeframes. Non-compliance or undertreatment may heighten the risk of recurrent cardiovascular events and poor outcomes.8
Identified contributing factors include poor communication between patients and healthcare providers, insufficient patient education on LDL cholesterol reduction benefits, and the necessity of timely re-assessment. Adequate documentation of LDL targets in discharge summaries is also deemed essential.9 The study suggests addressing these factors to bridge the identified gap in lipid management practices.
Recommendations and quality improvement plan
The study proposes recommendations and quality improvement plans to enhance lipid management and patient outcomes in the context of acute coronary syndrome (ACS). Firstly, it suggests improving patient education within cardiology facilities to inform patients about the benefits of lipid management, adherence to guideline-directed timelines, and LDL-C targets.2
Effective communication between healthcare providers and patients is emphasised to convey lipid management objectives and potential risks. Secondly, effective communication between healthcare providers and patients is emphasised to convey lipid management objectives and potential risks.10 The study advocates for a centralised system to share LDL-C management information among healthcare providers for seamless follow-up and monitoring. Improved documentation practices, including standardised templates for discharge summaries and cardiac rehabilitation notes, are recommended.
Continuous monitoring and evaluation of patients are crucial for quality improvement. Key performance indicators (KPIs) such as the percentage of patients with LDL-C reassessed and those achieving targets within a specified timeframe are suggested for measurement.10 Regular audits and evaluations should be conducted to assess the effectiveness of implemented quality improvement procedures. The overall goal is to enhance lipid management practices, reduce the risk of recurrent cardiovascular events, and improve patient outcomes.3 Implementation of these recommendations, including education, communication enhancement, and proper documentation, can be expected to result in improved adherence to guidelines.
Re-audit
To determine whether the adjustments outlined in the action plan following the initial audit in December 2022 had improved the performance in lipid control after ACS, a re-audit was conducted.
Methodology
This re-audit assessed current practices after implementing an action plan derived from the baseline audit. A retrospective review of 45 randomly selected recently-discharged patients was conducted using electronic records and phone calls. The aim was to determine if lipid checks occurred within the recommended timeframe after discharge. Baseline demographics were examined for differences between the baseline audit and re-audit.
The sample was chosen randomly to avoid repetition of baseline audit patients and to allow time for action plan implementation. The re-audit included three questions: whether the recommendation to repeat a lipid profile was in the percutaneous coronary intervention procedure note, in the discharge summary, and if the patient had their lipid profile checked by their primary care physician within four to six weeks post-discharge. The primary focus is on action plan implementation, with additional questions about the PCI procedure note compared to the baseline audit. Notably, patients were not directly asked if they were informed about the recommendations.
Results
The participants’ ages ranged from 43 to 88 years, with a mean age of 60.09 years, comparable to the baseline audit. The majority were male (77.8% vs. 22.2%).
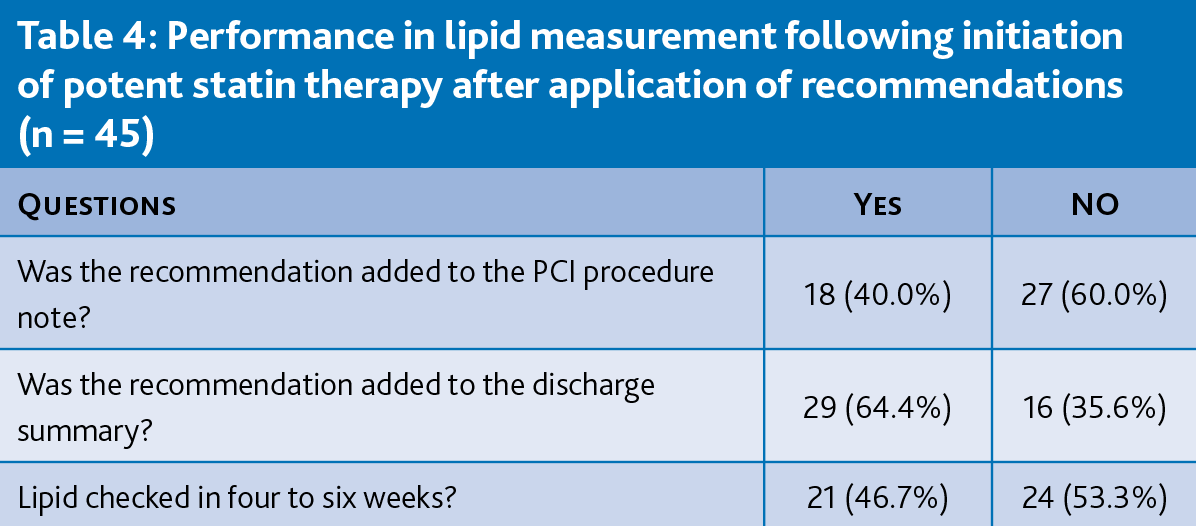
Guideline recommendations were added to the PCI procedure note for 40% of patients, while 60% did not have this addition. In the discharge summary, recommendations were included for 64.4% of patients, and omitted for 35.6%. Regarding lipid profile checks within four to six weeks post discharge, 53% did not undergo the check, while 46.7% did (see Table 4). Notably, only 13.3% of patients without a lipid profile evaluation by their doctor had a discharge report containing guideline recommendations.
(click to enlarge)
A summary of lipid measurement performance before and after implementing the recommendations showed improvements in some areas, such as reporting in the discharge summary and checking lipids in four to six weeks. However, there was still a lack of adherence to recommendations, particularly in the written procedure of treatment.
Conclusion
This audit’s findings indicate that the action plan enhanced the effectiveness of the lipid profile follow-up after discharge. Although it is extremely obvious that the primary care doctor followed the discharge summary’s recommendations, a tiny number of patients were unable to see their GP because of lengthy waiting lists.
Efforts should be made to strengthen the documentation in the discharge summary since despite this progress, there is still much that needs to be done to ensure that the recommendations are followed.
Alhmoud EN, Barazi R, Fahmi A, Abdu A, Higazy A, ElHajj M. Critical appraisal of the clinical practice guidelines for managing Dyslipidaemias: Lipid modification to reduce cardiovascular risk: European Society of Cardiology (ESC) and European Atherosclerosis Society (ESC/EAS) 2019 guidelines. Journal of Pharmaceutical Health Services Research, 2020; 11(4): 423-427. https://doi.org/10.1111/jphs.12371
Cho KH, Han X, Ahn JH, Hyun DY, Kim MC, Sim DS, KAMIR-NIH Investigators. Long-term outcomes of patients with late presentation of ST-segment elevation myocardial infarction. Journal of the American College of Cardiology, 2021; 77(15): 1859-1870
Claessen BE, Guedeney P, Gibson CM, Angiolillo DJ, Cao D, Lepor N, Mehran R. Lipid management in patients presenting with acute coronary syndromes: A review. Journal of the American Heart Association, 2020; 9(24). https://doi.org/10.1161/jaha.120.018897
Collet J, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Siontis GC. 2020 ESC guidelines for managing acute coronary syndromes in patients presenting without persistent ST-segment elevation. Revista Española de Cardiología (English Edition), 2021; 74(6): 544. https://doi.org/10.1016/j.rec.2021.05.002
Klassen A, Sussulini A, Derogis P, Ferreira C, Lopes A, Cruz E, Fonseca F. Evaluation of two highly effective lipid-lowering therapies in subjects with acute myocardial infarction: A Lipidomic analysis. 2021 https://doi.org/10.21203/rs.3.rs-154365/v1
Ibanez B, James S, Agewall S., et al. 2017 ESC guidelines for managing acute myocardial infarction in patients presenting with ST-segment elevation. Kardiologia Polska, 2018; 76(2): 229-313. https://doi.org/10.5603/kp.2018.0041
Ohm J, Hjemdahl P, Skoglund PH, et al. Lipid levels achieved after a first myocardial infarction and recurrent atherosclerotic cardiovascular disease prediction. International Journal of Cardiology, 2019; 296: 1-7. https://doi.org/10.1016/j.ijcard.2019.07.001
Zhao Q, Zhang T, Cheng Y, Ma Y, Xu Y, Yang J, Zhou Y. Impacts of the triglyceride-glucose index on the prognosis of patients with type 2 diabetes mellitus and non-ST-segment elevation acute coronary syndrome: Results from an observational cohort study in China. Cardiovascular Diabetology, 2020; 19(1). https://doi.org/10.1186/s12933-020-01086-5
 (click to enlarge)
(click to enlarge)