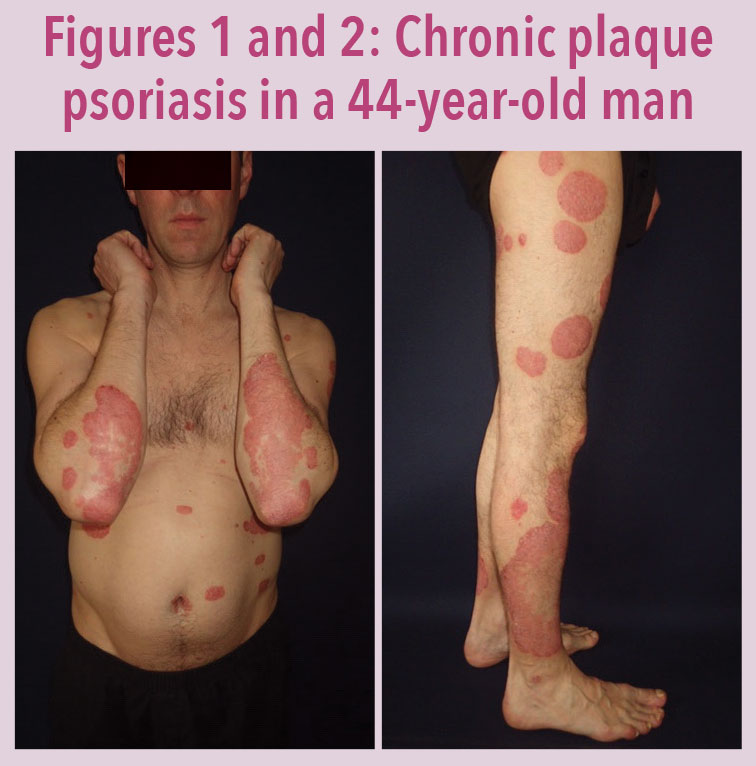
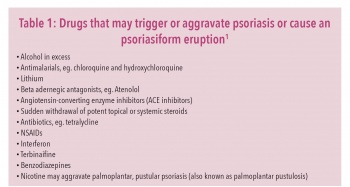
Psoriasis is a common, chronic, skin condition that usually presents as scaly plaques in the elbows, knees or scalp. However, psoriasis can affect any part of the body. It affects about 2% of the population and approximately 50% of patients with psoriasis will have another family member who is affected as there is a strong hereditary component. There may also be environmental triggers such as streptococcal throat infections and medication such as lithium, beta blockers, antimalarials or sudden stopping of oral or potent topical steroids (see Table 1).1
(click to enlarge)
In many cases, psoriasis can begin with no obvious trigger. Chronic plaque psoriasis most commonly occurs in adults with two peaks: one in the late teens and the second in patients in their fifties. Some patients have very mild psoriasis that is barely visible while others can have extensive psoriasis covering large areas of their body. Psoriasis can also affect the face, genitalia, nails and joints. Treatment will depend on the severity of the disease, the location and the age of the patient.
(click to enlarge)
Many patients with mild psoriasis may choose to ignore it which is perfectly acceptable as they often learn to live with the disease. It is important to assess the patient’s ideas, concerns and expectations with regard to their psoriasis. Some patients with even mild psoriasis may be very upset with their perceived unsightly appearance of the rash and may have unrealistic concerns or expectations regarding treatment.
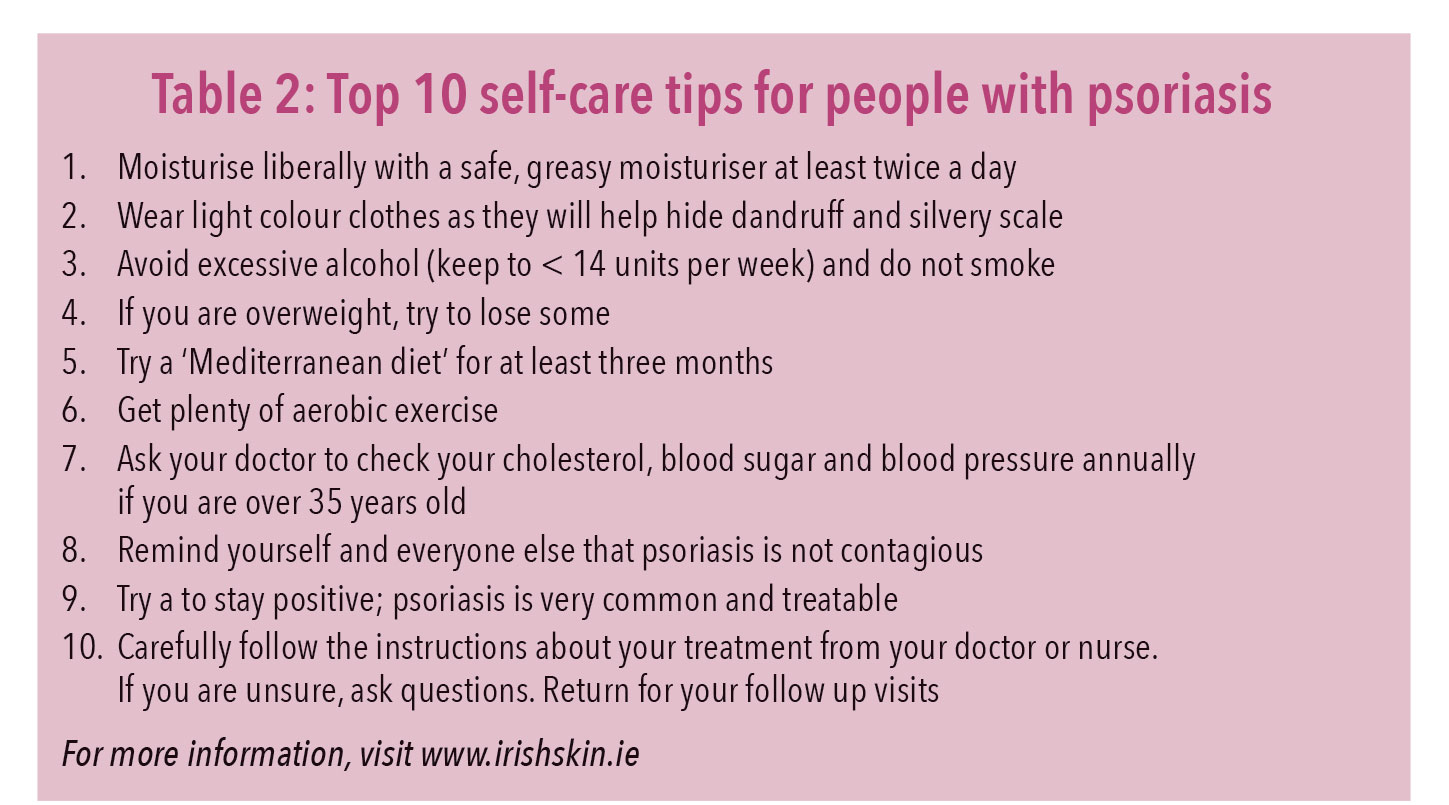
Many patients with mild psoriasis can manage their own disease by moisturising with a good greasy moisturiser such as emulsifying ointment or Epaderm ointment which should be rubbed downwards, twice a day, on the affected areas. These moisturisers are very greasy but are very effective at reducing the silvery scale that makes psoriasis so obvious (see Table 2).
(click to enlarge)
Psoriasis can often affect the scalp and can be linked with underlying dandruff or seborrhoeic dermatitis. A good dandruff shampoo such as Head & Shoulders, Nizoral or Stieprox may help to control the underlying dandruff and improve the psoriasis affecting the scalp. These should be used regularly at least three times a week and should be left to soak into the scalp for a few minutes before rinsing out. Patients with psoriasis on their scalp should avoid wearing dark clothes as these will make the dandruff more visible.
For more resistant scalp psoriasis in adults Etrivex shampoo may help but the treatment should not normally be used for more than one month. It contains a super potent topical steroid (clobetasol propionate) which is also found in Dermovate.
Most patients with chronic plaque psoriasis will improve with sunlight. However, 10% may get worse in the sun. For those who improve in the sun, natural sunlight is probably best but they should avoid getting sunburnt as this may make their psoriasis worse as a result of the Köbner phenomenon. Artificial sunlight from sunbeds should be avoided as these are predominantly UVA and can sometimes aggravate psoriasis. Some patients with severe extensive psoriasis may benefit from phototherapy in hospital dermatologist outpatients using narrow-band UVB or PUVA phototherapy.
Psoriasis is a chronic, inflammatory condition which increases the risks of developing the metabolic syndrome as a result of chronic, subclinical vascular inflammation which results in arteriosclerosis. This increases the overall risk of cardiovascular disease and type 2 diabetes. Patients with the metabolic syndrome are at two to four-fold increased risk of stroke, a three to four-fold increased risk of myocardial infarction and a two-fold increased risk of dying from such an event when compared to those without the syndrome, regardless of previous history of cardiovascular events.2 Treatment of the metabolic syndrome is lifestyle modification including weight loss, low sugar, low-fat diet and more aerobic exercise.
Psoriasis is not caused by food allergy. However, rare cases have been linked with coeliac disease and it may be worth considering a gluten-free diet in patients with positive coeliac antibodies or a positive family history of coeliac disease.3 A healthy diet rich in oily fish, green leafy vegetables, carrots, tomatoes and fresh fruit may help.4 Recent studies have suggested that a Mediterranean diet may also help psoriasis.5
Alcohol in excess is well-known to aggravate psoriasis so patients should be encouraged to keep their alcohol intake to a minimum and certainly not to exceed the recommended limits of 14 units per week.
Depression is more prevalent in people with psoriasis. Patients with severe psoriasis are more than three times more likely to suffer depression compared to controls.6 Treatment of the psoriasis may help the patient’s mood. Patients with psoriasis and depression may need counselling or medication to control their depression while they are trying to improve their psoriasis using various treatments. Stress reduction techniques, meditation and exercise may help their mood.
Patients need to know how to use the various medical treatments for psoriasis. The most common treatment for chorionic plaque psoriasis affecting the body is either Dovobet gel or Enstilar foam. Both of these products contain the same ingredients which is betamethasone (a potent topical steroid) and calcipotriol (a vitamin D analogue). The foam preparation seems to be more cosmetically acceptable and more effective than the gel formulation, which is easier to use on the scalp.7
The advantages of Dovobet and Enstilar are that they are relatively quick to improve the appearance of the psoriasis plaques and can be used in a convenient once a day application which usually does not burn, sting or stain the skin. The disadvantages are that they are expensive and do not work on all patients with psoriasis. They cannot be used on the face and they are not licensed for people under the age of 18 years old. The maximum dose of Dovobet in adults is 15g a day or 100g a week for acute management of psoriasis in the first month of treatment and it should not be used on more that 30% of body surface area. It should be applied once daily for the first two to four weeks and then gradually reduced to alternate days or twice a week as the psoriasis improves. Enstilar Cutaneous Foam can be applied up to 15g per day (0.5g covers the equivalent of an adult hand; 0.5g corresponds to the amount administered from the can if the actuator is fully depressed for two seconds). If the psoriases affects 12% of the body surface area (1% BSA is equivalent to the size of the palm of the hand), an adult patient would need 6g a day or three cans over a month.
Dovobet and Enstilar contain potent topical steroids that may cause skin atrophy which can look like partially treated psoriasis and there may be systemic absorption with adrenal suppression particularly if high doses are used. A rebound flare of psoriasis can occur if these potent steroid combinations are stopped suddenly. If possible, the patient should be slowly weaned off Dovobet gel or Enstilar foam and onto Dovonex cream which contains only calcipotrol but no steroid. This can be used daily and indefinitely until the psoriasis is fully cleared or improved to an acceptable level.
Dovobet and Enstilar are safe and effective but will only work in up to 60 to 70% of patients with chronic stable plaque psoriasis. They are not suitable for children. In these cases, dithranol is extremely safe and effective, although more messy and time consuming to use. Dithranol contains anthralin which is a chemical of plant origin taken from the bark of a South American tree. Short contact treatment using a preparation called Dithrocream is the most convenient way to use dithranol for home treatment. The weakest strength (0.1%) is applied for 30 minutes daily for one week to the plaques on the body and scalp but not on the face or genitalia. If the psoriasis does not clear and the Dithrocream does not burn the skin, patients should increase to the next strength. There are five strengths, so it takes five weeks to get up to the maximum strength of 2%. Up to 90% of patients will clear their psoriasis with this treatment but it causes considerable brown staining of the skin which may take a few weeks to fade once the treatment is stopped. It may also cause burning of the skin and if this happens the patient has to stop the treatment and go back to their previous strength.
The patient needs careful instructions about how to safely use these topical agents and the advice should be supported with written information that they can take home. This should help with improving compliance and reducing the risk of side effects.
Psoriasis on the face and flexures is usually less thick and scaly than other parts of the body and will often respond to 1% hydrocortisone ointment. More resistant psoriasis on the face or flexures may respond to tacrolimus (Protopic), although this ointment is not licensed for this indication.
More extensive, severe or resistant forms of psoriasis will probably have to be referred to hospital for phototherapy or systemic treatments such as methotrexate, fumaric acid or some of the new biological agents.8
References
Kim GK, Del Rosso JQ. Drug Provoked Psoriasis: Is it drug induced or drug aggravated? Understanding pathophysiology and clinical relevance. Journal of Clinical and Aesthetic Dermatology 3(1):32-8.Jan 2010
Kaur J. A Comprehensive Review on Metabolic Syndrome. Cardiology Research and Practice. 2014;2014:943162. doi:10.1155/2014/943162
Wolters M. Diet and psoriasis: experimental data and clinical evidence. Br J Dermatol. 2005 Oct;153(4):706-14
NALDI L . Dietary factors and the risk of psoriasis. Results of an Italian case–control study. British Journal of Dermatology. Volume 134, Issue 1, pages 101–106, January 1996
Phan C, Touvier M, Kesse-Guyot E, et al. Association Between Mediterranean Anti-inflammatory Dietary Profile and Severity of Psoriasis Results From the NutriNet-Santé Cohort. JAMA Dermatol. Published online July 25, 2018. doi:10.1001/jamadermatol.2018.2127
Kurd SK, et al. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010 Aug;146(8):891-5. doi: 10.1001/archdermatol.2010.186
Koo J, et al. Superior efficacy of calcipotriene and betamethasone dipropionate aerosol foam versus ointment in patients with psoriasis vulgaris – A randomized phase II study. J Dermatolog Treat 2016;27:120–7
Laws PM, Young HS. Update of the management of chronic psoriasis: new approaches and emerging treatment options. Clinical, cosmetic and investigational dermatology : CCID. 2010;3:25-37
 (click to enlarge)
(click to enlarge)