Rapid tranquillisation: prescribing practice of junior doctors in a general hospital setting
A study on the preferred medication regimen for rapid tranquillisation among NCHDs in a general hospital
Dr Julianne Reidy, Consultant Psychiatrist, Waterford Regional Hospital, Waterford and Dr Kizito Otuokpaikhian, Registrar in Adult Psychiatry, Clare Mental Health Services, Ennis, Co Clare
Acute behavioural disturbance can occur in the general hospital setting and may require the use of medication for rapid tranquillisation. This survey aims to examine the views of non-consultant hospital doctors (NCHDs) working in a general hospital regarding their preferred medication regimen for rapid tranquillisation. Questionnaires that explored prescribing practice were sent to 51 NCHDs. The majority of NCHDs would use an antipsychotic and/or a benzodiazepine. Haloperidol was the sole antipsychotic chosen. Diazepam was the benzodiazepine most chosen for the oral route and midazolam for the parenteral route. A majority of respondents identified adverse respiratory and cardiac effects as potential problems. Knowledge of remedial measures for adverse side-effects was limited.
In practice, an antipsychotic and/or a benzodiazepine is effective and frequently used for rapid tranquillisation. More education is required regarding the potential adverse effects of antipsychotics and benzodiazepines and potential remedial measures.
Introduction
Acute behavioural disturbance can occur in the general hospital setting, both in emergency departments (EDs) and on general hospital wards. It may occur in a number of different contexts including physical illness, psychiatric illness, substance misuse or personality disorder. Guidelines for managing disturbed/violent behaviour place a strong emphasis on anticipating and de-escalating aggressive behaviour.1,2 However, when non-pharmacological strategies have been ineffective, emergency drug treatment may be required.
Rapid tranquillisation (RT) is defined as the use of medication to calm an aggressive or agitated patient.3 It is an acute measure to address aggressive or violent behaviour when psychological and behavioural methods have failed. In psychiatric care, it is one of the most common types of emergency medication.4 Despite this, there is a lack of high-quality clinical trial evidence in the area.1,5 Much of the existing evidence base relies on naturalistic studies and case series.6 Some recent high-quality studies have been carried out in developing countries,7,8 however it is not yet clear whether the results of these trials are applicable in other contexts.5 There are guidelines on the subject, generally based on consensus opinion and clinical experience.1,2,6,9,10 Many existing guidelines are due to be reviewed1,9,10 and do not include more recent evidence.
In terms of choice of medication there is no “gold standard” medication regimen.5,6 This is evident in practice. A survey in a London hospital found that eight different drugs were used in 102 episodes of emergency treatment.11 There are no recent Irish studies in the area. Most guidelines and studies in the area also relate to psychiatric settings rather than the general hospital setting. The authors wished to examine the views of NCHDs working in a general hospital regarding their preferred medication regimen for RT.
Method
A questionnaire was sent to 51 NCHDs working in a general hospital with 307 beds. Paediatric, anaesthetic and psychiatric NCHDs were excluded as they are not responsible for the immediate management of adult patients on the general hospital wards or in the ED. In the questionnaire, RT was defined as the use of medication where other approaches have failed to de-escalate acutely disturbed behaviour and there is an immediate risk of potential harm to the patient or others.
The questionnaire consisted of six open-text questions. The first two questions requested information regarding the preferred choice and dose of oral and parenteral medications for RT. The respondents were asked what changes they would make to these choices if the patient was over the age of 65 years. The next question sought information on what physical monitoring the person would carry out following RT. The final questions addressed potential adverse effects and remedial measures which could be used.
Results
Twenty-three (45%) of the questionnaires were completed and returned. Six (26%) were completed by interns, six (26%) by registrars, 10 (43%) by senior house officers and one (4%) by a specialist registrar.
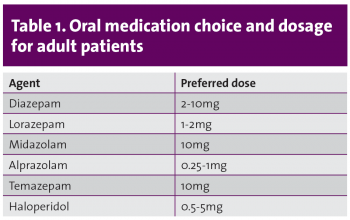
Oral medication chosen and dose range
An antipsychotic and/or a benzodiazepine (BZD) were the oral medications most commonly chosen. A BZD was more likely to be used (n = 11; 48%) than an antipsychotic (n = 5; 22%) and some respondents (n = 7; 30%) considered both. Thirty-four per cent of the NCHDs did not state the preferred dose. Haloperidol was the antipsychotic of preference, with a dose range of 0.5-5mg. The most common BZD chosen was diazepam (n = 8; 38%), followed by lorazepam (n = 6; 29%), midazolam (n = 3; 14%), alprazolam (n = 3; 14%) and temazepam (n = 1; 5%). Some respondents chose more than one BZD. The dose ranges chosen are outlined in Table 1.
(click to enlarge)
Parenteral medication chosen and dose range
A BZD was more commonly chosen (n = 11; 48%) than an antipsychotic (n = 7; 30%); 13% (n = 3) considered both. One respondent did not give a parenteral choice and intravenous morphine was chosen by another. A BZD was chosen 18 times – midazolam was the preferred BZD (n = 7; 39%), followed by diazepam (n = 6; 33%) and lorazepam (n = 5; 28%). The dose ranges chosen are outlined in Table 2.
Two of the respondents who would use a BZD did not give a dose. Seventeen per cent (n = 4) would consider giving BZD intravenously. Haloperidol was again the sole antipsychotic of choice. The dose range chosen was between 0.25mg and 10mg. Thirty per cent (n = 3) of respondents who chose haloperidol did not state the dose they would use.
(click to enlarge)
Changes if older than 65 years
Most respondents 74% (n = 17) stated they would use lower doses of the medication if the patient was 65 years of age or older, 17%, (n = 4) specified that they would use half of the adult dose. Four (17%) of the NCHDs stated they did not know what changes to make if the patient was over 65 years and one reported that they would look up the prescribing guidelines.
Physical monitoring
The majority of the respondents (87%; n=20) reported they would monitor the patient’s vital signs following RT. However, one of the NCHDs reported they would keep the patient comfortable and advise bed rest. Twenty-one per cent (n = 5) would also carry out neurological observations. Only one of the respondents specified monitoring the temperature of the patient.
Adverse effects
Respiratory depression (n = 15; 65%) was the most common adverse effect that respondents anticipated following the administration of RT. Thirty per cent (n = 7) were concerned about cardiovascular complications. Extrapyramidal side-effects (EPSEs) and over-sedation were also identified as adverse effects of concern following RT by 22% of respondents. Acute dystonic reaction was specifically mentioned by two of the respondents. Other potential adverse effects reported included dependency, paradoxical reaction and anaphylactic drug reaction (see Figure 1).
(click to enlarge)
Remedial measures for adverse reaction
Eight respondents (34%) stated that they did not know what remedial measure to implement if there was an adverse reaction. General supportive measures (IV fluids, administration of oxygen) were considered by 34% (n = 8) of respondents. Six respondents (26%) stated they would administer flumazenil for BZD toxicity and 4% (n = 1) would consider using an anticholinergic for acute dystonia.
Discussion
Traditionally, first-generation antipsychotics and BZDs have been the drugs most frequently used for rapid tranquillisation.1,3,5,6,9,10,12 It is therefore not surprising that the majority of NCHDs in this study chose to use haloperidol and/or a BZD.
Over 50% of NCHDs would use a BZD alone for both oral and parenteral RT. This is appropriate in a general hospital setting where patients may have comorbid medical illness and the risks of using antipsychotic medication may be greater in terms of cardiovascular and other side-effects. Respiratory depression must be considered, however, and 65% of respondents identified this risk. BZDs also have the advantage of having a specific antagonist (flumazenil).
Antipsychotics may also be used alone for RT. In this study 30% of respondents would use haloperidol alone if using parenteral medication for RT. This may be appropriate if there is a history of recent BZD or alcohol misuse or tolerance or where BZDs have previously been ineffective.1,6,11
Thirteen per cent (n = 3) of respondents would use haloperidol in combination with a BZD for parenteral route and 30% (n = 7) will consider an oral combination of haloperidol with a BZD. This approach minimises the dose of the antipsychotic required.1 It may also be more effective than a BZD alone for severe behavioural disturbance.6
Haloperidol was the sole antipsychotic chosen for both oral and parenteral routes. It is an effective agent for RT and there is significant experience in its use.12 The Maudsley guidelines, however, have suggested that it be the last drug considered as a consequence of the higher incidence of EPSEs and dystonic side-effects. A pre-treatment ECG is also recommended,14 which may not be practical in a very agitated patient.
There are alternatives to haloperidol including olanzapine, quetiapine, risperidone and aripiprazole.2 Olanzapine and aripiprazole are also available in formulations for intramuscular (IM) administration in RT. Some studies have suggested than IM olanzapine is more effective than IM haloperidol, however the behavioural disturbances in these studies were modest.13 A disadvantage compared to other agents is that it cannot be given concurrently with a parenteral BZD. Experience with IM aripiprazole is limited as it is a relatively new agent.6
In terms of choices of BZD the most commonly chosen BZDs were diazepam for the oral route and midazolam for the parenteral route. It is more common to use lorazepam both orally and intramuscularly.1 The choices made may reflect the BZDs with which non-psychiatric doctors are most familiar.
Seventeen per cent (n = 4) would use the intravenous route, however this is the most hazardous route and its use should be limited.1,3 It is concerning that one individual also considered the use of intravenous morphine, although it is not clear what context they had in mind. An agent which was not mentioned was promethazine, an antihistamine which is gaining evidence as an alternative to BZD.7,8
For older patients, most of the NCHDs stated they would reduce the doses of the medications. This is reassuring as older adults are more sensitive to adverse effects of medicines and generally respond to lower doses due to pharmacokinetic changes with increasing age. Only 17% (n = 4) specified using half the dose, which is the general recommendation.2 This needs to be judged on a case-by-case basis, however, with regard to the older patient’s age, comorbid physical problems and level of frailty.
Regarding monitoring, most respondents appropriately suggested they would monitor vital signs. This may include respiratory rate, blood pressure, oxygen saturation, pulse rate and temperature. It would also be advisable to perform an ECG and haematological monitoring.2 In terms of adverse effects most of the NCHDs were concerned about respiratory and cardiovascular adverse effects. Fewer numbers were aware of the EPSEs. Studies8 have suggested that 6% of patients who receive haloperidol develop an acute dystonic reaction.
However, only a small number of respondents indicated EPSEs as a potential side-effect and even fewer numbers for acute dystonia. Consequently, some of the respondents were unsure of the remedial measures for EPSEs. Overall the level of knowledge regarding remedial measures was poor, with 34% reporting that they were unsure regarding remedial measures. This may reflect the unavailability of established local guidelines.
It is recommended that anyone administering RT should be familiar with the adverse effects of the medicines used and how to manage them.1
Conclusion
The choices made by NCHDs were generally appropriate and within licensed dosages. However, the choices of agents could be improved. Lorazepam should be the BZD of choice, orally or intramuscularly; it has the advantage of a short half-life and is available for both oral and parenteral use.1,3
If an antipsychotic is also required a second-generation could be considered, particularly for the oral route. There is also a need for increased knowledge and familiarity about possible adverse reactions and remedial measures.
In the absence of high-quality studies in this area the availability of guidelines is helpful to those making decisions regarding individual patients. Local guidelines are currently being developed, which, in addition to assisting in the choice, dose and route of administration of specific agent(s), will also give information regarding recommended monitoring and remedial measures. These guidelines will be introduced as part of a teaching programme for NCHDs.
Declaration of interest: none.
References
National Institute for Health and Clinical Excellence. Violence: The short-term management of disturbed/violent behaviour in in-patient psychiatric settings and emergency departments. 2005 (www.nice.org.uk/pdf/cg025niceguideline.pdf)
Maudsley Prescribing Guidelines (10th edition). The South London and Maudsley/Oxleas NHS Foundation Trusts
Macpherson R, Dix R, Morgan S. A growing evidence base for management guidelines. Revisiting guidelines for the management of acutely disturbed psychiatric patients. Adv Psychiatr Treat 2005; 11: 404-415
Ellison et al. Emergency treatment of acute psychosis, agitation and anxiety. Hosp Comm Psych 1985; 36: 351-352
Pratt JP, Chandler-Oatts J, Nelstrop L et al. Establishing gold standard approaches to rapid tranquillisation: A review and discussion of the evidence on the safety and efficacy of medications currently used. J Psychiatr Intensive Care 2008; 4: 43-57
Parker C, Khwaja MG. What is new in rapid tranquillisation? J Psychiatr Intensive Care 2011; 7: 91-101
Raveendran NS, Tharyan P, Alexander J, Adams CE; and the TREC-India II Collaborative Group. Rapid tranquillisation in psychiatric emergency settings in India: pragmatic randomised controlled trial of intramuscular olanzapine versus intramuscular haloperidol plus promethazine. BMJ 2007 (doi: 10.1136/bmj.39341.608519.BE)
Huf G, Coutinho ESF, Adams CE; TREC Collaborative Group. Rapid tranquillisation of violent or agitated people in psychiatric emergency settings: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol plus promethazine. BMJ 2007 (doi: 10.1136/bmj.39339.448819.AE)
Royal College of Psychiatrists. Strategies for the Management of Disturbed and Violent Patients in Psychiatric Units. Royal College of Psychiatrists, Council Report CR41, 1995
Royal College of Psychiatrists. Management of Imminent Violence: Clinical Practice Guidelines to Support Mental Health Services. Occasional Paper OP41, 1998
Pilowsky LS, Ring H, Shine P J. Rapid tranquillisation. A survey of emergency prescribing in a general psychiatric hospital. Br J Psychiatry 1992; 160: 831-835
Brenda wood. Clinically significant acute agitation. Consensus update US Pharm 2010; 35(11): HS-9-HS-15
L San, B Arranz, I Querejeta, S Barrio. A naturalistic multicentre study of intramuscular olanzapine in the treatment of acutely agitated manic or schizophrenic patients. Eurpsych 2006; 21(8): 539-543
Janssen-Cilag Ltd. Summary of product characteristics. Haloperidol injection. 2009 (hppt.//emc.medicines.org.uk)
 (click to enlarge)
(click to enlarge)

