New ESC guidelines will hopefully lead to improvements in the treatment of ACS, as well as promoting research to further improve outcomes
Prof Robert Byrne, Director of Cardiology, Mater Private Network, Chair of Cardiovascular Research, RCSI and Dr JJ Coughlan, Consultant Cardiologist, Mater Private Network, Dublin
The 2023 European Society of Cardiology (ESC) Guidelines for the management of acute coronary syndromes (ACS) combined the two previously separate non-ST elevation ACS (NSTEACS) and ST elevation myocardial infarction (STEMI) guidelines into one document for the first time (escardio.org/Guidelines). This was intended to highlight that all of ACS can be considered as a clinical spectrum.
The concept of the ‘ACS spectrum’ encompasses clinical presentation, electrocardiogram (ECG) findings and cardiac biomarker levels. The underlying pathophysiology for the majority of ACS is thought to be unstable plaque, most commonly plaque rupture or erosion. The diagnosis of myocardial infarction is based on the fourth universal definition of MI. This requires elevation of cardiac biomarkers, with high sensitivity cardiac troponin (hs-cTn) the recommended biomarker to use. Unstable angina (UA) is also a subtype of ACS and is not associated with elevated cardiac biomarkers. It is defined clinically as myocardial ischaemia at rest or on minimal exertion in the absence of acute cardiomyocyte injury/necrosis. It is characterised by specific clinical findings of prolonged (> 20 min) angina at rest; new onset of severe angina; angina that is increasing in frequency, longer in duration, or lower in threshold; or angina that occurs after a recent episode of MI.
This article highlights some of the key concepts in the 2023 ACS guidelines.
Initial assessment
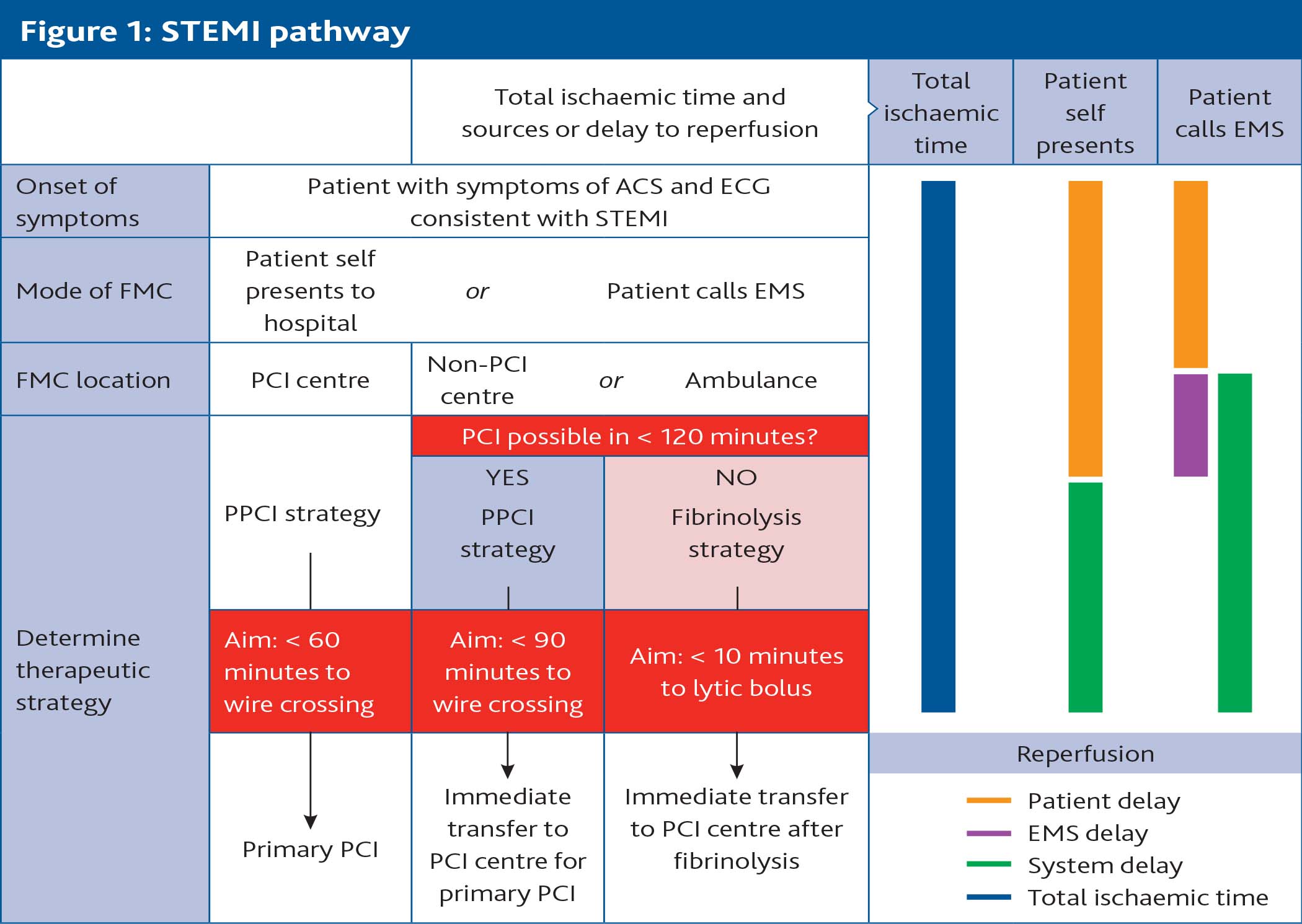
If a patient is suspected to be presenting with ACS, early recognition and risk stratification is key to appropriate management. The 2023 guideline highlights this with the ACS assessment, which is intended to summarise the most important components of the initial assessment of a patient presenting with a suspected ACS. This involves performing an ECG to assess for electrocardiographic evidence of ischaemia (this should be performed within 10 minutes of first medical contact), considering the clinical context of the patient’s presentation (including symptoms, the results of any other available investigations and the clinical background) and performing a focused clinical examination to assess if the patient is clinically stable. It is important to note that cardiac biomarkers do not play a role in this assessment. This is because there will inevitably be a delay associated with waiting for analysis of these tests and many of the initial treatment decisions for patients with ACS are time dependent (ie. transfer for primary percutaneous coronary intervention [PPCI]).
(click to enlarge)
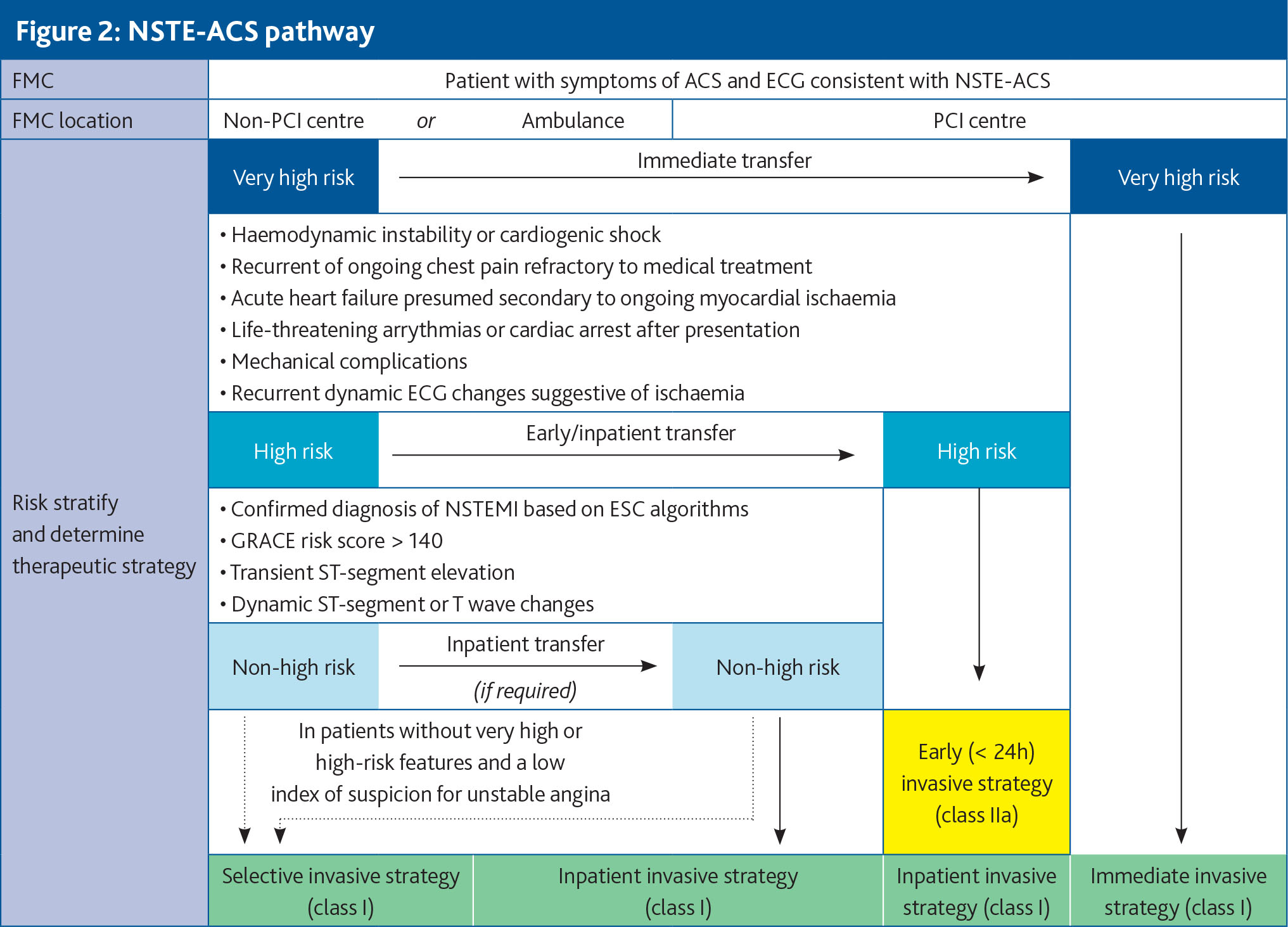
Based on the ACS assessment, it should be possible to stratify the patient into one of two treatment pathways, the STEMI pathway or the NSTE-ACS pathway (see Figures 1 and 2). As can be seen in these figures, the majority of patients with STEMI and NSTE-ACS are recommended to undergo invasive coronary angiography (ICA). ICA allows for delineation of the coronary anatomy and is considered central to the ACS treatment paradigm. The majority of these patients will eventually be treated with PCI, with a smaller proportion of patients undergoing coronary artery bypass grafting (CABG). Some patients may require medical management alone.
(click to enlarge)
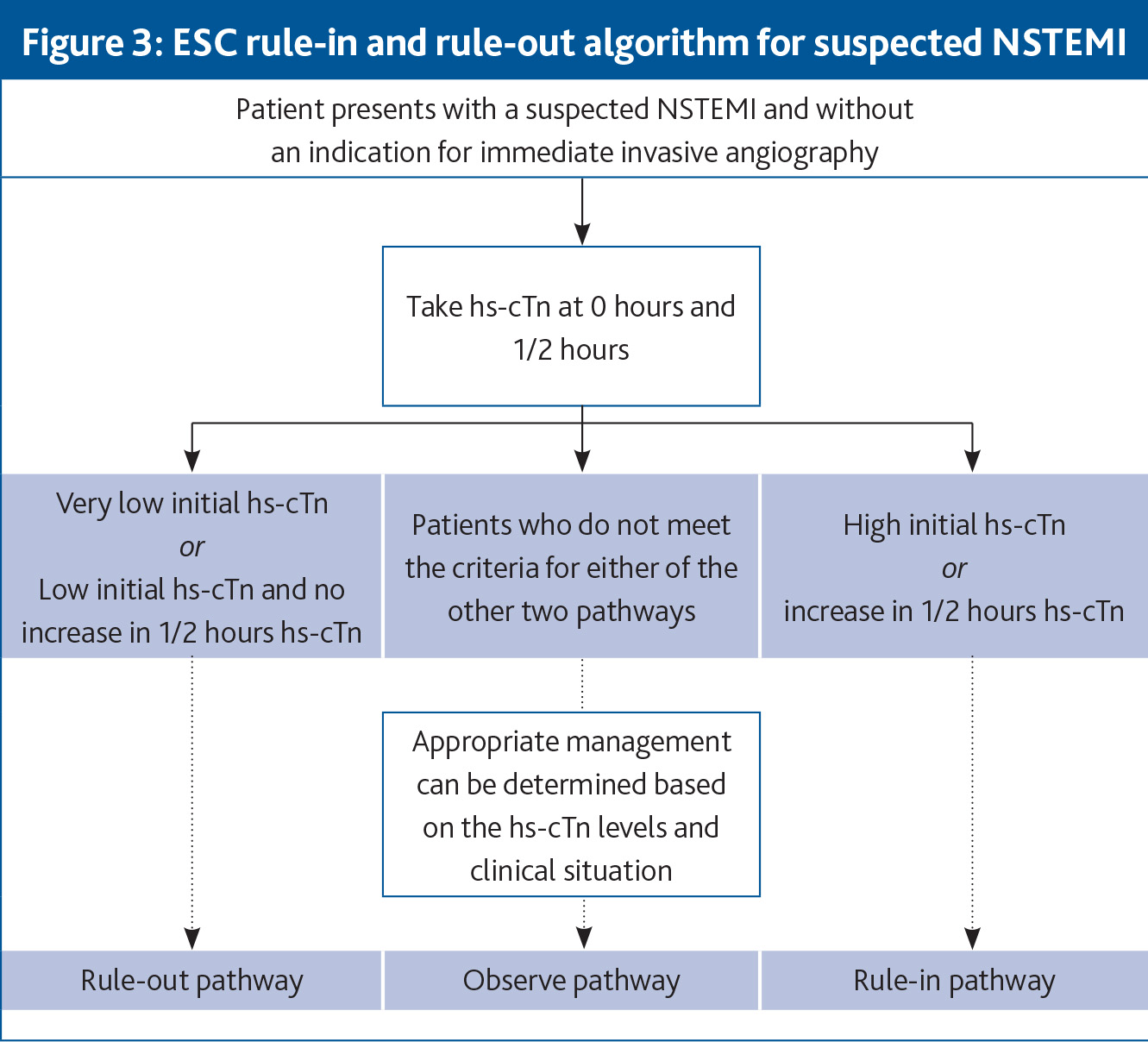
For patients who are not presenting with STEMI or NSTE-ACS with an indication for immediate ICA, it is recommend to use an algorithmic approach to rule in or rule out NSTEMI. This is highlighted in Figure 3.
(click to enlarge)
Antithrombotic therapy
Regardless of the ACS subtype, the general recommendations for antithrombotic therapy (ATT) are similar. All patients with ACS should be treated initially with parenteral anticoagulation and antiplatelet therapy.
Dual antiplatelet therapy (DAPT), consisting of aspirin and a P2Y12 receptor inhibitor, for 12 months is recommended as the default regimen for patients with a confirmed ACS diagnosis. This DAPT duration may be abbreviated if patients are felt to be at high bleeding risk (HBR).
Longer-term treatment
Patients with ACS require long term medical treatment to reduce their risk of future cardiovascular events. An important concept in the guideline is that the prevention of the next event starts at the time of ACS diagnosis.
All patients should be discharged on cardioprotective medications, with information on lifestyle management and a referral to cardiac rehabilitation. A follow-up outpatient appointment should also be arranged. The treatment goals at outpatient follow up should be to support healthy lifestyle choices, to promote adherence to and persistence with pharmacological cardioprotective therapies, and to reach and sustain risk factor treatment targets. Key treatment targets include a BP of < 130mmHg systolic and < 80mmHg diastolic, a low density lipoprotein cholesterol (LDL-C) of < 1.4mmol/L, and, for diabetic patients, a HbA1c of < 53mmol/L. Lipid lowering therapy is particularly important for ACS patients and it is recommended to follow an algorithmic approach, with stepwise addition of lipid lowering agents until treatment goals are met.
Patients with cancer
A section on patients with ACS and cancer was included for the first time in this guideline. This was intended to highlight that there are an increasing number of patients presenting with ACS who either have a history of cancer or are being actively treated for cancer. Cancer and atherosclerotic cardiovascular disease share many common risk factors and given that survival from most cancers is improving, it is natural that this is a more commonly encountered clinical situation. In general, patients with a history of cancer should be treated the same as any other patient with ACS. For patients undergoing active treatment for cancer, interruption of cancer therapies suspected to be contributing to the ACS presentation is recommended. All these patients should be managed in a multi-disciplinary fashion, with input from their relevant specialist teams.
Patient perspectives
Another new section in this guideline is the patient perspectives section. This was compiled with valuable input from a patient representative on the task force panel and is intended to highlight that the care of ACS patients should not only reflect the best scientific evidence, but should also try to promote care that is respectful of, and responsive to, the individual patient’s preferences, needs and values.
Patients who are regarded as equal partners in their ACS medical management are recognised to be more likely to engage and participate in their own healthcare. The guidelines stress the importance of shared decision-making, informed consent and patient education.
Sex differences in ACS
There are currently no data suggesting that men and women with ACS should be treated differently. However, several studies have observed that women presenting with ACS are often treated differently to men. This includes being less likely to undergo ICA, to receive timely revascularisation, to be prescribed evidence based medications and to be referred to cardiac rehabilitation. These findings suggest a potential gender bias in the management of patients with ACS.
It may also be relevant that women with ACS tend to be older than men and therefore, these findings may also reflect some degree of age bias. All healthcare providers should be conscious of this potential gender bias in the management of patients with ACS and strive to ensure that all patients receive evidence based, guideline recommended care.
Conclusions
The 2023 ESC guidelines for ACS provide a comprehensive overview of the management of patients across the entire ACS spectrum, from patients presenting with unstable angina to patients presenting with STEMI in cardiogenic shock. The guideline provides an evidence based framework to guide healthcare professionals in providing high quality care to these patients.
While the clinical severity of the ACS presentation may vary, the underlying principles of management remain the same. Recommendations are provided for the entire patient journey, from initial assessment and emergent management, through to discharge and the longer term prevention of recurrent events. It is our hope that this guideline will lead to improvements in the care of patients with ACS, as well as promoting more scientific research to further improve clinical outcomes.
 (click to enlarge)
(click to enlarge)