Cardiovascular disease (CVD) is at endemic levels worldwide and is currently the leading cause of death among both men and women. Heart attacks in women account for one-third of deaths globally.1 In this modern age of medicine, women have worse outcomes and a higher mortality risk than men. This multifactorial issue stems from late diagnoses, less aggressive treatment of cardiac risk factors and poor referral rates to cardiac rehabilitation (CR) programmes.2
CR is deemed a class 1A recommendation for the secondary prevention of CVD.3 The early ambulation of post-MI patients in the 1960s has developed into a comprehensive programme to improve cardiovascular function through exercise and risk factor management.4 Yet, it is a significantly underutilised resource, particularly among women. Evidence suggests that only 20-50% of eligible patients participate in CR, with the percentage of female participation being much lower.5
This article aims to address the misconceptions about female CVD risk and explore the benefits of CR for women. It will also identify the barriers to female CR participation and completion. Only by understanding the root cause of this gender disparity in CR can we move beyond the barriers to find real-life solutions.
The enigma of female CVD
It is estimated that 75-90% of CVD is attributed to cardiac risk factor exposure.6 Risk factors include diabetes, physical inactivity, diet, hypertension, smoking, obesity and psychological stress.3,4 Both men and women are vulnerable to risk factor exposure, but women are rarely treated with the same aggressive therapies.2,7 Practitioners frequently misdiagnose women due to the complexity of female pathophysiology.
The beneficial effects of oestrogen as a cardioprotector are well documented. In younger years, women have higher high-density lipoprotein (HDL) cholesterol levels than men.7-10 However, most acute cardiovascular events occur in women with normal low-density lipoprotein (LDL) cholesterol levels.7 Due to these normal LDL levels, many women do not qualify for statin therapy on standard male-orientated guidelines.7,9 Despite this, there has been significant improvement in cardiovascular health outcomes with the use of simvastatin for LDL levels less than 100mg/dL.9,10
One Swedish cohort study that followed up with female patients after 17 years identified the total cholesterol-to -HDL ratio as a formidable predictor of acute myocardial infarction (AMI) in women. However, a gender-specific tool has yet to be developed globally.11
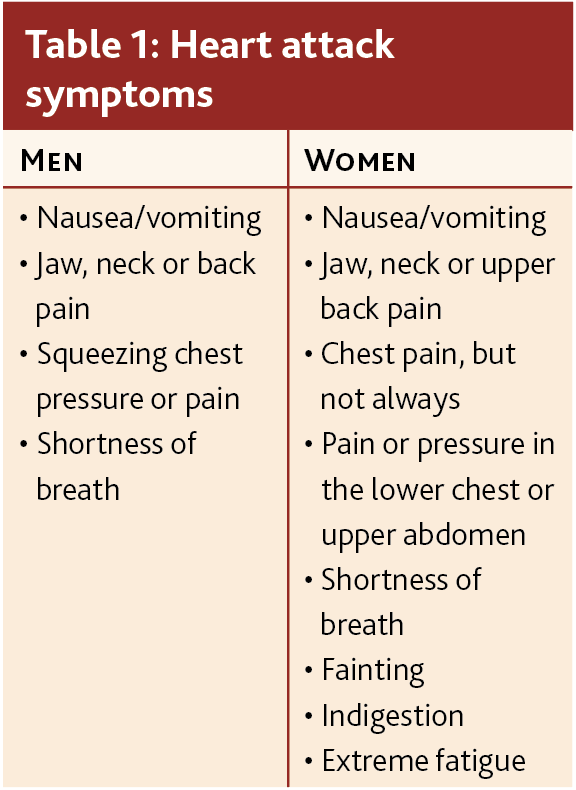
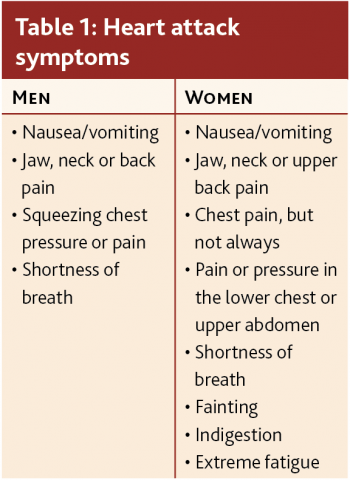
Once women reach menopause, the cardioprotection of oestrogen erodes.7 Menopausal transitioning is a time of accelerated CVD risk for women, as depleting oestrogen levels adversely affect the distribution of body fat, vascular health and lipid profiles. Treating women with hormone replacement therapy can have beneficial effects on cholesterol; however, it does not prevent CVD from occurring.12 During this period, women often experience vague symptoms of CVD and do not identify with textbook male symptoms (see Table 1), which can often delay the diagnosis of CVD by practitioners.2,13 Coupled with less aggressive treatment plans, when women are referred to CR, they are older with multiple comorbidities, musculo-skeletal disorders, decreased functional capacity and worse exercise tolerance than men.14
(click to enlarge)
Benefits of cardiac rehabilitation for women
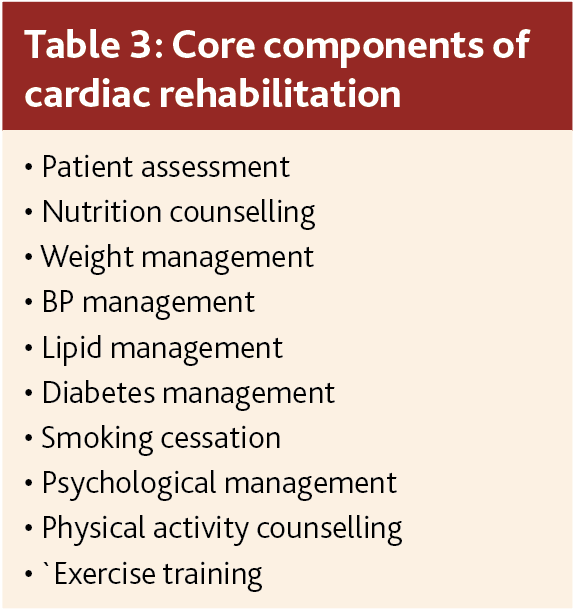
The European Society of Cardiology defines cardiac rehabilitation as “a comprehensive, multifactorial intervention recommended in international guidelines to patients with cardiovascular disease”. It consists of “patient assessment, physical activity counselling, exercise training, diet/nutritional counselling, risk factor control, patient education, psychosocial management, vocational advice, and lifestyle behaviour change”.15
Although the aetiology and treatment of male and female CVD differ significantly, CR benefits men and women alike.3 A well-conducted cohort analysis of 73,000 patients found a relative reduction rate in mortality of 58% at one year and 21- 34% at five years, with older women gaining the most benefit.16 Due to the undertreatment of risk factors in women,4 CR provides the opportunity to alter these risk factors systematically. The completion of the programme resulted in greater functional capacity in women.7,13
Physical improvement
In terms of physical improvement, women can increase their aerobic capacity parallel with their male cohort despite entering CR programmes with reduced fitness levels.17 Appropriate exercise therapy also provides crucial education and guidance for those who may have yet to implement it into their daily routine.18
Psychological improvement
Perhaps the most beneficial aspect of CR for women is a psychological improvement. Social deprivation for women has superseded traditional cardiac risk factors in the past decade.7 Analysis of these risk factors in the 2004 INTERHEART study19 showed that psychosocial stress was twice as common in women than men and was a significant predictor of the risk of MI.2
After a cardiovascular event, compared with men, women often leave hospitals and appointments with feelings of confusion as they find it more difficult to question physicians and advocate for their health.2,7 In this sense, CR is an invaluable therapeutic tool in providing a safe space for women in similar circumstances to develop meaningful relationships. This, in turn, supports positive and open dialogue about their cardiovascular health with qualified professionals.7,19
Barriers to female participation in cardiac rehabilitation
Physician referrals
Although women may be in greater need of secondary prevention therapy, they are significantly less likely than men to access it.14 Many primary providers assign a lower risk to female patients, which enables this gender barrier. This risk-treatment paradox has been well-documented for more than a decade.14 Studies have shown that participation levels increase when physicians endorse CR and encourage their female patients to enrol.7 Yet the most significant obstacle in their participation is poor physician referral rates in eligible patients.20
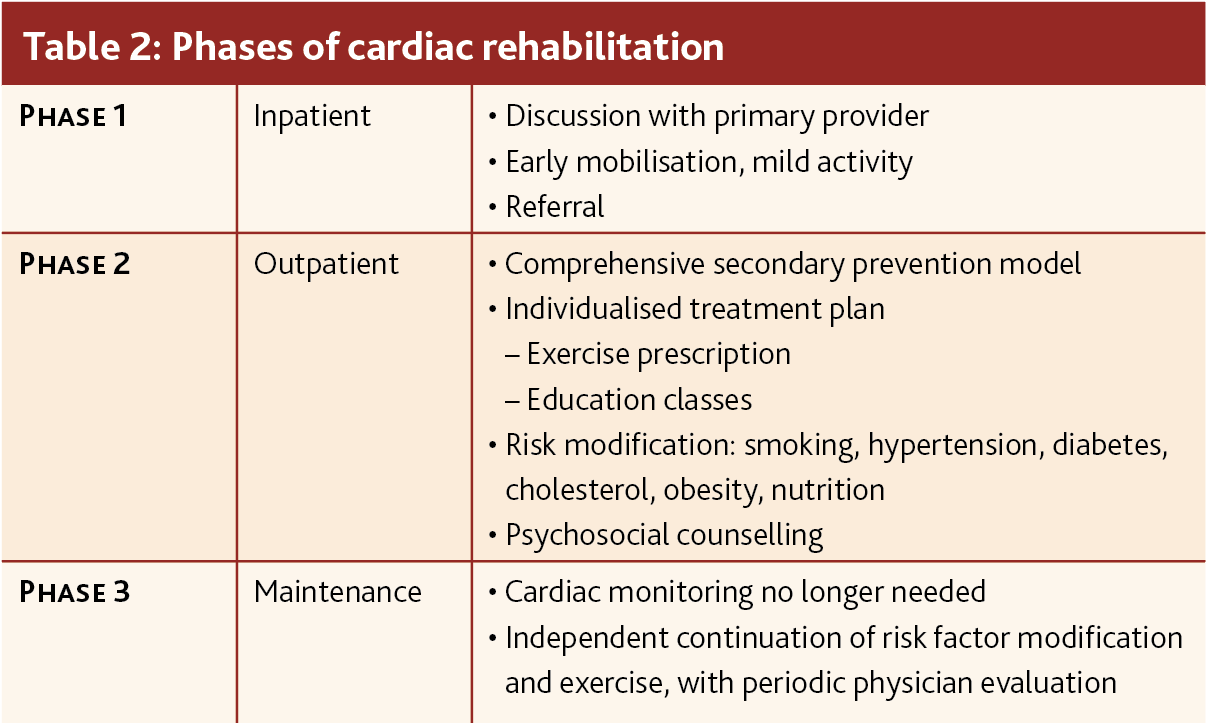
Traditionally, CR is divided into three phases. These consist of inpatient, outpatient and independent maintenance (see Table 2).15,18 Physician referral should ideally occur in phase 1 to optimise CR uptake. However, due to the complexities of inpatient and discharge management, physicians often omit this referral. Patients, particularly women, are therefore discharged without a meaningful insight into the benefits of attending CR. Women patients often find it increasingly more challenging to self-advocate than their male cohort.2,3
Once female patients are referred to CR, however, they are statistically more likely to have lower levels of participation and higher drop-out rates than men.14 This is due to increased comorbidities, depression, transportation issues, economic burden and less exercise tolerance than men.17,20
(click to enlarge)
Exercise
In comparison to men, women are less likely to have an exercise routine incorporated into their daily lives.7 Many women may perceive exercise as tiring and painful, particularly those suffering from musculoskeletal issues.21 Increasing cardiovascular fitness is one of the main objectives of modern CR programmes. VO2 peak measures the maximum amount of oxygen the body can utilise during exercise. It is considered the gold standard for measuring cardiovascular fitness.22 Generally, sex differences exist in VO2 peak and become more apparent with age.17,21 CR programmes with higher intensity exercises are more beneficial in increasing VO2 peak on completion. Although advantageous, high-intensity exercise programmes can alienate women. Women often experience pain, fitness insecurity and exertional discomfort.21 Finding the ideal exercise balance is paramount in recruiting and retaining women in CR programmes while improving their cardiovascular fitness.
Socio-economic barriers
Historically, women have always been of lower socio-economic status globally. In Ireland, the 2017 risk of poverty rate for women was 16.5% compared to 14.7% for men.23 Regarding finances, women face conflicting priorities, which leaves them unable to allocate restricted financial resources to attend CR programmes. Female patients often dismiss CR, with priority given to caregiving responsibilities and work.7 However, data from European CR programmes suggest that once referred, patients are more likely to complete CR when financial assistance is provided.4 Transportation issues and costs are also indicators of poor CR attendance.14,17 Due to female longevity, older women depend more on adult children for transportation but are reluctant to burden them with this request.14,17
Overcoming obstacles
Bridging the gender gap in CR participation is essential for the future treatment of female cardiovascular health. Globally, CVD is the leading cause of death for women, yet the disparity of treatment options is abundantly clear. Perhaps the root cause of this inequality lies in clinicians’ misunderstanding of female CVD risk. Improving physician understanding and assessment of female CVD risk is crucial.
Standardised referral process
A lack of referral to CR programmes is one of the most modifiable factors. Implementing a standardised referral process for CR has the capacity for the most significant impact.4 Automated referral processes would exponentially increase the enrolment of women in CR programmes. One study found that automated referral increased enrolment from 32% to 70%, with females being 6.5 to 10 times more likely to be referred to CR.21 Another suggestion was the requirement of physicians to document why there was an absence of a referral, which would be beneficial in addressing the shortcomings.3,7
Female-focused cardiac rehab programmes
A 2022 systematic review and meta-analysis13 of women-focused CR programmes found that such models improved quality of life and reduced morbidity. Another study found that female-only exercise programmes improved cardiovascular fitness and women’s overall perception of their health. It also recorded improvements in systolic blood pressure and lipid profile.21 While social deprivation for women has superseded traditional cardiac risk factors in recent years,7 women-focused CR programmes offer a social outlet where women can feel supported by their peers.25
Hybrid models
Given society’s increasing dependence on technology, digital health initiatives are quickly emerging as encouraging alternatives to traditional in-person CR programmes. With improved accessibility for patients and reduced costs for health services, the benefits are substantial.3 In 2017, a randomised control trial of a digital health initiative (DHI) versus a standard in-person CR programme found significant improvements in weight loss in the DHI cohort.24 It also reported a reduced number of hospitalisations and ED presentations. This DHI was a smartphone-based model where patients self-reported their dietary and exercise habits. This model provided educational information on healthy lifestyles that patients could access in their own free time.24 This trial’s findings suggest using a hybrid CR model for optimal results.
The American Heart Association has also highlighted the importance of combining new digital models with existing in-person CR programmes, instead of replacing them.4 A hybrid system of CR has the potential to address the barriers that women often face, such as financial and transportation issues and family responsibilities.21
Intensive cardiac rehabilitation
Intensive cardiac rehabilitation (ICR) is a form of CR that includes “comprehensive non-exercise components such as stress management, peer support and diet modification”.25 A retrospective cohort study of 15,613 patients in the US identified the effectiveness of ICR in addressing female-specific concerns.25 In this study, the percentage of male and female programme completion was similar. With mounting evidence suggesting female drop-out rates are much higher than men,5 this study speculates that the ratio of exercise to non-exercise components in ICR aided in women’s completion of the programme. For the completers, women also achieved better quality of life and depression reduction.25 As psychological distress is known to profoundly impact female cardiovascular health,14 these findings are promising for women’s CR outcomes.
(click to enlarge)
Conclusion
Cardiac rehabilitation is a class 1A recommendation for the secondary prevention of CVD.3 It is a significantly under-utilised resource worldwide, especially in female patients with higher morbidity and mortality levels after CVD diagnosis.1 Gender disparity runs deep throughout the 3-phase process. The barriers to women accessing and completing CR are rooted in the misconceptions of female CVD risk, poor physician referral rates, non-female-orientated CR programmes and socio-economic concerns.
Although improvements have been made in the past decade, it is important that future studies and trials include larger numbers of female participation. Implementing research-based recommendations will address the failings of healthcare systems globally. These include standardised referral processes, female-orientated CR programmes and hybrid digital and in-person models. Now is the time to bridge the gender gap in cardiovascular health to ensure that future generations of women have better health outcomes.
References
Mehran R, Vogel B, Ortega R, Cooney R, Horton R. The Lancet Commission on women and cardiovascular disease: time for a shift in women’s health. The Lancet. 2019 Mar;393(10175):967–8.
Aggarwal NR, Patel HN, Mehta LS, et al. Sex Differences in Ischemic Heart Disease. Circulation: Cardiovascular Quality and Outcomes. 2018 Feb;11(2)
Simon M, Korn K, Cho L, Blackburn GG, Raymond C. Cardiac rehabilitation: A class 1 recommendation. Cleveland Clinic Journal of Medicine. 2018 Jul;85(7):551–8
Sandesara PB, Lambert CT, Gordon NF, et al. Cardiac Rehabilitation and Risk Reduction. Journal of the American College of Cardiology [Internet]. 2015 Feb [cited 2019 Jul 10];65(4):389–95. Available from: https://reader.elsevier.com/reader/
Forsyth F, Deaton C. Women and cardiac rehabilitation: Moving beyond barriers to solutions? European Journal of Preventive Cardiology. 2020 Mar 26;28(7):758–60
Dhingra R, Vasan RS. Age As a Risk Factor. Medical Clinics of North America [Internet]. 2012 Jan;96(1):87–91. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3297980/
Daniels KM, Arena R, Lavie CJ, Forman DE. Cardiac Rehabilitation for Women across the Lifespan. The American Journal of Medicine. 2012 Sep;125(9):937.e1–7. Available from: https://www.sciencedirect.com/science/article/pii/S0002934311010357
Maas AHEM, Appelman YEA. Gender differences in coronary heart disease. Netherlands heart journal: monthly journal of the Netherlands Society of Cardiology and the Netherlands Heart Foundation [Internet]. 2010;18(12):598–602. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3018605/
Sharma J, McAlister J, Aggarwal NR, et al. Evaluation and management of blood lipids through a woman’s life cycle. American Journal of Preventive Cardiology. 2022 Jun 1
Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the Management of dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. European Heart Journal [Internet]. 2019 Aug 31;41(1). Available from: https://academic.oup.com/eurheartj/article/41/1/111/5556353
Calling S, Johansson SE, Wolff M, Sundquist J, Sundquist K. The ratio of total cholesterol to high density lipoprotein cholesterol and myocardial infarction in Women’s health in the Lund area (WHILA): a 17-year follow-up cohort study. BMC Cardiovascular Disorders. 2019 Oct 29;19(1)
El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation [Internet]. 2020 Nov 30;142(25)
Mamataz T, Ghisi GL, Pakosh M, Grace SL. Outcomes and cost of women-focused cardiac rehabilitation: A systematic review and meta-analysis. Maturitas. 2022 Jun;160:32–60
Oosenbrug E, Marinho RP, Zhang J, et al. Sex Differences in Cardiac Rehabilitation Adherence: A Meta-analysis. Canadian Journal of Cardiology. 2016 Nov;32(11):1316–24
Bäck M, Hansen TB. ESC Prevention of CVD Programme: Rehabilitation. Escardio.org. 2017
Suaya JA, Stason WB, Ades PA, Normand SLT, Shepard DS. Cardiac Rehabilitation and Survival in Older Coronary Patients. Journal of the American College of Cardiology. 2009 Jun;54(1):25–33
Menezes AR, Lavie CJ, Milani RV, Forman DE, King M, Williams MA. Cardiac Rehabilitation in the United States. Progress in Cardiovascular Diseases. 2014 Mar;56(5):522–9
Mampuya WM. Cardiac rehabilitation past, present and future: an overview. Cardiovascular diagnosis and therapy [Internet]. 2012;2(1):38–49. Available from: https://www.ncbi.nlm.nih.gov/pubmed/24282695
Yusuf S, Hawken S, Ôunpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. The Lancet. 2004 Sep;364(9438):937–52
Jones CA, Valle M, Manring S. Using survival analysis to explore female cardiac rehabilitation program adherence. Applied Nursing Research. 2001 Nov;14(4):179–86
Smith JR, Thomas RJ, Bonikowske AR, Hammer SM, Olson TP. Sex Differences in Cardiac Rehabilitation Outcomes. Circulation Research. 2022 Feb 18;130(4):552–65
Ross R, Blair SN, Arena R, et al. Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign: A Scientific Statement From the American Heart Association. Circulation. 2016 Dec 13;134(24)
Poverty, Peace and Justice - CSO - Central Statistics Office [Internet]. www.cso.ie
Widmer RJ, Allison TG, Lennon R, Lopez-Jimenez F, Lerman LO, Lerman A. Digital health intervention during cardiac rehabilitation: A randomized controlled trial. American Heart Journal. 2017 Jun;188:65–72
 (click to enlarge)
(click to enlarge)