A case of being on the ‘wrong’ side of the doctor-patient divide
An interesting case of a doctor who ignored his symptoms of worsening fatigue and weight loss for almost a year, blaming his hectic lifestyle
Dr Zulfiqar Ali Sandhu, AMAU Staff Physician, Wexford General Hospital, Wexford, Dr Melika Hamouda, Medical SHO, Wexford General Hospital, Wexford and Prof Obada Yousif, Consultant Endocrinologist, Wexford General Hospital, Wexford
A 40-year-old surgical colleague presented to the acute medical assessment unit (AMAU) with vague symptoms of progressively worsening fatigue and weight loss. He admitted unintentional weight loss of approximately 20kg over a space of one year. He was working as an emergency department SHO when the symptoms started. He attributed his weight loss to a heavy workload, shift work and a hectic lifestyle. Due to these symptoms he moved to a different specialty, ie. surgery. However, the symptoms did not improve and in fact continued to progress. He is a smoker with no past medical history of note.
He had a complete workup for the investigations of unintentional weight loss. His thyroid functions showed secondary hypothyroid picture with a low TSH and T3. His hormone profile showed low cortisol and testosterone levels with a normal prolactin.
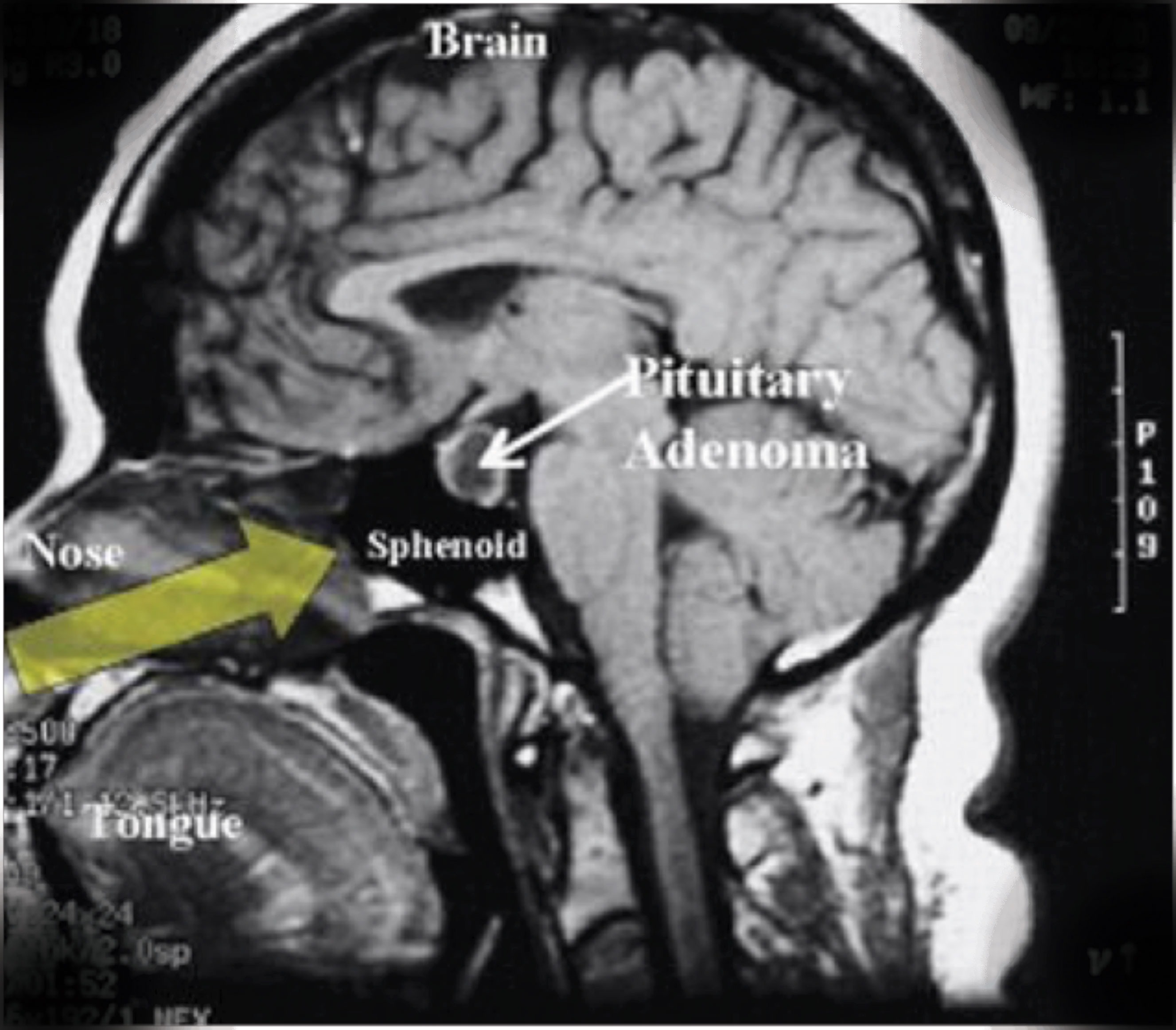
The panhypopituitarism picture prompted MRI pituitary and formal assessment of visual fields by ophthalmology colleagues. The MRI reported a large pituitary mass measuring 24mm by 23mm with significant suprastellar extension, intra-lesional haemorrhage and expansion consistent with pituitary apoplexy. The visual field assessment confirmed the suspicion of bi-temporal haemianopia.
He was urgently transferred to the neurosurgical unit and had trans-sphenoidal hypophysectomy with a good outcome. He is currently on eltroxin and hydrocortisone and is doing well.
(click to enlarge)
Discussion
A pituitary gland, also known as hypophysis, weighs approximately 0.5g and in humans is the size of a pea. It sits on hypophysial fossa of sphenoid bone and is surrounded by the sella turcica.1,2 Deficiency of one or more hormones of the pituitary gland is called hypopituitarism. The pituitary gland has three lobes:
Anterior lobe, which secretes six hormones including gonadotropin, follicle stimulating hormone, growth hormone, luteinising hormone, adrenocorticotropic hormones, thyroid stimulating hormone and prolactin
Posterior lobe, which secretes two hormones – oxytocin and antidiuretic hormone, which are produced in the supra-optic and paraventricular nuclei of the hypothalamus and then transported via the pituitary stalk to be stored and released from the posterior lobe3
Intermediate lobe, which produces and secretes melanocyte stimulating hormone, which is avascular and mostly absent in human beings.4
Pituitary gland disorder may produce pituitary disease with over or under production of hormones. Over production of growth hormone can cause acromegaly;adrenocorticotropic hormone can cause Cushing’s disease; vasopressin can cause syndrome of inappropriate antidiuretic hormone; and under production of growth hormone can cause growth hormone deficiency. In addition, vasopressin can cause diabetes insipidus hypopituitarism.5
The most common tumour in the pituitary gland is pituitary adenoma, which are the third most common intracranial tumour, accounting for approximately 10% of all intracranial tumours.6,7 These adenomas are divided into benign adenoma, invasive adenoma and carcinoma. Most adenomas are benign, 35% are invasive and 0.1% to 0.2% are carcinomas. The estimated prevalence rate in the general population is approximately 17%.
Pituitary gland injury or damage can occur slowly or be of sudden onset, mild or severe. Pituitary damage can affect either one or all hormones. The clinical picture and presentation will depend on the number of hormones involved. If one of the pituitary hormones is deficient then it is called partial hypopituitarism and it is not very common when compared to deficiency of all pituitary hormones, which is called panhypopituitarism.8,9
Patients may present with various symptoms, including fatigue, weakness, dizziness, nausea, vomiting, hypotension, hypoglycaemia, anorexia, weight loss, weight gain, constipation, hair loss, dry skin, bradycardia, loss of libido, osteoporosis, decreased muscle mass, premature atherosclerosis, inability to breastfeed, polyuria, polydipsia and nocturia, depending on the hormones involvement.10 The treatment strategy for a pituitary adenoma is hypophysectomy followed by hormone replacement if required.
Doctors as patients
Faced with the prospect of an illness, the doctor’s objectivity often crumbles. Some reach for a diagnoses at the first hint of illness; many more ignore or downplay their health problems.
The reasons for the failure of many doctors to seek appropriate and timely help are multifactorial.
This has now been recognised by different medical associations, including the Royal College of Physicians of Ireland. Various courses and seminar have been introduced on physician health, including one specially designed for trainee doctors called Wellness Matters.
Self-care is now considered a core competency by the Royal College of Physicians and Surgeons of Canada, as physicians are expected to “demonstrate a commitment to physician health and sustainable practice.”8,9
Likewise other medical associations have similar programmes in place, such as Norway’s Physicians for Physicians programme10 and doctors’ health and wellbeing by the British Medical Association.11
References
Gibo H, Hokama M, Kyoshima K, Kobayashi S. Arteries to the pituitary. Nippon Rinsho 1993; 51(10):2550-2554. PMID 8254920
Mancall EL, Brock DG, eds. Cranial Fossae in Gray’s Clinical Anatomy. Elsevier Health Sciences 2011; p 154. ISBN 9781437735802.
Higham CE, Johannsson G, Shalet SM. Lancet 2016, Nov 12; 388(10058):2403-2415 doi: 10.1016/S0140-6736(16)30053-8. Epub 2016, Mar 31
Melmed S. The Pituitary - (Third Edition). San Diego, CA 92101-4495, USA: Academic Press is an imprint of Elsevier, 2011; pp. 23-25. ISBN 978-0-12-380926-1
Overview of the Pituitary Gland: Pituitary Gland Disorders: Merck Manual Home Health Handbook. Retrieved 2009-04-04
Surawicz TS, McCarthy BJ, Kupelian V et al. Descriptive epidemiology of primary brain and CNS tumors: results from the Central Brain Tumor Registry of the United States, 1990-1994. Neuro Oncol 1999 Jan; 1(1):14-25
Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am 1999 Mar; 28(1):81-117
Prabhakar VK, Shalet SM. Aetiology, diagnosis, and management of hypopituitarism in adult life. Postgrad Med J 2006; 82:259-66. [PMC free article] [PubMed]
Jostel A, Lissett CA, Shalet MS. In: Hypopituitarism in Endocrinology. 5th ed. Degroot LJ, Jameson JL, editors. Philadelphia: Elsevier Saunders; 2006; pp. 397-409
van Aken MO, Lamberts SW. Diagnosis and treatment of hypopituitarism: an update. Pituitary 2005; 8:183-191
Royal College of Physicians and Surgeons of Canada. CanMEDS 2005 Physician Competency Framework. Accessed 5 September 2012. www.royalcollege.ca/portal/page/portal/rc/common/documents/canmeds/resou
Provincial Physician Health Programs. Canadian Medical Association. Acces-sed 5 September 2012. www.cma.ca/living/centrephysicianhealthwellbeing
Rosvold EO. Physicians in illness and health. An epidemiological study on health- and illness behaviour among 19th and 20th century Norwegian physicians. [Dissertation] University of Oslo, Oslo, Norway 2002. Accessed 20 June 2011. www.legeforeningen.no/asset/20570/1/ 20570_1.pdf
British Medical Association: Doctors health and wellbeing. Accessed 2012, Sept 7. http://bma.org.uk/practical-support-at-work/doctors-well-being
 (click to enlarge)
(click to enlarge)