A hidden trauma – concealed pregnancy in 21st century Ireland
An exploration of concealed pregnancy in modern Ireland
Ms Sylvia Murphy Tighe, Doctoral Midwifery Student, School of Nursing and Midwifery, Trinity College Dublin and Prof Joan Lalor, Associate Professor of Midwifery, School of Nursing and Midwifery, Trinity College Dublin
Concealed pregnancy as a social issue remains a contemporary problem in Ireland and internationally. It is a complex process which involves hiding a pregnancy and can lead to maternal or neonatal morbidity or mortality.1
Many still believe that women and young girls conceal their pregnancy because of the stigma related to pregnancy before marriage, but it is much more complex than that. Understanding why women conceal a pregnancy will help in offering responsive care to women and may have a positive impact on consequences such as birthing alone or neonatal abandonment. Concealed pregnancy is a complex phenomenon, where a woman is aware of her pregnancy and copes by keeping it secret and hidden.1
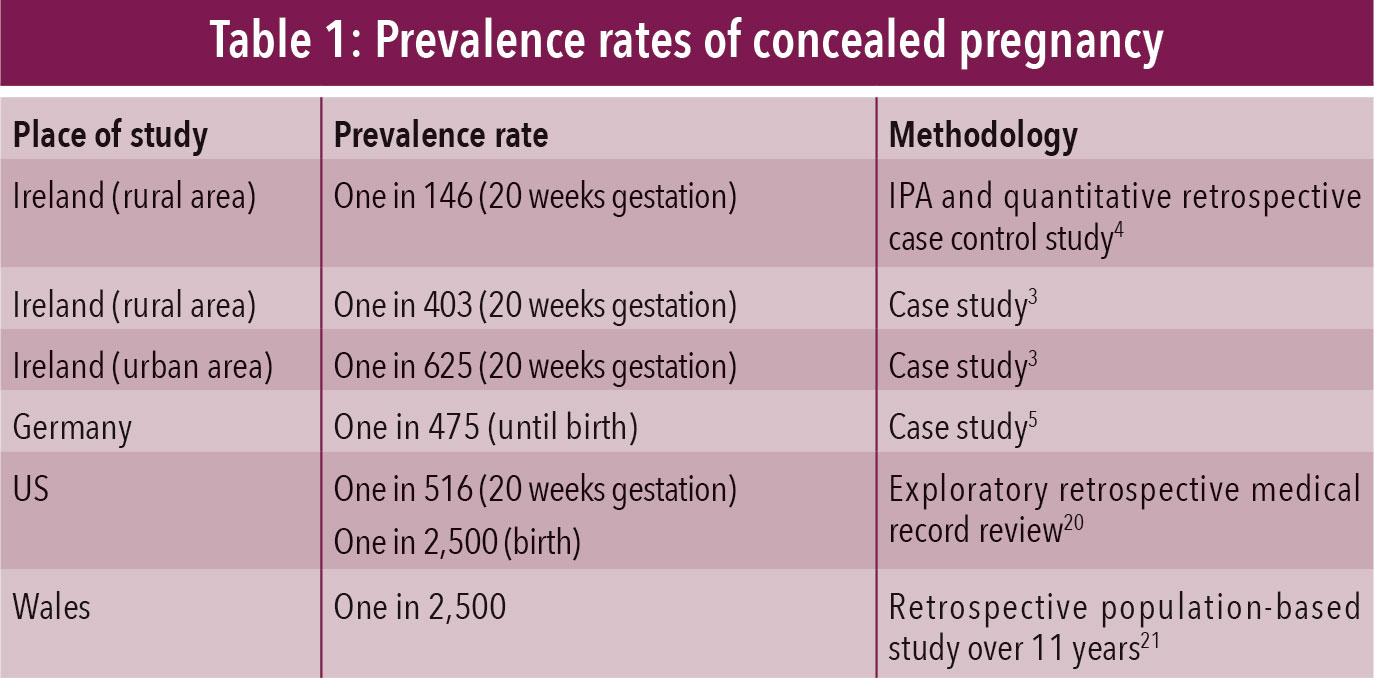
Prevalence rates of concealed pregnancy (see Table 1) are difficult to establish because of the nature of the phenomenon and the way in which countries collect population-based data. The Confidential Enquiry into Maternal Deaths2 and Serious Case Reviews of infant deaths in the UK have identified some of the risks of concealing a pregnancy, including unassisted birth, maternal death, neonatal death, newborn abandonment and neonaticide.1
(click to enlarge)
The Keeping it Secret (KISS) Study
Our research, funded by the Health Research Board, the Keeping it Secret (KISS) Study involved exploring the nature and impact of the experience of concealed pregnancy for women. We have interviewed 30 women up to three times who were concealing or had concealed a pregnancy in the past.
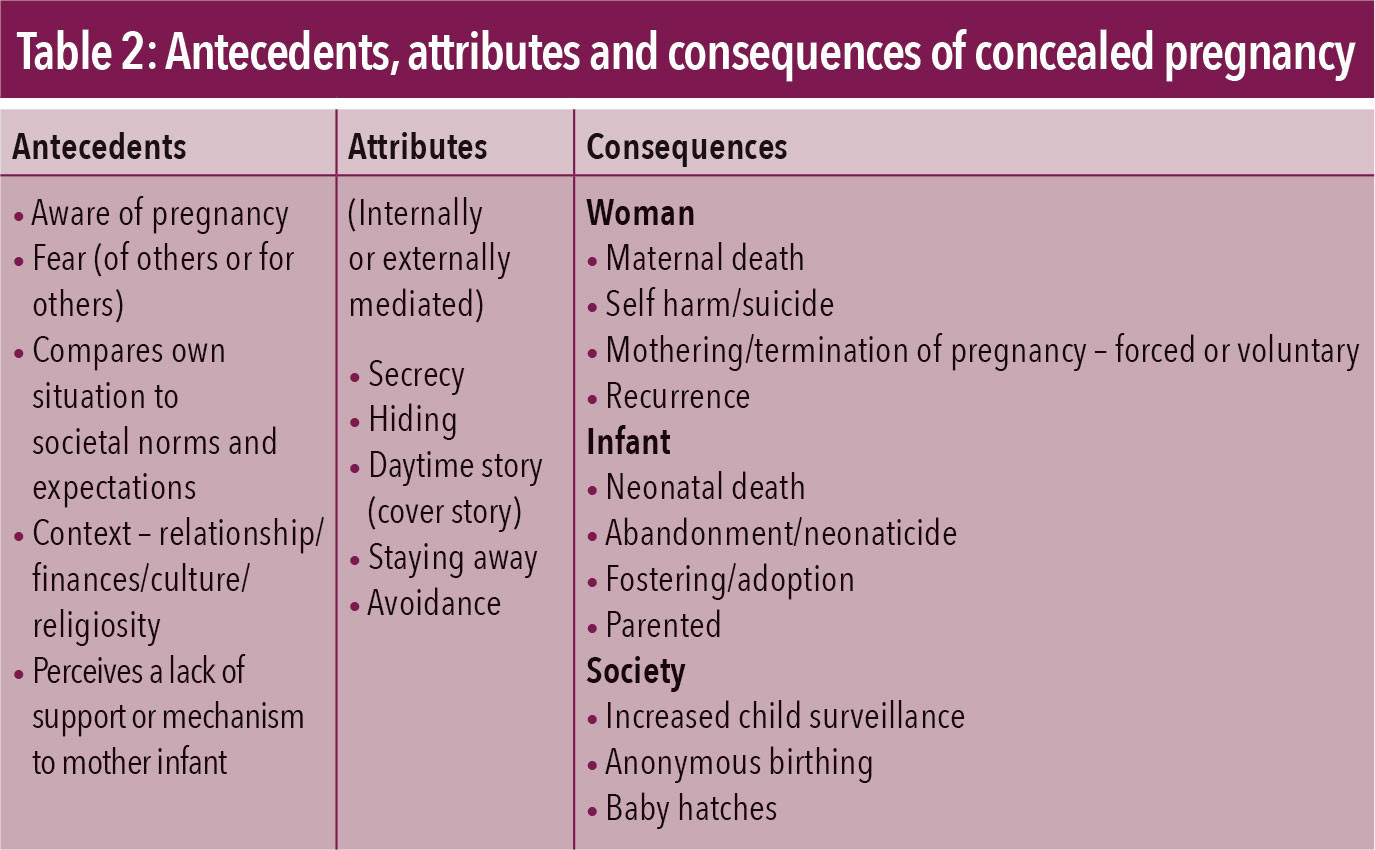
Definitional confusion around concealed pregnancy and what it is and is not is problematic.1,3,4,5 This ambiguity has hindered the development of responsive services to support women concealing a pregnancy and their choices. Consequently, one of the aims of the KISS study was to generate a new definition for concealed pregnancy and the characteristics of the process to assist understanding (see Table 2).
(click to enlarge)
Concealed pregnancy is a complex, multidimensional and temporal process where a woman is aware of her pregnancy and copes by keeping it secret and hidden. Behaviours such as avoidance, hiding, using a daytime story, staying away and secrecy are key characteristics of a concealed pregnancy. Fear (of others or for others) is central to the process and an interaction with another antecedent, eg. context/culture or a perceived lack of support to a mother and her infant, leads to concealing a pregnancy. It is a difficult and traumatic experience for the woman. Variations in the duration of concealed pregnancy exist and recurrence may feature in this process.1
The Ann Lovett and Kerry babies cases are perhaps the most publicly known examples of concealed pregnancy in Ireland. However, more recent incidences include a case in July 2013, when a newborn infant was found dead in Cork after being born in a toilet.6 The following year in 2014 the media reported on a newborn infant’s body that was found in a bin,7 and again recently a newborn infant’s body was found in Wicklow, likely abandoned after a concealed pregnancy. Last year, a newborn (baby Maria) was found on the roadside in Dublin.8 The media captured pleas made by a Garda and a social worker asking Maria’s mother to come forward, and although reassurances were given that the mother was not in trouble, this was at odds with images of Garda checkpoints searching for the mother seen on TV and in newspapers.
Lest we believe that this phenomenon is peculiar to Ireland, such cases have also occurred in Wales and Australia.1,9
In 2014 in Australia a newborn baby was found alive but hidden in a storm-drain,1 also following a concealed pregnancy. At the same time, a second case emerged which involved a young Irish backpacker in Australia who gave birth alone and then concealed the body of her stillborn baby.11 She revealed the situation to friends days later and was charged by police for concealing a birth. The response to charge this young woman with a criminal act and subsequently incarcerate her, demonstrates a serious lack of understanding of the process of concealing a pregnancy and will do little to encourage women who are distressed and traumatised by being pregnant to come forward to access help.
These tragic cases serve to highlight that concealed pregnancy remains problematic today. As a nation we might wish to forget our dark history of mother and baby homes, Magdalene laundries and forced adoptions.12,13,14,15 However, concealed pregnancy is real, is happening today and needs an effective response if we are to mitigate the worst possible outcomes.
Who conceals a pregnancy?
The notion that only young women and girls conceal pregnancy is a fallacy.1,2 Concealed pregnancy crosses many boundaries and in fact a woman may be in a relationship, married with children and financially secure. As pregnancy outside of marriage is now generally accepted, concealment is sometimes viewed as an abnormal response to a crisis pregnancy.
Although women who experience a concealed pregnancy report it is a distressing time where they often have no support,16 it is still the case that some authors approach this event as being related to a pathological disorder such as psychosis or mental ill health.17,18,19 The potential exists for women who conceal a pregnancy to become pathologised and stereotyped as mentally ill, despite little evidence to support this.1
Women have described the time when they were concealing a pregnancy as a bleak, desolate and lonely period in their lives.1,3 Women in the KISS study were fearful of the pregnancy becoming known and many sought antenatal care late in their pregnancy, if at all. One participant in the study said: “To this day, the official story I tell my family is that I did not know I was pregnant.” This woman was aware of her pregnancy but reported she felt disconnected, shut down and paralysed by fear. Another participant who hid her pregnancy said “my plan was to show up, have the baby, hand it over and walk away”, as she feared others would influence the outcome.
It must be recognised that women who experience a concealed pregnancy may have had no healthcare or support during their pregnancy, and some have had traumatic experiences in their lives such as domestic violence, child sexual abuse or a sexual assault.1 Contemporary society imposes expectations on pregnant women that discourages the expression of ambivalent or conflicted feelings. The silence and lack of discussion around conflicted feelings about a crisis pregnancy is problematic.1
Key learning points for midwifery and nursing practice
• Women can experience such intense levels of paralysing fear while concealing a pregnancy that they may risk their own lives and that of their infant
• Women may conceal a pregnancy if they fear significant others will dictate the outcome, eg. forced termination, forced adoption or forced mothering
• Some women in the KISS study who concealed a pregnancy had experienced pre-pregnancy trauma such as child sexual abuse, sexual assault or were in a relationship characterised by violence
• It is essential that concealed pregnancy is viewed as a trauma rather than through a biomedical lens that presumes mental ill health is a causative factor
• Some women report that a concealed pregnancy is a life-altering experience with major consequences including depression, self-blame, complicated maternal-infant attachment, self-harm and suicidal ideation and intent
• Accessible integrated care pathways are urgently required so women can obtain antenatal care and privacy and confidentiality to make an informed decision regarding themselves and their babies.
Critical need for support
Midwives may meet women who are concealing their pregnancy in advanced gestation or during labour. It is critical that midwives are compassionate, non-judgemental and provide empathic listening. Sensitive enquiry about support available to the woman may reveal a hidden story.
The therapeutic relationship at the heart of midwifery care is essential when working with a woman who is experiencing a concealed pregnancy. Recognising that concealed pregnancy is still occurring is the first step to preventing abandonment, neonaticide and negative outcomes for women.
Online information about concealed pregnancy, telephone helplines providing a listening service and non-directive and therapeutic counselling are essential. Integrated care pathways for women are urgently required in order to decrease missed opportunities for engagement with women who conceal a pregnancy. If midwives do not recognise that concealed pregnancies still occur, healthcare systems will continue to fail women and their babies.
Acknowledgement
The authors would like to acknowledge the contribution of the women who participated in The KISS Study and the Health Research Board who funded this research
References
Murphy Tighe S, Lalor JG. Concealed pregnancy: a concept analysis. J Advanced Nursing 2016. Available at: doi:10.1111/jan.12769
Lewis GE. The confidential enquiry into maternal and child health (CEMACH) saving mothers’ lives: reviewing maternal deaths to make motherhood safer 2003-2005. The seventh report on confidential enquiries into maternal deaths in the United Kingdom 2007. CEMACH: London
Conlon C. Concealed pregnancy: a case study approach from an Irish setting. 2006. Dublin: Crisis Pregnancy Agency
Thynne C. Exploring the experience of women who undergo a late disclosure of pregnancy, 2006. Available at: www.lenus.ie
Wessel J, Endrikat J, Busher U. Denial of pregnancy- characteristics of women at risk. Acta Obstetricia et Gynecologicia, 2007; 86: 542-546
English E. Inquiry launched after body of newborn found in house. Irish Examiner 30.07.2013. Available at: www.irishexaminer.com/ireland/inquiry-launched-after-body-of-newborn-baby-found-in-house-238323.html
Riegel R. Newborn baby found lying dead in a toilet inquest told. Irish Independent August 7, 2014. Available at: www.independent.ie/irish-news/courts/newborn-found-dead-in-toilet-inquest-told-29903635.html
Murphy Tighe S, Lalor JG. Concealed pregnancies, letter to the Irish Times May18, 2015. Available at: www.irishtimes.com/opinion/letters/concealed-pregnancies-1.2214480
BBC, September 1, 2015. Police probe after baby’s body found in River Taaff, Cardiff. Available at: www.bbc.com/news/uk-wales-south-east-wales-3324774
BBC, November 24, 2014. Mother charged for abandoning baby in drain in Sydney. Available at: www.bbc.com/news/world-australia-30172577
Collins P. Irish backpacker in Australia charged with hiding newborn baby. Irish Times, August 9, 2014. Available at: www.irishtimes.com/news/crime-and-law/irish-backpacker-in-australia-charged-with-hiding-newborn-baby-s-body-1.1891221
Ferriter D. Occasions of sin, sex and society in modern Ireland. Suffolk Profile Books 2009
Farrell E. A most diabolical deed: Infanticide and Irish society, 1850-1900. Manchester: Manchester University Press 2012
Rattigan C. What else could I do? Single mothers and infanticide, Ireland 1900-1950. Dublin: Irish Academic Press 2012
Mahon E, Conlon C, Dillon L. Women and crisis pregnancy. Government publications: Dublin 1998
Murphy Tighe S, Lalor JG. When mothering isn’t part of your lifeplan: concealed pregnancy and the link with complicated maternal-infant attachment. Conference proceedings, UNESCO Child and Family Research Centre, 7th Biennial Conference, June 11, 2015. Available at: www.conference.ie/content/MurphyTigheS_Whenmothering%20isntpartofyourlife%20planConcealedPregnancy_1.pdf
Jenkins A et al. Denial of pregnancy- a literature review and discussion of ethical and legal issues. J Royal Society of Medicine 2011; 104: 286-291
Sandoz P. Reactive-homeostasis as a cybernetic model of the silhouette effect of denial of pregnancy. Medical Hypotheses Nov, 2011; 77 (5) 782-5
Kenner WD, Nicholson SE. Psychosomatic disorders of gravida status: false and denied pregnancies. Psychosomatics March-April, 2015; 56(2): 119-28
Hatters Friedman S, Heneghan A, Rosenthal M. Characteristics of women who deny or conceal pregnancy. Psychosomatics, March-April, 2007; (48)2:117-122
Nirmal D, Thijs I, Bethel J, Bhal P. Frequency of denial of pregnancy: results and epidemiological significance of a 1 year prospective study in Berlin. Acta Obstetricia et Gynecologica Scandanavica, 2006; 81: 1021-27
 (click to enlarge)
(click to enlarge)