The issue of unscheduled bleeding in patients on hormonal contraception can plague users and prescribers of contraception. If not managed correctly it can cause a patient to discontinue a method that she might eventually find quite suitable, to say nothing of the chance that the bleeding symptom might also be caused by an as yet undiagnosed form of gynaecological disease.
It is crucial that prescribers have a thorough, systematic but workable method of managing this complaint. In the seventh edition of Prof John Guillebaud’s* handbook, Contraception Today, which was published earlier this year, there is a checklist section on why abnormal bleeding occurs in women who take the contraception pill.
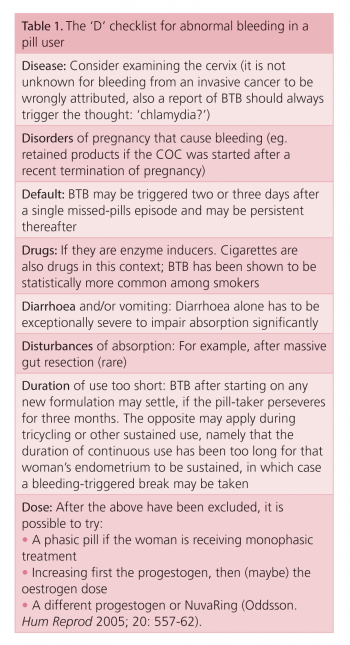
The checklist lends itself to unexpected bleeding in a patient on any from of hormonal contraception.
The ‘D’ checklist includes:
Duration
Default
Drugs
Diarrhoea and vomiting
Disturbances of absorption
Dose
Disorders of pregnancy
Disease.
(click to enlarge)
Duration of use
If we look at each of the possible causes in more detail beginning with duration of use – a woman new to or returning to hormonal contraception will occasionally (10%) experience unexpected bleeding. In most cases it is a harmless, self-limiting consequence of exposing the endometrium to progestogen.
Why does it happen to some but not others?
Many factors are involved in the endometrial shedding that occurs during menstruation and these can be impacted by the use of exogenous hormones. Erratic surface breakdown of the endometrium, abnormal angiogenesis (with wider, thin-walled, more fragile vessel formation) and an increase in the expression of matrix metalloproteinases at the endometrium, among other anomalies have all been observed in women on contraceptive hormones.
In most cases the endometrial disturbances are short-lived and a predictable bleeding pattern will emerge if given enough time. Many patients are not happy to watch and wait. Some are afraid; others are annoyed by the unexpected bleeding and will most likely discontinue the method.
If adequately counselled beforehand and given possible strategies in advance of starting the hormones, women may be more likely to persevere.
There is an excellent management pathway for unexpected bleeding while using longer-acting forms of contraception which GPs should familiarise themselves with.
Default
A woman is far more likely to encounter unexpected bleeding if she does not use her contraceptive hormones as directed. Missed pills are so common as to happen in virtually every packet and the small drop in hormone level by missing one or two pills can easily bring on unexpected or ‘breakthrough’ bleeding (BTB).
Drugs
The third ‘D’ on the list is drugs. Certain medications induce the production of liver enzymes which help to metabolise contraceptive hormones. Women on liver enzyme-inducing (LEI) medications must be careful which forms of hormonal contraception they choose.
Etonogestrel (Implanon NXT) implant cannot be used at all by women on LEI whereas a LNG-IUS (Mirena IUS; or any copper coil) and medroxyprogesterone acetate (Depo-Provera) injections are perfectly fine.
Oral hormones are often given in arbitrarily higher doses (50 micrograms of oestrogen with a combined pill, double doses of progestogen-only pills) but this unlicensed use has not been studied in any detail.
Diarrhoea
Diarrhoea (but more likely vomiting) can precipitate BTB on hormones as there may be impaired absorption through the gastrointestinal tract.
Disturbances of absorption
Thus other disturbances of absorption can also cause BTB. Patients with illnesses like colitis or who have had bowel resection would be best to avoid oral hormones altogether.
Dose
Our sixth ‘D’ on the list is dose. There is a trend among some GP colleagues to commence women who are new to oral contraceptive use on the lower-dose (20mcg) oestrogen pills. There is no evidence to suggest that this is in any way a safer practice. Women who are likely to experience a thromboembolic phenomenon are as likely to have this on a 20mcg pill as a 30mcg pill or higher, but lower-dose pills will be somewhat less efficient at suppressing endometrial shedding and the women will be more inclined to experience BTB.
Current Faculty for Reproductive Healthcare (FSRH) guidance is to start women on a 30mcg, second-generation pill and adjust accordingly depending on their satisfaction.
Disorders of pregnancy
If the pill (unlikely) or its user (more likely) fails then there is a risk of pregnancy. Some women bleed in early pregnancy. This may be a sign of serious pregnancy risk such as an ectopic pregnancy but it may just be the more common unexplained bleeds that sometimes occur.
Either way you need to rule out this unlikely possibility by a clinical pregnancy test before exploring other causes. It also gives the woman better reassurance.
Disease
And finally, but perhaps most important of all the Ds, is that of disease. There are many gynaecological conditions that can cause unexpected bleeding. Among the most common in younger women is infection of the cervix with chlamydia.
Some women are less vigilant about their use of barrier contraception, particularly when they have the security against pregnancy risk that hormonal contraception gives them. If the patient stops using condoms after she begins the pill her unexpected bleeding may be caused by bacteria and not the hormones.
Other conditions such as cervical cancer, cervical and endometrial polyps, etc. can also precipitate unexpected vaginal bleeds.
If a new hormone contraceptive user experiences unexpected bleeding and it has not responded to your first few attempts to modify it within three to four months then I would suggest testing for chlamydia initially (either with endocervical swab or with first void urine if she is only newly sexually active or objects to having a pelvic exam). If this is unhelpful it is time for a speculum exam. If the cervix looks abnormal doctors should not just send a smear, the patient should be referred for investigation.
*Prof John Guillebaud was the first person to be appointed as professor (now emeritus) of family planning and reproductive health at University College, London, and recently presented a masterclass on contraception in Dublin
Reading List
Guillebaud J. Contraception Today – A Pocketbook for General Practitioners and Practice Nurses (seventh edition), 2012
Clinical Effectiveness Unit. Drug interactions with hormonal contraception. London (UK): Faculty of Sexual and Reproductive Healthcare, 2012
Holland G. LARCs and management of vaginal bleeding. Forum 2012; 29(2): 55-6
Livingstone M, Fraser IS. Mechanism of abnormal uterine bleeding. Human Reproduction Update 2011; 8 (1)
 (click to enlarge)
(click to enlarge)