The ideal analgesic for the treatment of breakthrough cancer pain is an analgesic with good efficacy and potency, a rapid onset of action, a relatively short duration of action with minimal side-effects and a good safety profile.
Dr Elaine Wallace, Clinical Fellow, Princess Margaret Hospital, Toronto, Canada
Breakthrough cancer pain (BTcP) is defined as a: “transient exacerbation of pain that occurs either spontaneously, or in relation to a specific predictable or unpredictable trigger, despite relatively stable and adequately controlled background pain.” Background pain, also known as ‘baseline pain’ and ‘persistent pain’, refers to ‘constant or continuous pain of long duration’.2
Characteristics of BTcP
BTcP is reported to affect up to 95% of all cancer patients who experience pain.3 Although variable, a typical BTcP episode is:
Rapid in onset (median onset to peak pain intensity ~3-5 minutes)3
Severe to excruciating in intensity3,4
Short-lived, with a median duration of 30-45 minutes3,4
Largely unpredictable in nature.3-5
BTcP can have a significant negative impact on patients’ quality of life and it can be associated with increased health care costs through additional healthcare professional interactions, hospital admissions and longer inpatient hospital stays.3,6
Traditional management approach to BTcP
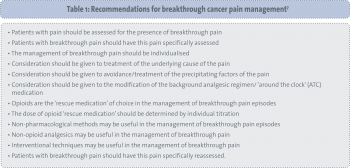
The use of a pharmacological opioid ‘rescue’ dose has traditionally been used in the management of BTcP. Here, a supplemental ‘as required’ dose of analgesia is given along with the regularly scheduled baseline opioid using the same route of administration for both. The ‘rescue’ dose is titrated in line with the baseline dose (See Table 1).7
(click to enlarge)
A major limitation of these short-acting opioids is their relatively slow onset of action. Oral hydrophilic opioids, such as morphine, oxycodone, and hydromorphone, have a delayed absorption and, following oral administration, the average time for onset of pain relief is 30 minutes with an average duration of effect of four hours, by which time the BTcP episode may have come and gone.
New routes of administration
One of the most extensively studied novel routes for medication administration is the transmucosal route. The oral mucosa has many advantages for systemic drug delivery. It is easily accessible, convenient, non-invasive, non-threatening and does not require technical equipment, expertise, preparation or supervision.
The oral mucosa is highly vascularised, highly permeable and has a large surface area and uniform temperature, all of which facilitate rapid absorption. Oral transmucosal drug delivery avoids first pass metabolism and has properties of onset and peak activity similar to those of intravenous morphine.
Nasal delivery of medications is associated with high patient acceptability and familiarity and this non-invasive route has been widely used in the delivery of medications in rhinitis, nasal congestion and migraine. Nasal delivery of medications does not suit hydrophilic medications, ie. morphine, however lipophilic drugs, ie. fentanyl, are rapidly and extensively absorbed via this route.
Dose delivery can be precisely controlled via an easy to use metered nasal spray. Nasal delivery also avoids issues with oral pathologies eg. dry or ulcerated buccal membrane or in cases of nausea or vomiting.
Fentanyl
The ideal analgesic for the treatment of BTcP is an analgesic with good efficacy and potency, a rapid onset of action, a relatively short duration of action with minimal side-effects and a good safety profile. It also needs to be easy to administer and should be inexpensive (see Table 2).8
(click to enlarge)
Fentanyl is a potent, short-acting and well-established opioid, with many years of clinical use as an analgesic and is an ideal molecule for the treatment of BTcP. It is a synthetic opioid and, like morphine, it is a strong mu opioid receptor agonist but is approximately 100-fold more potent than morphine.9 It is absorbed faster than morphine, with a shorter half life.10-12 Due to its high lipid solubility, fentanyl is distributed in all human tissues and, in contrast with morphine, crosses the blood-brain barrier easily and quickly, which explains its strong analgesic effect. Its high lipid solubility thus makes it ideal for delivery via a variety of routes including transmucosal, buccal, sublingual and nasal absorption. Fentanyl also has a lower intensity of the common adverse-effects associated with a central (nausea and vomiting) and peripheral (constipation) mode of action.
Fentanyl formulations
Oral transmucosal fentanyl citrate (Actiq)
Oral transmucosal fentanyl citrate (OTFC [Actiq]) was the first approved rapid-onset opioid. Each OTFC unit consists of a lozenge containing fentanyl on a handle. The lozenge is applied to the buccal mucosa, and as it dissolves in saliva, a proportion of the drug diffuses across the oral mucosa. The patient is required to move the lozenge around in the mouth and twirl the handle for a period of 15 minutes.
Approximately 25% of the total dose of OTFC is rapidly absorbed from the buccal mucosa and becomes systemically available; the remaining 75% of the total dose is swallowed with the saliva and then is slowly absorbed from the gastrointestinal (GI) tract.13,14 Transmucosal absorption into the bloodstream is rapid, with peak plasma concentrations achieved in 20 minutes with the onset of meaningful pain relief reported as < 10 minutes.15,16
Several studies have shown the superiority of OTFC over placebo and over oral morphine in the treatment of BTcP.7,17 As OTFC requires active patient collaboration, it may not be suitable for all patients.
Fentanyl buccatablet (Effentora)
Fentanyl buccal tablet (FBT [Effentora]) is an emerging treatment for BTcP, which uses the OraVescent delivery system. Buccal delivery generates release of CO2 and the OraVescent technology is designed to enhance dissolution and absorption of fentanyl and minimises first-pass effect. The tablet must be left in place for 15-25 minutes until it is dissolved.
Approximately 50% of the total dose of FBT is absorbed transmucosally and becomes systemically available; the remaining half of the dose is swallowed and undergoes more prolonged absorption from the GI tract.18 Randomised controlled trials evaluating FBT have reported improvements in BTcP intensity within 10 minutes of administration among patients with chronic low back pain, non-cancer neuropathic pain and cancer-related breakthrough pain.19-21 Availability of FBT has been shown to be higher in comparison with OTFC.14,22 Effentora is also now licensed to be given sublingually as well as buccally.18
Sublingual fentanyl tablet (Abstral)
Abstral is a new sublingual fentanyl formulation with pharmacokinetics closely matching the profile of BTcP. Formulated as a rapidly disintegrating muco-adhesive sublingual tablet, Abstral is highly lipophilic with the fentanyl dissolving almost instantly and the active substance absorbed via the mucous membrane.23
Abstral’s innovative technology means it requires less than 1ml of fluid to dissolve. It is highly potent, crossing the blood-brain barrier rapidly in both directions, avoiding first-pass metabolism by the liver enzymes and offering approximately 70% bioavailability.24 Studies have shown that the onset of pain relief was significantly faster for Abstral compared with placebo with significant differences evident at 10 minutes after administration and pain relief was sustained for 60 minutes.24
Fentanyl pectin nasal spray (PecFent)
PecFent is a fentanyl pectin nasal spray powered by the innovative PecSys technology which enables rapid but controlled absorption of fentanyl. PecFent is a low volume, aqueous mist of similarly sized droplets delivered to the front areas of the nasal cavity. This technology ensures that the droplets gel when they come into contact with the nasal mucosal surface and thus enables rapid but controlled absorption of fentanyl through a gel matrix.25-27
It has been shown to provide rapid onset to clinically meaningful pain relief at 10 minutes, consistent efficacy and high patient scores for acceptability, simplicity and convenience of use.26,28,29 It has also been shown to be well tolerated with no significant nasal side-effects reported.4,30
Intranasal fentanyl spray (Instanyl)
Intranasal fentanyl spray (IFNS, Instanyl) is another fast-acting nasal opioid approved for the management of BTcP. It bypasses the oral/GI route and thus offers advantages to patients with nausea or vomiting, oral mucositis and impaired gastrointestinal function.
In an open-label, randomised, crossover trial, significantly more patients attained faster ‘meaningful’ pain relief with INFS than OTFC with more patients preferring INFS to OTFC.31,32 The recent launch of the single-dose nasal spray will provide greater flexibility to patients and help to manage dose titration and dose modification, which together with the nasal spray’s safety and convenience should contribute to further improving the management of BTcP.
Safety and practical considerations
In general, transmucosal products are well-tolerated and effective analgesics for BTcP. It is important to note that all these formulations require individual titration. The effective dose for relief of BTcP cannot be predicted from the regularly scheduled baseline opioid or from the previous rescue medication. These newer fentanyl formulations are only licensed for the management of cancer-related breakthrough pain and for patients on maintenance opioid therapy for chronic pain. Concerns exist over the cost of these agents, as well as the appropriate dose titration. Potential also exists for misuse. These formulations are not bio-equivalent, thus 100µg of Abstral does not equate with 100µg of Effentora. Therefore, contrary to what is considered best prescribing practice for other drugs, it is important that these agents are prescribed using proprietary rather that generic names.
(click to enlarge)
Conclusion
BTcP is an important clinical problem, often significantly impacting on a patients’ quality of life. It is likely that the new fentanyl agents will offer advantages over some of the more traditional products. It is vital that these agents are prescribed by a physician experienced in the management of opioid therapy in cancer patients. Adequate assessment and reassessment, along with titration of different analgesics and doses, tailored to the needs of the individual leads to the best management of this heterogeneous condition.
References
Davies A. Current thinking in cancer breakthrough pain management. Eur J Palliat Care 2005; 12(Suppl): 4-6
Ferrell BR, Juarez G, Borneman T. Use of routine and breakthrough analgesia in home care. Oncol Nursing Forum 1999; 26: 1655-1661
Portenoy RK, Raffaeli W, Torres LM et al. Long-term safety, tolerability, and consistency of effect of fentanyl pectin nasal spray for breakthrough cancer pain in opioid-tolerant patients. J Opioid Manag 2010; 6(5): 319-328
Zeppetella G, Catherine A, Collins S. Prevalence and characteristics of breakthrough pain in cancer patients admitted to a Hospice. J Pain Symp Manag 2000; 20(2): 87-92
Svendsen KB, Andersen S, Arnason S et al. Breakthrough pain in malignant and non-malignant diseases: A review of prevalence, characteristics and mechanisms. Eur J Pain 2005; 9: 195-206
Davies A, Dickman A, Reid C et al. The management of cancer-related breakthrough pain: Recommendations of a task group of the Scientific Committee of the Association for Palliative Medicine of Great Britain and Ireland. Eur J Pain 2009; 13; 331-338
Bennett D, Burton AW, Fishman S et al. Consensus panel recommendations for the assessment and management of breakthrough pain. Part II – management. Pharm Ther 2005; 30: 354-361
Prommer E. The role of fentanyl in cancer-related pain. J Palliat Med 2009; 12: 947-954
Reisfield GM, Wilson GR. Rational use of sublingual opioids in palliative medicine. J Pall Med 2007; 10(2): 465-475
Bredenberg S, Duberg M, Lennernäs B et al. In vitro and in vivo evaluation of a new sublingual tablet system for rapid oromucosal absorption using fentanyl citrate as the active substance. Eur J Pharm Sci 2003; 20(3): 327-334
Lennernäs B, Hedner T, Holmberg M et al. Pharmacokinetics and tolerability of different doses of fentanyl following sublingual administration of a rapidly dissolving tablet to cancer patients: A new approach to treatment of incident pain. Br J Clin Pharmacol 2004; 59(2): 249-253
Actiq (fentanyl citrate oral transmucosal lozenge CII), package insert. Salt Lake City, Utah: Cephalon, Inc; September 2009
Mercadante S. Emerging drugs for cancer-related pain. Support Care Cancer 2011; 19(12): 1887-1893
Hanks G. Oral transmucosal fentanyl citrate for the management of breakthrough pain. Eur J Pall Care 2001; 8: 6-9
Lichtor JL, Sevarino FB, Joshi GP et al. The relative potency of oral transmucosal fentanyl citrate compared with intravenous morphine in the treatment of moderate to severe postoperative pain. Anaesth Analg 1999; 89: 732-738
Portenoy RK, Payne R, Coluzzi P et al. Oral transmucosal fentanyl citrate (OTFC) for the treatment of breakthrough pain in cancer patients: a controlled dose titration study. Pain 1999; 79(2-3): 303-312
Effentora (fentanyl buccal tablet) SmPC. Available from http://www.fentora.com/patient/000-default.aspx. Accessed October 10, 2011
Portenoy RK, Messina J, Xie F, Peppin J. Fentanyl buccal tablet (FBT) for relief of breakthrough pain in opioid-treated patients with chronic low back pain: a randomised placebo-controlled stud. Curr Med Res Opin 2007; 23: 223-233
Simpson DM, Messina J, Xie F, Hale M. Fentanyl buccal tablet for the relief of breakthrough pain in opioid-tolerant adult patients with chronic neuropathic pain: a multicenter, randomized double-blind placebo controlled study. Clin Ther 2007; 29: 588-601
Portenoy RK, Taylor D, Messina D, Tremmel L. Randomized, Placebo-Controlled Study of Fentanyl Buccal Tablet for Breakthrough Pain in Opioid-treated Patients With Cancer. Clin J Pain 2006: 22: 805-811
Darwish M, Kirby M, Robertson P Jr et al. Absolute and relative bioavailability of fentanyl buccal tablet and oral transmucosal fentanyl citrate. J Clin Pharmacol 2007; 47(3): 343-350
Abstral SmPC. Available from http://www.ProStrakan.com. Accessed October 11 2011
Rauck R, Tark M, Reyes E et al. Efficacy and long-term tolerability of sublingual fentanyl orally disintegrating tablet in the treatment of breakthrough cancer pain. Curr Med Res Opin 2009; 25(12): 2877-2885
PecFent SmPC 2010. Available from http://www.archimedespharma.com. Accessed October 10 2011
Taylor D, Galan V, Weinstein SM et al. Fentanyl pectin nasal spray in breakthrough cancer pain. J Supp Oncol 2010; 8: 184-190
Fisher A, Watling M, Smith A, Knight A. Pharmacokinetic comparisons of three nasal fentanyl formulations; pectin, chitosan and chitosan-poloxamer 188. Int J Clin Pharmacol Ther 2010; 48(2): 138-145
Fallon M, Gatti A, Davies A et al. Fentanyl pectin nasal spray provides clinically meaningful pain relief and a more rapid onset of analgesia compared with immediate-release morphine sulphate in breakthrough cancer pain. Pall Med 2010; 24: S24 (Abstract)
Farrar JT, Berlin JA, Strom BL. Clinically important changes in acute pain outcome measures: a validation study. J Pain Symp Manag 2003; 25: 406-411
Davis A et al. Consistency of efficacy, patient acceptability, and nasal tolerability of fentanyl pectin nasal spray compared with immediate-release morphine sulfate in breakthrough cancer pain. J Pain Symp Manage 2011; 41(2): 358-366
Mercadante S, Radbruch L, Davies A et al. A comparison of intranasal fentanyl spray with oral transmucosal fentanyl citrate for the treatment of breakthrough cancer pain: an open-label, randomised, crossover trial. Curr Med Res Op 2009; 25(11): 2805-2815
Mercadante S, Radbruch L, Popper L et al. Efficacy of intranasal fentanyl spray (INFS) versus oral transmucosal fentanyl citrate (OTFC) for breakthrough cancer pain: an open-label crossover trial. Abstract presented at EFIC 2009
 (click to enlarge)
(click to enlarge)

