Multiple myeloma (MM) is a malignant neoplasm of clonal plasma cells. Incidence of MM is approximately 4/100,000/year, with a slight male predominance.1 Treatment advancements have led to significant improvements in patient outcomes with a 50% increase in overall survival seen in those diagnosed after 1997 compared with those diagnosed before.2
Since that time, therapeutic options for MM have expanded at an explosive rate, and numerous additional therapeutic agents are now available. Many of the newer treatments in clinical use, or under development, target the immune system which is dysfunctional in MM patients, contributing not only to disease progression but also enabling drug-resistance. These immune-mediated therapies provide new mechanisms to destroy the malignant cells with very promising results, and also reduce dependence on traditional chemotherapy drugs. Myeloma is still considered an incurable disease, but future development of efficacious novel immunotherapies may one day challenge this status.
Current standard of care
The current up-front standard of care treatment for younger, fit patients with MM – outside of a clinical trial – is induction chemotherapy with four cycles of multi-agent chemotherapy, usually based on a bortezomib (proteasome inhibitor)-dexamethasone backbone, followed by high-dose chemotherapy using melphalan and an autologous stem cell transplant (ASCT).
Older patients, or those with comorbidities precluding ASCT are assessed on a case-by-case basis, where quality of life and treatment tolerability are important considerations. Common treatment options include bortezomib-based regimens or use of the immunomodulatory drug lenalidomide with dexamethasone.
There have been numerous advances in MM therapies over the past few years, particularly relating to the field of immunotherapies. In this paper, we will briefly discuss the immunomodulatory drugs (IMiDs), before moving on to monoclonal antibodies, bispecific antibodies and cellular therapies.
Immunomodulatory drugs (IMiDs)
The IMiDs are thalidomide and its derivatives lenalidomide and pomalidomide. They were first trialled in MM for their ability to inhibit angiogenesis,3 enabling limitation of the spread of malignant cells within the bone marrow microenvironment. Their mechanism of action is multifaceted, with effects on cell survival, proliferation, spread within the bone marrow, and importantly, upregulation of the host immune system. IMiDs act via binding to cereblon, a component of the E3 ubiquitin ligase enzyme. This results in labelling of the Ikaros family zinc finger protein (IKZF) transcription factors 1 and 3 with the ubiquitin tag, which targets them for destruction by the cellular proteasome.
The resultant reduction in levels of IKZF1 and -3 in turn leads to reduced transcription of MYC and IRF4, which are required for survival and proliferation,4 and in upregulation of production of the cytokines IL-2 and IFN-γ, stimulating improvement in T-cell and NK cell responses.5,6,7 This facilitates detection and subsequent immune-mediated destruction of MM cells.
The newer IMiDs, lenalidomide and pomalidomide, are more effective anti-myeloma treatments and less toxic than thalidomide, which causes significant gastrointestinal toxicity, thrombotic risk and sleep disturbance. Lenalidomide is used in the frontline setting in Ireland, and as maintenance after ASCT. Pomalidomide is currently licensed only in relapsed disease.
Monoclonal antibodies
Monoclonal antibodies target specific tumour antigens or surface markers in order to stimulate an immune response and facilitate cell killing. Recent years have seen a marked expansion in monoclonal antibodies for use in MM.
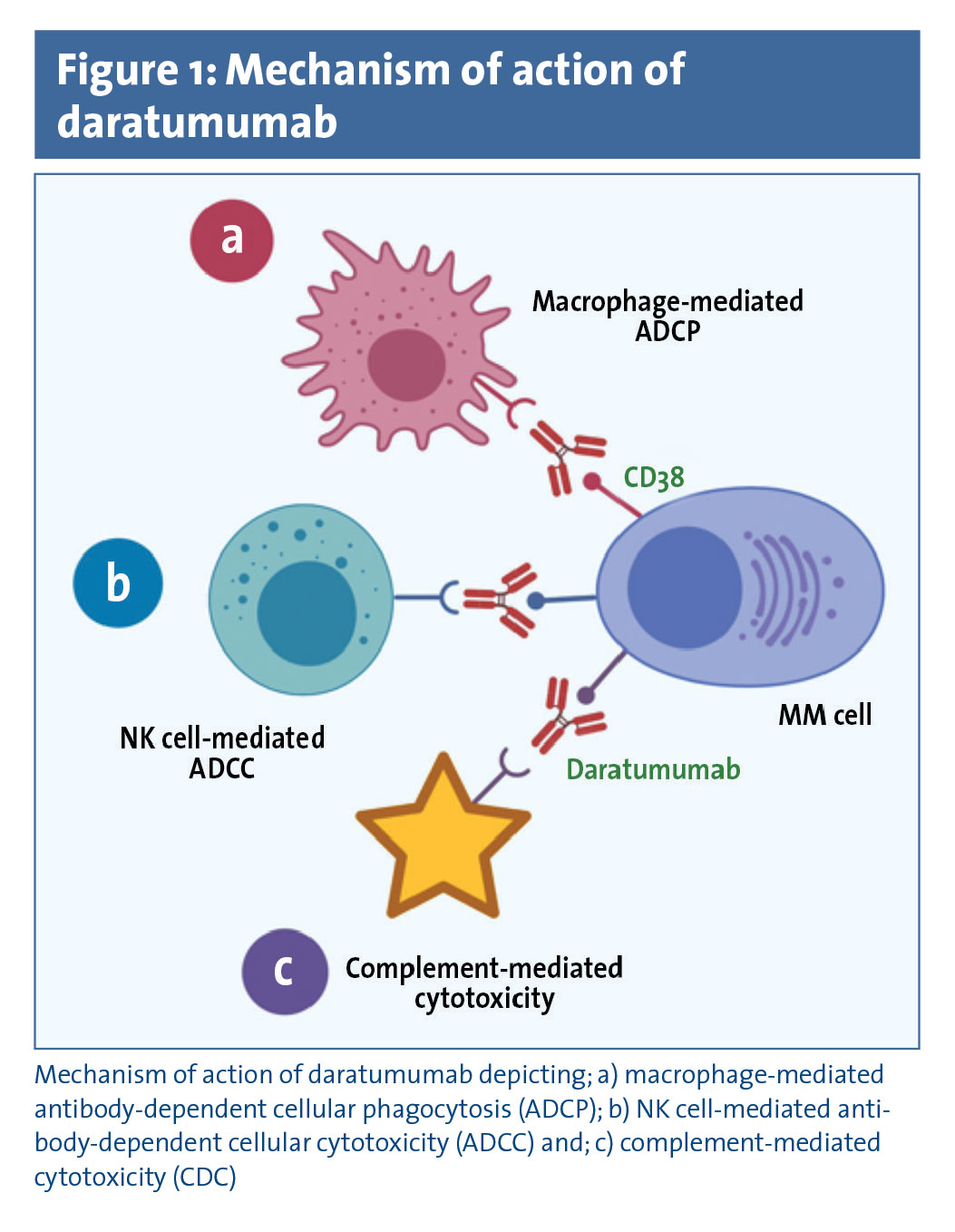
Daratumumab is a fully humanised anti-CD38 monoclonal antibody that kills myeloma cells by three mechanisms:
Antibody-dependent NK cell-mediated cellular cytotoxicity (ADCC)
Complement-dependent cytotoxicity (CDC), and
Antibody-dependent cellular phagocytosis (ADCP), via macrophage phagocytosis of antibody-tagged MM cells (see Figure 1).
(click to enlarge)
Single-agent daratumumab yielded an overall response rate (ORR) of 35% in relapsed refractory MM (RRMM).8 The addition of lenalidomide has been shown to improve ADCC of daratumumab in preclinical studies, and low doses of the traditional chemotherapy drug cyclophosphamide improve macrophage-dependent ADCP,9,10 increasing killing of MM cells through phagocytosis by host immune cells.
Phase III trials of daratumumab with either lenalidomide/dexamethasone or bortezomib/dexamethasone in transplant-eligible patients have shown impressive responses in RRMM with a 12-month progression-free survival (PFS) rate of 83.2% versus 60.1% for standard of care, and 60.7% versus 26.9% respectively.11,12 In the up-front setting, non-transplant candidates have also had excellent responses with daratumumab, in combination with both bortezomib/melphalan/prednisolone, and lenalidomide/dexamethasone.13,14 In both these trials, complete response (CR) rate was approximately doubled in the daratumumab arm, with significant prolongation of PFS seen.
In Ireland, the improvement in daratumumab activity induced by low doses of cyclophosphamide in vitro is the focus of an ongoing study in which the combination of daratumumab with cyclophosphamide, bortezomib and dexamethasone (CyBorD-Dara regimen) in previously untreated transplant-eligible patients is being studied, with excellent results being identified thus far. Of the patients (n = 15) who received induction therapy with CyBorD-Dara followed by high-dose therapy and ASCT, early results show 92% achieved complete response (CR) or near-CR, with a significant number attaining minimal residual disease (MRD) negativity in post-transplant samples, indicating absence of disease at a very low level indeed.15
Early evidence from this and other trials of very high response rates frontline suggest that the efficacy of daratumumab is likely to be better in the initial treatment of patients, rather than in those with relapsed disease. This relates to ongoing, progressive immune dysfunction that occurs throughout the MM disease course, acting to subvert the mechanisms by which the monoclonal antibodies function. The possibility of using daratumumab frontline in both transplant-eligible and -ineligible patients is an attractive one, and it has been suggested that it could become the ‘rituximab of myeloma’ in the future.
Based on the results of these major trials, daratumumab is available for use in Ireland in patients previously treated with, or unable to receive both an immunomodulatory drug and a proteasome inhibitor. It is licensed in Europe for initial treatment in elderly transplant-ineligible patients, however not yet available in Ireland for this indication.
Elotuzumab is a humanised anti-SLAMF7 (signalling-lymphocyte-activating molecule F7) monoclonal antibody, also reliant upon NK-mediated ADCC and macrophage-mediated ADCP. Single-agent elotuzumab has not demonstrated significant efficacy, however, responses have been seen in combination with IMiDs or proteasome inhibitors.16 Elotuzumab is not currently available for routine use outside of a clinical trial, however daratumumab is the more potent of the two.
Bispecific antibodies, compared with monospecific antibodies, recognise two (or more) cell surface markers. As such, they have the potential to simultaneously inhibit multiple survival and proliferation pathways, or redirect immune cells to the tumour through expression of T-cell/NK-cell markers alongside a tumour cell epitope, or increase tumour-specificity via expression of more than one tumour-specific antigen, thereby reducing off-target toxicity.
Bispecific T-cell engagers (BiTEs) are a form of bispecific antibody, which lack the large Fc region. They are smaller with improved tumour-specificity and tissue penetration, but a shorter half-life necessitating frequent administration or continuous infusion.17
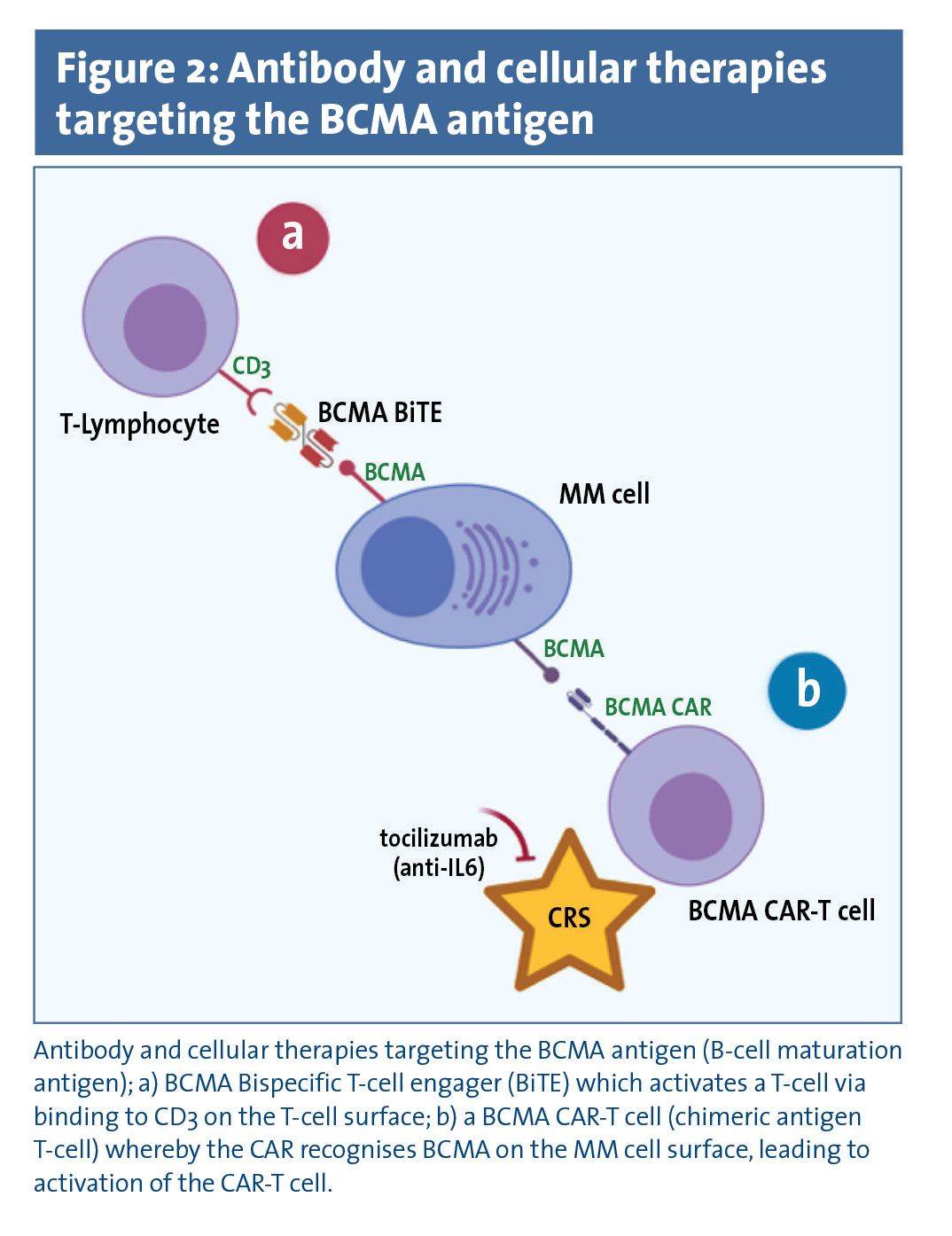
BiTEs target a tumour epitope and a T-cell antigen, usually CD3. Recognition of the tumour epitope leads to T-cell engagement, activation, and cytotoxicity directed against the tumour cell. BCMA (B-cell maturation antigen) has been the focus of the majority of BiTEs to date (see Figure 2).18,19,20
(click to enlarge)
BCMA is a member of the TNF-receptor superfamily required for differentiation of B-cells into mature, immunoglobulin-secreting plasma cells. Early phase I results of the Amgen BCMA BiTE, AMG-420, are encouraging: Of 35 heavily treated, treatment-resistant RRMM patients, six CRs have been achieved, with negative MRD attained in all patients receiving a dose of 400µg/d,21 indicating absence of disease at a low, sensitive level of detection.
Another Amgen BCMA BiTE under development is AMG-701, similar to AMG-420, but with an extended half-life, allowing for easier administration.22 Other bispecific antibodies under investigation are designed to recruit NK cells, rather than T cells, to the MM cells.23,24
Antibody-drug conjugates are also in trial stages. These antibodies release an additional product, usually a chemotherapy drug, after binding to the malignant cell of interest, thereby delivering a toxic product directly to the target cell. GSK285916 is an anti-BCMA antibody linked to the anti-mitotic agent monomethyl auristatin F. In a phase I study, GSK285916 monotherapy produced a 60% response rate and PFS of 7.9 months in RRMM.25,26
Cellular therapies
Despite the advances with antibody therapies, there are still patients who either do not respond, or rapidly progress. High-risk patients, those with aggressive disease based on cytogenetic abnormalities, or who progress quickly despite effective therapy eg. within one-year post-ASCT, have particularly poor outcomes.
Cellular therapies are another new branch of immunotherapies. Data is still relatively immature, but early impressive results have been seen. The longevity of responses is not yet certain, and these treatments carry significant risks of adverse events, however they may offer another therapeutic avenue for a group of patients with very few current options.
T cells
The first cellular therapies took the form of allogeneic stem cell transplant (alloSCT) and donor lymphocyte infusions (DLI). Chronic graft versus host disease (GvHD) confers protection against relapse,27 and DLI can induce a graft-versus-myeloma (GvM) effect.28 However, the increased rate of CR associated with alloSCT is balanced by a high transplant-related mortality, partly attributable to GvHD. Engineering autologous T cells to express tumour-specific receptors allows researchers and clinicians to utilise the cytotoxic properties of T cells in order to kill MM cells, without the risks of GvHD associated with an allogeneic, foreign product. The most well studied form of cellular therapies are the chimeric antigen receptor T cells (CAR-Ts).
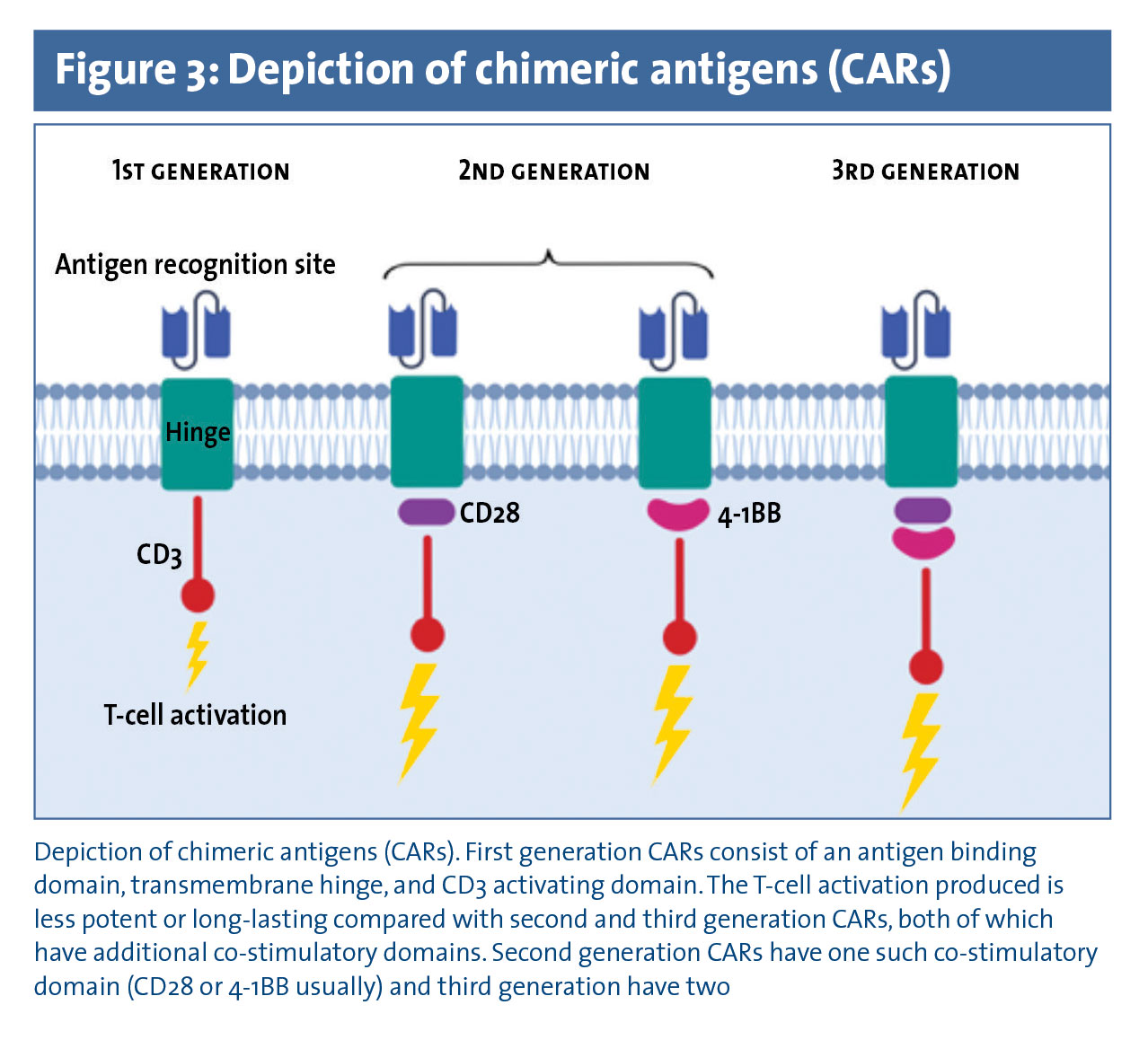
CARs are engineered T-cell receptors with an extracellular domain comprised of a single chain variable fragment of a tumour-specific monoclonal antibody. CAR-T cells can therefore recognise specific tumour epitopes without the usual need for antigen presentation. A transmembrane domain connects the antigen-recognition domain to the T cell activating CD3 domain. Binding of the tumour epitope by the CAR thereby causes direct cytotoxic T cell activation, targeted towards the chosen tumour cell. Second and third generation CARs have an additional one or two co-stimulatory domains which enhance cytokine production, cytolytic capacity, and in vivo persistence of the cellular product (see Figure 3).29
(click to enlarge)
The major toxicity of CAR-T therapy is cytokine release syndrome (CRS), due to the potent T cell response generating a burst of IL-6, interferon-γ and other cytokines. CRS, which is potentially fatal, may produce hypotension, hypoxia, neurological dysfunction, and multisystem organ failure, but can be effectively ameliorated by tocilizumab, an anti-IL6 receptor antagonist.30
Similar to BiTEs, the most promising work to date has been using anti-BCMA CAR-Ts (see Figure 2). BCMA is expressed by late memory B-cells, plasmablasts, mature plasma cells and myeloma cells, but not haematopoietic stem cells or non-haematopoietic cells, making it a good target with comparatively minimal toxicity to normal tissues, compared with other more ubiquitous antigens.31
Bluebird Bio has recently received breakthrough status by the FDA for the bb2121 BCMA CAR. Twenty-one patients with RRMM, two-thirds with high-risk disease features, were infused with the bb2121 CAR-T. At doses of ≥ 150 x 106 the overall response rate (ORR) was 94% with a CR of 56%. Seventy-one percent of patients had CRS which was generally mild, and only around 20% required tocilizumab. Median PFS has not yet been reached, and rates at six and nine months were 81% and 71% respectively, which is extremely encouraging.32 A modification of the bb2121 CAR, bb21217, has increased efficacy and persistence in early clinical trial stages.33
Finally, Legend Biotech has the LCAR-B38M anti-BCMA CAR, which recognises two separate epitopes on the BCMA antigen. Initial data shows an ORR of 100% at a median 17 months follow-up in 19 evaluable patients.34
NK cells
NK cells play a critical role within the innate immune system. NK activity is tightly regulated by the overall balance between numerous activating and inhibitory stimuli. Killer immunoglobulin-like receptors (KIR) are important activating receptors, and KIR-ligand mismatch between donor and recipient, indicating non-self, is associated with reduced relapse rate following T cell-depleted alloSCT, ie. in the absence of any appreciable GvHD.35 Anti-KIR monoclonal antibodies are being studied,36 and use of NK cells to stimulate a GvM effect via KIR-mismatch is being assessed alongside lenalidomide or bortezomib-based regimens, or ASCT.37,38
NK cells engineered with CARs are also being investigated. For example, the combination of daratumumab with CD38-negative NK cells engineered with a SLAMF7-CAR is being trialled, in order to target two myeloma-specific epitopes (CD38 and SLAMF7) while avoiding destruction of NK cells, which are usually CD38-positive, by the daratumumab.39 Other CAR-NK cells targeting alternative tumour cell epitopes are at various stages of development.
Conclusion
Outcomes for patients with MM have improved dramatically over the past decades, particularly since the advent of the immunomodulatory drugs and proteasome inhibitors in the early 2000s, however it still remains an incurable condition. Recent developments in the field of immunotherapies, particularly relating to monoclonal antibodies and cellular therapies are transforming the treatment of these patients. More effective, targeted treatments are becoming available in the frontline setting, and further novel treatments are being developed for RRMM patients, with previously limited options.
 (click to enlarge)
(click to enlarge)