Significant advances have been made in the surgical management of breast cancer, which remains at the core of breast cancer treatment
Dr Patrick Owens, Specialist Registrar in Surgery, NUI Galway and Galway University Hospitals, Galway, Dr Aoife Lowery, Specialist Registrar in Surgery, NUI Galway and Galway University Hospitals, Galway and Prof Michael Kerin, Professor of Surgery, NUI Galway and Galway University Hospitals, Galway
Breast cancer is the most commonly diagnosed cancer in Ireland with over 3,000 new cases each year, accounting for 31% of all invasive cancers. It is the most common cause of cancer-related death in women worldwide.1,2 The increasing incidence of breast cancer with its resultant social and economic burden has stimulated focused efforts to develop and provide appropriate, patient-specific treatment to reduce the morbidity and mortality of the disease. The development of an Irish Cancer Control Network with eight cancer centres, as outlined in ‘A Strategy for Cancer Control’, has been pivotal in addressing the increasing burden of cancer in Ireland.3
Recent decades have seen dramatic changes in breast cancer management including the development of new and effective adjuvant and targeted therapies that have resulted in significant decreases in breast cancer mortality.4,5,6 Current treatment of breast cancer patients is an intricate multidisciplinary process with surgical management remaining at its core. Significant advances have been made in the surgical management of breast cancer, primarily as a result of a series of large, well designed and co-ordinated clinical trials that have shaped modern surgical practice.
Evolving surgical techniques, combined with an improved understanding of tumour biology and increasing efficacy of adjuvant targeted therapies, have resulted in a shift towards increasingly conservative surgical approaches. The introduction of breast cancer screening has changed the profile of the disease at presentation and as surgical treatment continues to evolve, the new paradigm includes an emphasis on oncoplastic techniques and a growing awareness of the psychosocial needs of breast cancer patients. This review will provide an overview of the evidence-base that has guided the evolution to current practices in the surgical management of breast cancer.
Diagnostics and breast cancer screening
Accurate pre-operative diagnosis and staging of breast cancer is critical to optimise therapeutic and surgical strategies. Mammography is the mainstay in diagnostic investigations for breast cancer. Diagnostic mammography is performed in symptomatic patients who present with a palpable mass or other symptoms of breast disease, a personal history of breast cancer or an abnormality detected on a breast screening mammography. Additional imaging studies, including ultrasonography and magnetic resonance imaging (MRI), are also used selectively to characterise breast lesions and aid in surgical planning. Mammography, however, is the only screening examination demonstrated to decrease breast cancer mortality in the general population.7,8,9
The National Breast Cancer Screening Programme in Ireland commenced in 2000. Since 2008, it has provided a programme of two-yearly mammograms to women aged 50-64. The relative risk of breast cancer mortality for women in a breast screening programme compared to controls is estimated to be reduced by 20%.9 Breast cancer screening impacts significantly on the type of breast cancer being diagnosed; screen-detected cancers are generally smaller, lower grade, more hormone-sensitive, more node-negative and less invasive than symptomatic breast cancers.10
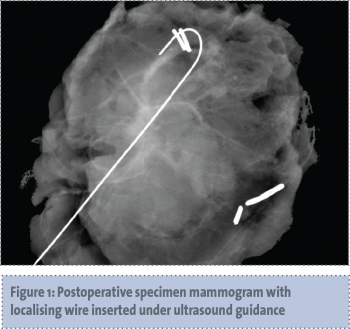
Additionally, since the introduction of breast screening there has been an increase in the detection rate of in situ breast cancers, now accounting for 21% of all screen detected breast cancers, a proportion of which will progress to invasive disease if left untreated. The specific tumour characteristics of screen-detected breast cancers have implications for surgical strategy, which has adapted to suit the needs of this population, including radiologically-guided localisation for both biopsy and excision of non-palpable mammographically detected lesions (see Figure 1).
(click to enlarge)
Prior to surgical intervention, confirmed abnormalities on diagnostic imaging studies require further evaluation with a biopsy. Surgical biopsy was the gold standard for diagnosis until the 1990s, when most breast cancers presented at the symptomatic stage. However, the widespread introduction of mammographic screening significantly increased the number of non-palpable breast lesions requiring diagnostic biopsy. Improved methods of obtaining tissue were developed including fine needle aspiration and core biopsy, which are significantly less invasive and can be performed in the outpatient setting. The European Society for Surgical Oncology guidelines recommended that the majority of breast cancers should receive a pre-operative diagnosis by fine needle aspiration or core biopsy.11 More recently in the US, the National Accreditation Program for Breast Centers established “palpation-guided or image-guided needle biopsy as the initial diagnostic approach rather than open biopsy” as one of 19 clinical management standards by which breast centres are measured.12,13
This reflects current practice in Ireland, where breast cancer care has been centralised into eight dedicated centres, which provide a multidisciplinary framework for the care of breast cancer patients. The National Cancer Control Programme and the Health Information and Quality Authority (HIQA) have developed key performance indicators (KPIs) to standardise care in line with international best practice. These KPIs include a recommendation that > 90% of breast cancers should be diagnosed without an operative procedure (open biopsy), with core biopsy being the diagnostic investigation of choice. The majority of breast core biopsies are now done under ultrasound guidance. This approach improves cancer treatment and minimises the number of surgical procedures to which the patient is subjected.
From radical mastectomy to breast conservation
Surgery has always been the primary modality of breast cancer treatment. William Halsted first described the radical mastectomy in 1894.14 This procedure involved removal of the breast, pectoral muscles and regional lymph nodes, and remained the mainstay of breast cancer treatment until the 1970s despite its associated physical and psychosocial morbidity.15 The first steps towards less aggressive surgery to treat breast cancer were taken in the 1970s with the modified radical mastectomy which spared the pectoralis muscles. Subsequent evolution towards more conservative surgery followed as the result of large randomised clinical trials by pioneering investigators, which demonstrated comparable survival with less radical surgical approaches combined with adjuvant radiotherapy and systemic therapy.
The National Surgical and Adjuvant Breast and Bowel Project (NSABP), founded in 1957, has conducted a number of landmark prospective, randomised controlled trials, giving rise to Level 1A evidence for breast cancer management. NSABP B-04 compared outcomes in patients who underwent radical mastectomy, total mastectomy or total mastectomy with regional radiotherapy, and demonstrated with 25-year follow-up that less aggressive surgery, with or without radiotherapy, would provide equivalent outcomes to radical mastectomy.16 The evidence from this practice-changing study brought about an end to Halsted’s radical mastectomy and signalled a paradigm shift in our approach to breast cancer treatment. Attempts to further reduce the radicality of breast cancer surgery led to the concept of breast conservation. A subsequent series of prospective randomised trials were designed to evaluate breast conserving surgery (BCS) or ‘lumpectomy’ in smaller tumours (see Table 1).17,18,19,20,21,22,23,24
(click to enlarge)
Taken together, the data from these studies, some with follow-up of more than 20 years, has established that survival is equivalent for mastectomy and BCS followed by adjuvant radiotherapy. NSABP B-06, the only one of these trials which required negative resection margins, published 20-year follow-up of 1,851 patients, which concluded that lumpectomy followed by breast irradiation is an appropriate therapy provided that the margins of resected specimens are tumour free and an acceptable cosmetic result can be obtained.17
Importantly, although there was no difference in overall survival between the groups, those that underwent lumpectomy without radiation had a high recurrence rate of 39.2% at 20 years. This data established the acceptance of BCS and also confirmed the importance of radiation in this therapeutic strategy. Since these practice-changing trials were conducted, the rates of locoregional recurrence (LRR) have decreased further due to factors including improved imaging, increased attention to negative margins and advances in adjuvant and targeted therapy for breast cancer. The use of systemic chemotherapy, tamoxifen and trastuzumab have all been shown to significantly reduce the rate of locoregional or in-breast recurrence following BCS; recurrence rates of approximately 6% at 12 years follow-up are reported following breast conservation combined with contemporary adjuvant therapy.25,26
The importance of disease-free margins of resection to minimise LRR is well recognised and there is consensus that negative margins, where there are no tumour cells adjacent to any edge of the resected specimen, is a requirement for BCS.27 The anatomically complete resection of the tumour is not the only factor which impacts on LRR; there is an increasing recognition of the heterogeneity of breast cancer, and molecular sub typing has identified genetically distinct subtypes based on the expression of specific genes including oestrogen receptor (ER), progesterone receptor (PR) and HER2/neu receptor.28 These subtypes have been shown to be predictive of outcomes including response to adjuvant therapy and LRR.29 This highlights the importance of considering breast cancer biology in addition to the extent of surgical excision in adjuvant treatment decisions.
Since there is no difference in overall survival between BCS and mastectomy, the primary aim of BCS is to adequately excise the breast tumour with oncologically acceptable outcomes while maintaining an optimal aesthetic outcome with minimal loss of breast tissue. Appropriate patient selection is crucial to the success of this approach and there remain some contraindications to BCS, including a history of prior therapeutic radiotherapy, persistently positive resection margins following repeated attempts at re-excision, multifocal disease or diffuse malignant calcifications. Large tumour size relative to breast size was previously considered to be a contra-indication to BCS, however, the increased use of neoadjuvant systemic therapy to downstage tumours pre-operatively has increased the cohort of patients for whom BCS may be indicated. Neoadjuvant systemic therapy has been shown to reduce the mastectomy rate by 16.6% while maintaining equivalent survival rates when compared to delivery of systemic therapy adjuvantly.30,31
Oncoplastic breast preservation surgery
Another development that has facilitated BCS for larger tumours is the new paradigm of oncoplastic breast preservation surgery, which combines oncologic principles with plastic surgery techniques to provide wide surgical margins while preserving the appearance and shape of the breast.32 Oncoplastic surgery by definition is a therapeutic procedure only undertaken on biopsy proven tumours. The specific goals of oncoplastic surgery are to remove the lesion with clear margins, to obtain excellent cosmesis and to perform one definitive surgery.32 To achieve these goals, surgical techniques employed by the oncoplastic surgeon include crescent, batwing, inframammary, periareolar and triangular incisions. Advancement flaps and the Benelli ‘round block’ mastopexy are also commonly performed.33 The choice of technique is tailored to the individual patient and depends on factors including tumour size, tumour location within the breast, breast size and shape, and the need for a symmetrising procedure on the contralateral breast. Oncoplastic techniques have been shown to have comparable therapeutic outcomes when compared to BCS alone, with patients also being more satisfied with cosmetic outcomes.34
Breast reconstructive surgery
Despite advances in neoadjuvant systemic therapy and oncoplastic techniques, there remain patients for whom mastectomy is the optimal therapeutic surgical procedure (large multifocal tumours, inflammatory breast cancer, history of previous irradiation). Most patients requiring mastectomy are now offered reconstructive surgery35 and it has been shown that breast reconstruction does not impact on the efficacy of adjuvant therapy or the ability to detect recurrence.36 Immediate breast reconstruction has become increasingly popular, with patients undergoing oncologic mastectomy and reconstruction in a single procedure. With the increase in immediate reconstruction, skin-sparing mastectomy has developed as a technique to preserve the natural skin envelope at the time of mastectomy, which can then be used in the reconstructive surgery to improve cosmetic outcomes. Meta-analyses of prospective studies demonstrate that this approach provides equivalent oncologic outcomes to simple mastectomy.37 A further development is nipple and areola-sparing mastectomy, which preserves the entire skin envelope including the areola and nipple. This approach is predominantly utilised for high-risk patients with BRCA 1 or 2 mutations undergoing risk-reducing surgery,38 but has also been used in the treatment of highly selected tumours of small size and adequate distance from the nipple.39 Retrospective series report that the oncologic outcomes are comparable to skin-sparing mastectomy.40
Reconstruction methods frequently utilised in patients undergoing mastectomy include implants, with or without tissue expanders and/or autologous tissue flaps such as an extended latissimus dorsi flap or deep inferior epigastric perforators (DIEP) flap. Mammoplasty may also be undertaken on the contralateral breast, often in patients where large ipsilateral lesions have been resected (see Figures 2, 3 and 4).32
(click to enlarge)
(click to enlarge)
(click to enlarge)
The principal advantage of BCS, skin- and nipple-sparing mastectomies with breast reconstructive techniques, compared to traditional mastectomy, is that of improved aesthetic outcome and reduced psychosocial morbidity while maintaining oncological safety.41,42
Surgery of the axilla
Axillary nodal disease is a significant prognostic indicator for breast cancer overall survival and disease recurrence, with extent of positive nodes determining the pathological staging of the disease. As discussed previously, NSABP B-04 demonstrated that no survival advantage was conferred by undertaking axillary lymph node dissection (ALND) in addition to mastectomy for early breast cancers.16 Despite the absence of a survival advantage, surgical evaluation of the axilla remains valuable for disease staging, to inform decisions regarding adjuvant therapy and for locoregional control. Although these indications remain valid, ALND of disease-free axillary nodes may result in significant morbidity for patients including lymphoedema, axillary seroma, pain and shoulder problems such as brachial plexus injuries.43,44
The development of sentinel lymph node biopsy (SLNB) represented a significant change in practice and has negated the need for extensive axillary dissection in clinically node-negative patients while still facilitating pathological tumour staging. The concept was initially described in 1960 by Gould et al, in the setting of a parotid gland neoplasm.45,46 The technique is based on the theory that the first lymph node draining the primary tumour reflects the disease status of the regional lymph node basin. SLNB in breast cancer was firmly established in the 1990s by Morton, Giuliano et al, who used blue dye, injected subdermally into the breast, to identify the sentinel node.47,48,49 In 1997, Veronesi et al utilised particles of albumin, labelled with a radioisotope, technetium-99m, as a tracer to identify the sentinel node. Following tracer injection the sentinel node was identified both pre-operatively and intra-operatively using scintigraphy and a hand-held gamma-ray detector probe. In patients where a sentinel node was identified, their method accurately determined nodal status in 98% of patients.50
Following these early results, a number of prospective randomised controlled trials were published, with a total of more than 10,000 patients, demonstrating similarly high sentinel node detection rates and further confirming the role of SLNB (see Table 2).51,52,53,54,64 One such trial, NSABP B-32, conducted between 1999 and 2004, enrolled 5,611 patients and importantly demonstrated that in patients with clinically negative axillary nodes and pathologically negative SLNBs, no survival benefit was gained by performing completion ALND.51 Furthermore, the multicentre ALMANAC trial published in 2006 demonstrated significantly improved quality of life and reduced arm morbidity, at all measured time points up to one year, for patients randomised to SLNB rather than traditional ALND. They also observed reduced drain usage, length of hospital stay, and time to resumption of normal day-to-day activities after surgery.54 SLNB following BCS is currently the standard of care for early stage breast cancers and has been a revolutionary advancement in breast cancer management, avoiding ALND in those with a positive SLNB.
(click to enlarge)
More recent debate has centred around the management of patients with a positive SLNB. Traditionally, completion ALND was advocated in this scenario. Disease in the SLN is classified according to the American Joint Committee on Cancer based on burden of tumour cells as follows (see Figures 5, 6 and 7):55
• Isolated tumour cells (ITC) < 0.2mm of disease
• Micrometastases 0.2-2mm of disease
• Macrometastases > 2mm of disease.
(click to enlarge)
(click to enlarge)
(click to enlarge)
Low burden axillary metastatic disease (ITC and micrometastases) are frequently occult and only detected when additional, non-standard pathological investigations including immunohistochemistry are performed on the SLN. The clinical significance of micrometastatic disease in terms of overall survival has been examined by three large studies, concluding that the presence of occult/micrometastatic disease does not impact significantly on overall survival (see Table 3).51,56,63 The data from these trials taken together strengthened the argument for no further axillary treatment in patients with micrometastatic disease, which is now the recommendation of the American Society of Clinical Oncology (ASCO).57
(click to enlarge)
To address the question of macrometastatic axillary disease, the American College of Surgeons Oncology Group (ACOSOG) conducted the Z0011 trial, which randomised patients with a positive SLNB into two arms: ALND or no further surgery.58 Both cohorts underwent BCS with adjuvant whole breast irradiation and hormonal and/or systemic chemotherapy. Results at six-year follow-up demonstrated no significant difference in overall survival or locoregional recurrence between the groups. The authors concluded that omission of ALND in low axillary disease burden (< 3 positive nodes) may be a reasonable management strategy in select patients only. There has been much debate on the applicability of these results to clinical practice, with critics citing the incomplete accrual of patients, non-significant differences in prognostic factors between the groups and questions regarding clarity of the radiotherapy fields as flaws of the study. Nonetheless, this trial has been practice changing; ASCO has this year revised its guidelines for SLNB, recommending that ALND can be omitted for selected patients with macrometastatic disease.57
The concept that ALND is not necessary for all patients with SLN metastases has been further supported by recent data from the European Organisation for Research and Treatment of Cancer AMAROS trial.59 This study demonstrated that, in select patients, adjuvant axillary radiotherapy provides comparable locoregional control of metastatic disease to ALND with a significantly reduced risk of lymphoedema; a further move towards conservation and reduced morbidity for breast cancer patients.
Further clinical trials are ongoing to determine whether the change in practice effected by the Z0011 results can also be applied to patients with larger primary tumours, post-mastectomy, post partial breast irradiation, and in those undergoing neoadjuvant systemic therapy. However, until these data mature, there remain indications for ALND in select patients (see Table 4).
(click to enlarge)
While the surgical approach to the axilla has become increasingly conservative, there has been an increasing recognition of the importance of tumour biology in prognostication. Through gene expression profiling studies, we now have predictive tools which are increasingly used to guide adjuvant therapy decisions, for example Oncotype DX.60 Ongoing trials are evaluating the potential for such tools to inform decision-making even in node-positive patients.61,62
It is possible that in the future, node-positive patients may be spared chemotherapy based on a favourable biological profile. This is something that will need to be considered when planning axillary treatment and locoregional control as, to date, the evidence driving our new conservative approach has been based on patients treated with systemic therapy. The importance of multidisciplinary decision-making in this new era of conservative surgery coupled with increasingly tailored adjuvant therapeutic strategies cannot be underestimated.
Conclusion
Surgery for breast cancer has evolved significantly over the past 50 years. The goal of contemporary breast cancer management is for individualised therapy. An increased recognition of the biological heterogeneity of the disease has greatly informed current management.
While adjuvant therapy advances have moved towards targeted therapy, surgical advances, based on the results from well-designed randomised trials, have been aimed at minimising morbidity from extensive surgery.
We have progressed from radical surgery to an era of conservation. Surgical management is now tailored for each individual patient and may include a variety of breast conserving techniques with SLNB and reconstruction methods that optimise both oncologic and psychosocial outcomes for patients. As the biological complexity of breast cancer is further uncovered and locoregional treatment strategies continue to evolve, the optimal setting for multimodality breast cancer treatment remains the multidisciplinary framework where therapeutic advances can be critically assessed and implemented for continued improvements in cancer outcomes.
References
Cancer in Ireland 1994-2011: Annual report of the National Cancer Registry. National Cancer Registry, 2014.
Press Release No. 223 Latest world cancer statistics WHO International Agency for Research on Cancer. December 12, 2013.
Redmond P. A Strategy for Cancer Control in Ireland. National Cancer Forum, 2006.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365(9472): 1687-717.
Clarke M, Collins R, Darby S, et al. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 366(9503): 2087-106.
Clarke M. Meta-analyses of adjuvant therapies for women with early breast cancer: the Early Breast Cancer Trialists’ Collaborative Group overview. Ann Oncol 2006; 17(Suppl 10): x59-62.
Weedon-Fekjaer H, Romundstad PR, Vatten LJ. Modern mammography screening and breast cancer mortality: population study. BMJ (Clinical research ed) 2014; 348: g3701. PubMed PMID: 24951459. Pubmed Central PMCID: PMC4061379. Epub 2014/06/22. eng.
Christiansen P, Vejborg I, Kroman N, et al. Position paper: breast cancer screening, diagnosis, and treatment in Denmark. Acta Oncologica 2014; 53(4): 433-44. PubMed PMID: 24495043. Epub 2014/02/06. eng.
Marmot MG, Altman DG, Cameron DA, Dewar JA, Thompson SG, Wilcox M. The benefits and harms of breast cancer screening: an independent review. Br J Cancer 2013; 108(11): 2205-40. PubMed PMID: 23744281. Pubmed Central PMCID: PMC3693450. Epub 2013/06/08. eng.
Burke JP, Power C, Gorey TF, Flanagan F, Kerin MJ, Kell MR. A comparative study of risk factors and prognostic features between symptomatic and screen detected breast cancer. Eur J Sur Oncol 2008; 34(2): 149-53. PubMed PMID: 17498912. Epub 2007/05/15. eng.
O’Higgins N, Linos DA, Blichert-Toft M, et al. European guidelines for quality assurance in the surgical management of mammographically detected lesions. European Breast Cancer Working Group. Annales Chirurgiae et Gynaecologiae 1998; 87(1): 110-2. PubMed PMID: 9598249. Epub 1998/05/23. eng.
Moran MS, Kaufman C, Burgin C, Swain S, Granville T, Winchester DP. What currently defines a breast center? Initial data from the national accreditation program for breast centers. J Oncol Practice 2013; 9(2): e62-70. PubMed PMID: 23814526. Pubmed Central PMCID: PMC3595452. Epub 2013/07/03. eng.
Calhoun KE, Anderson BO. Needle biopsy for breast cancer diagnosis: a quality metric for breast surgical practice. J Clin Oncol 2014; 32(21): 2191-2. PubMed PMID: 24934794. Epub 2014/06/18. eng.
Halsted WS. I. The Results of Operations for the Cure of Cancer of the Breast Performed at the Johns Hopkins Hospital from June, 1889, to January, 1894. Ann Surgery 1894; 20(5): 497-555. PubMed PMID: 17860107. Pubmed Central PMCID: PMC1493925. Epub 1894/11/01. eng.
Cotlar AM, Dubose JJ, Rose DM. History of surgery for breast cancer: radical to the sublime. Current Surgery 2003; 60(3): 329-37.
Fisher B, Jeong J-H, Anderson S, Bryant J, Fisher ER, Wolmark N. Twenty-Five-Year Follow-up of a Randomized Trial Comparing Radical Mastectomy, Total Mastectomy, and Total Mastectomy Followed by Irradiation. NEJM 2002; 347(8): 567-75. PubMed PMID: 12192016.
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. NEJM 2002; 347(16): 1233-41. PubMed PMID: 12393820. Epub 2002/10/24. eng.
Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. NEJM 2002; 347(16): 1227-32. PubMed PMID: 12393819. Epub 2002/10/24. eng.
Litiere S, Werutsky G, Fentiman IS, et al. Breast conserving therapy versus mastectomy for stage I-II breast cancer: 20 year follow-up of the EORTC 10801 phase 3 randomised trial. The Lancet Oncol 2012; 13(4): 412-9. PubMed PMID: 22373563. Epub 2012/03/01. eng.
Poggi MM, Danforth DN, Sciuto LC, et al. Eighteen-year results in the treatment of early breast carcinoma with mastectomy versus breast conservation therapy: the National Cancer Institute Randomized Trial. Cancer 2003; 98(4): 697-702. PubMed PMID: 12910512. Epub 2003/08/12. eng.
Blichert-Toft M, Nielsen M, During M, et al. Long-term results of breast conserving surgery vs. mastectomy for early stage invasive breast cancer: 20-year follow-up of the Danish randomized DBCG-82TM protocol. Acta Oncologica 2008; 47(4): 672-81. PubMed PMID: 18465335. Epub 2008/05/10. eng.
Arriagada R, Le MG, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. Institut Gustave-Roussy Breast Cancer Group. J Clin Oncol 1996; 14(5): 1558-64. PubMed PMID: 8622072. Epub 1996/05/01. eng.
Simone NL, Dan T, Shih J, et al. Twenty-five year results of the national cancer institute randomized breast conservation trial. Breast Cancer Res Treat 2012; 132(1): 197-203. PubMed PMID: 22113254. Epub 2011/11/25. eng.
Arriagada R, Le MG, Guinebretiere JM, Dunant A, Rochard F, Tursz T. Late local recurrences in a randomised trial comparing conservative treatment with total mastectomy in early breast cancer patients. Ann Oncol 2003; 14(11): 1617-22. PubMed PMID: 14581268. Epub 2003/10/29. eng.
Anderson SJ, Wapnir I, Dignam JJ, et al. Prognosis after ipsilateral breast tumor recurrence and locoregional recurrences in patients treated by breast-conserving therapy in five National Surgical Adjuvant Breast and Bowel Project protocols of node-negative breast cancer. J Clin Oncol 2009; 27(15): 2466-73. PubMed PMID: 19349544. Pubmed Central PMCID: PMC2684852. Epub 2009/04/08. eng.
Fisher B, Dignam J, Bryant J, et al. Five versus more than five years of tamoxifen therapy for breast cancer patients with negative lymph nodes and estrogen receptor-positive tumors. J Natl Cancer Inst 1996; 88(21): 1529-42. PubMed PMID: 8901851. Epub 1996/11/06. eng.
Buchholz TA, Somerfield MR, Griggs JJ, et al. Margins for breast-conserving surgery with whole-breast irradiation in stage I and II invasive breast cancer: American Society of Clinical Oncology endorsement of the Society of Surgical Oncology/American Society for Radiation Oncology consensus guideline. J Clin Oncol 2014; 32(14): 1502-6. PubMed PMID: 24711553. Epub 2014/04/09. eng.
Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Nat Acad Sci US 2001; 98(19): 10869-74. PubMed PMID: 11553815. Pubmed Central PMCID: PMC58566. Epub 2001/09/13. eng.
Lowery AJ, Kell MR, Glynn RW, Kerin MJ, Sweeney KJ. Locoregional recurrence after breast cancer surgery: a systematic review by receptor phenotype. Breast Can Res Treatment 2012; 133(3): 831-41. PubMed PMID: 22147079. Epub 2011/12/08. eng.
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 2014; 384(9938): 164-72. PubMed PMID: 24529560. Epub 2014/02/18. eng.
Mieog JS, van de Velde CJ. Neoadjuvant chemotherapy for early breast cancer. Expert Op Pharmacotherapy 2009; 10(9): 1423-34. PubMed PMID: 19505212. Epub 2009/06/10. eng.
Silverstein MJ, Mai T, Savalia N, Vaince F, Guerra L. Oncoplastic breast conservation surgery: The new paradigm. J Surg Oncol 2014; 110(1): 82-9.
Benelli L. A new periareolar mammaplasty: the ‘round block’ technique. Aesthetic Plastic Surgery 1990; 14(2): 93-100. PubMed PMID: 2185619. Epub 1990/01/01. eng.
Losken A, Dugal CS, Styblo TM, Carlson GW. A meta-analysis comparing breast conservation therapy alone to the oncoplastic technique. Ann Plastic Surgery 2014; 72(2): 145-9. PubMed PMID: 23503430. Epub 2013/03/19. eng.
Heneghan HM, Prichard RS, Devaney A, et al. Evolution of breast cancer management in Ireland: a decade of change. BMC Surgery 2009; 9 :15. PubMed PMID: 19765289. Pubmed Central PMCID: PMC2753567. Epub 2009/09/22. eng.
Allweis TM, Boisvert ME, Otero SE, Perry DJ, Dubin NH, Priebat DA. Immediate reconstruction after mastectomy for breast cancer does not prolong the time to starting adjuvant chemotherapy. Am J Surgery 2002; 183(3): 218-21. PubMed PMID: 11943114. Epub 2002/04/12. eng.
Lanitis S, Tekkis PP, Sgourakis G, Dimopoulos N, Al Mufti R, Hadjiminas DJ. Comparison of skin-sparing mastectomy versus non-skin-sparing mastectomy for breast cancer: a meta-analysis of observational studies. Ann Surgery 2010; 251(4): 632-9. PubMed PMID: 20224371. Epub 2010/03/13. eng.
Yao K, Liederbach E, Tang R, et al. Nipple-Sparing Mastectomy in BRCA1/2 Mutation Carriers: An Interim Analysis and Review of the Literature. Annals of surgical oncology. 2014 Jul 15. PubMed PMID: 25023546. Epub 2014/07/16. Eng.
Sacchini V, Pinotti JA, Barros AC, et al. Nipple-sparing mastectomy for breast cancer and risk reduction: oncologic or technical problem? J Am Coll Surgeons 2006; 203(5): 704-14. PubMed PMID: 17084333. Epub 2006/11/07. eng.
Wang F, Peled AW, Garwood E, et al. Total Skin-Sparing Mastectomy and Immediate Breast Reconstruction: An Evolution of Technique and Assessment of Outcomes. Ann Surgical Oncol 2014 Jul 23. PubMed PMID: 25052246. Epub 2014/07/24. Eng.
Baildam A, Bishop H, Boland G, et al. Oncoplastic breast surgery – a guide to good practice. Eur J Surgical Oncol 2007; 33 Suppl 1: S1-23. PubMed PMID: 17604938. Epub 2007/07/03. eng.
Al-Ghazal SK, Fallowfield L, Blamey RW. Comparison of psychological aspects and patient satisfaction following breast conserving surgery, simple mastectomy and breast reconstruction. Eur J Cancer (Oxford, England : 1990). 2000; 36(15): 1938-43. PubMed PMID: 11000574. Epub 2000/09/23. eng.
Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol 2007; 25(24): 3657-63. PubMed PMID: 17485711. Epub 2007/05/09. eng.
Fleissig A, Fallowfield LJ, Langridge CI, et al. Post-operative arm morbidity and quality of life. Results of the ALMANAC randomised trial comparing sentinel node biopsy with standard axillary treatment in the management of patients with early breast cancer. Breast Can Res Treatment 2006 ;95(3): 279-93. PubMed PMID: 16163445. Epub 2005/09/16. eng.
Gould EA, Winship T, Philbin PH, Kerr HH. Observations on a ‘sentinel node’ in cancer of the parotid. Cancer 1960; 13: 77-8. PubMed PMID: 13828575. Epub 1960/01/01. eng.
Tanis PJ, Nieweg OE, Valdes Olmos RA, Th Rutgers EJ, Kroon BB. History of sentinel node and validation of the technique. Breast Can Res 2001; 3(2): 109-12. PubMed PMID: 11250756. Pubmed Central PMCID: PMC139441. Epub 2001/03/16. eng.
Morton DL, Wen DR, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surgery 1992; 127(4): 392-9. PubMed PMID: 1558490. Epub 1992/04/01. eng.
Giuliano AE, Kirgan DM, Guenther JM, Morton DL. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surgery 1994; 220(3): 391-8; discussion 8-401. PubMed PMID: 8092905. Pubmed Central PMCID: PMC1234400. Epub 1994/09/01. eng.
Giuliano AE. Sentinel lymphadenectomy in primary breast carcinoma: an alternative to routine axillary dissection. J Surg Oncol 1996; 62(2): 75-7. PubMed PMID: 8649044. Epub 1996/06/01. eng.
Veronesi U, Paganelli G, Galimberti V, et al. Sentinel-node biopsy to avoid axillary dissection in breast cancer with clinically negative lymph-nodes. Lancet 1997; 349(9069): 1864-7. PubMed PMID: 9217757. Epub 1997/06/28. eng.
Krag DN, Anderson SJ, Julian TB, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase III trial. The Lancet Oncol 2007; 8(10): 881-8. PubMed PMID: 17851130. Epub 2007/09/14. eng.
Cote R, Giuliano A, Hawes D, et al. ACOSOG Z0010: A multicenter prognostic study of sentinel node (SN) and bone marrow (BM) micrometastases in women with clinical T1/T2 N0 M0 breast cancer. J Clin Oncol 2010; 28(18 Suppl).
Straver MME, PhD, Meijnen MP, et al. Sentinel Node Identification Rate and Nodal Involvement in the EORTC 10981-22023 AMAROS Trial. Ann Surgical Oncol 2010; 17(7): 1854-61.
Mansel RE, Fallowfield L, Kissin M, et al. Randomized Multicenter Trial of Sentinel Node Biopsy Versus Standard Axillary Treatment in Operable Breast Cancer: The ALMANAC Trial. J Nat Can Inst 2006; 98(9): 599-609.
McCready DR, Yong WS, Ng AK, Miller N, Done S, Youngson B. Influence of the new AJCC breast cancer staging system on sentinel lymph node positivity and false-negative rates. J Nat Cancer Inst 2004; 96(11): 873-5. PubMed PMID: 15173271. Epub 2004/06/03. eng.
Galimberti V, Cole BF, Zurrida S, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. The Lancet Oncol 2013; 14(4): 297-305. PubMed PMID: 23491275. Pubmed Central PMCID: PMC3935346. Epub 2013/03/16. eng.
Lyman GH, Temin S, Edge SB, et al. Sentinel lymph node biopsy for patients with early-stage breast cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol 2014; 32(13): 1365-83. PubMed PMID: 24663048. Epub 2014/03/26. eng.
Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surgery 2010; 252(3): 426-32; discussion 32-3. PubMed PMID: 20739842. Epub 2010/08/27. eng.
Rutgers EJ, Donker M, Straver ME, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer patients: final analysis of the EORTC AMAROS trial (10981/22023). J Clin Oncol 2013; 31(1).
NICE. Gene expression profiling and expanded immunohistochemistry tests for guiding adjuvant chemotherapy decisions in early breast cancer management: MammaPrint, Oncotype DX, IHC4 and Mammostrat. National Institute for Health and Care Excellence 2013; DG-10.
Gonzalez-Angulo A, Barlow W, Gralow J. A randomized phase III clinical trial of standard adjuvant endocrine therapy chemotherapy in patients (pts) with 1–3 positive nodes, hormone receptor (HR)-positive and HER2-negative breast cancer with recurrence score (RS) of 25 or less: SWOG S1007 [abstract OT1–03-01]. Cancer Res 2011; 71(24 suppl): 607s.
Cardoso F, Piccart-Gebhart M, Van’t Veer L, Rutgers E. The MINDACT trial: the first prospective clinical validation of a genomic tool. Molecular Oncol 2007; 1(3): 246-51. PubMed PMID: 19383299. Epub 2007/12/01. eng.
Giuliano AE, Hawes D, Ballman KV, et al. Association of occult metastases in sentinel lymph nodes and bone marrow with survival among women with early-stage invasive breast cancer. JAMA 2011; 306(4): 385-93. PubMed PMID: 21791687. Epub 2011/07/28. eng.
Veronesi U, Paganelli G, Viale G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. NEJM 2003; 349(6): 546-53. PubMed PMID: 12904519. Epub 2003/08/09. eng.
 (click to enlarge)
(click to enlarge)









