Looking at how a national clinical trials network (CTN) in diabetes could benefit practice was the subject of Prof Fidelma Dunne’s presentation at the recent Farmleigh conference.
Having been involved in establishing the Atlantic-Dip in the west of Ireland, Prof Dunne has seen first-hand the benefits of a clinical trials network and was eager to present that there is now a proposal to establish a national network that could greatly impact on the practice of diabetes management in the future.
“We are fortunate in that the Health Research Board has a call out at the moment and we are now in stage 2 proposal for a truly national network involving the Republic of Ireland and Northern Ireland,” said Prof Dunne.
Obstacles to high quality clinical research
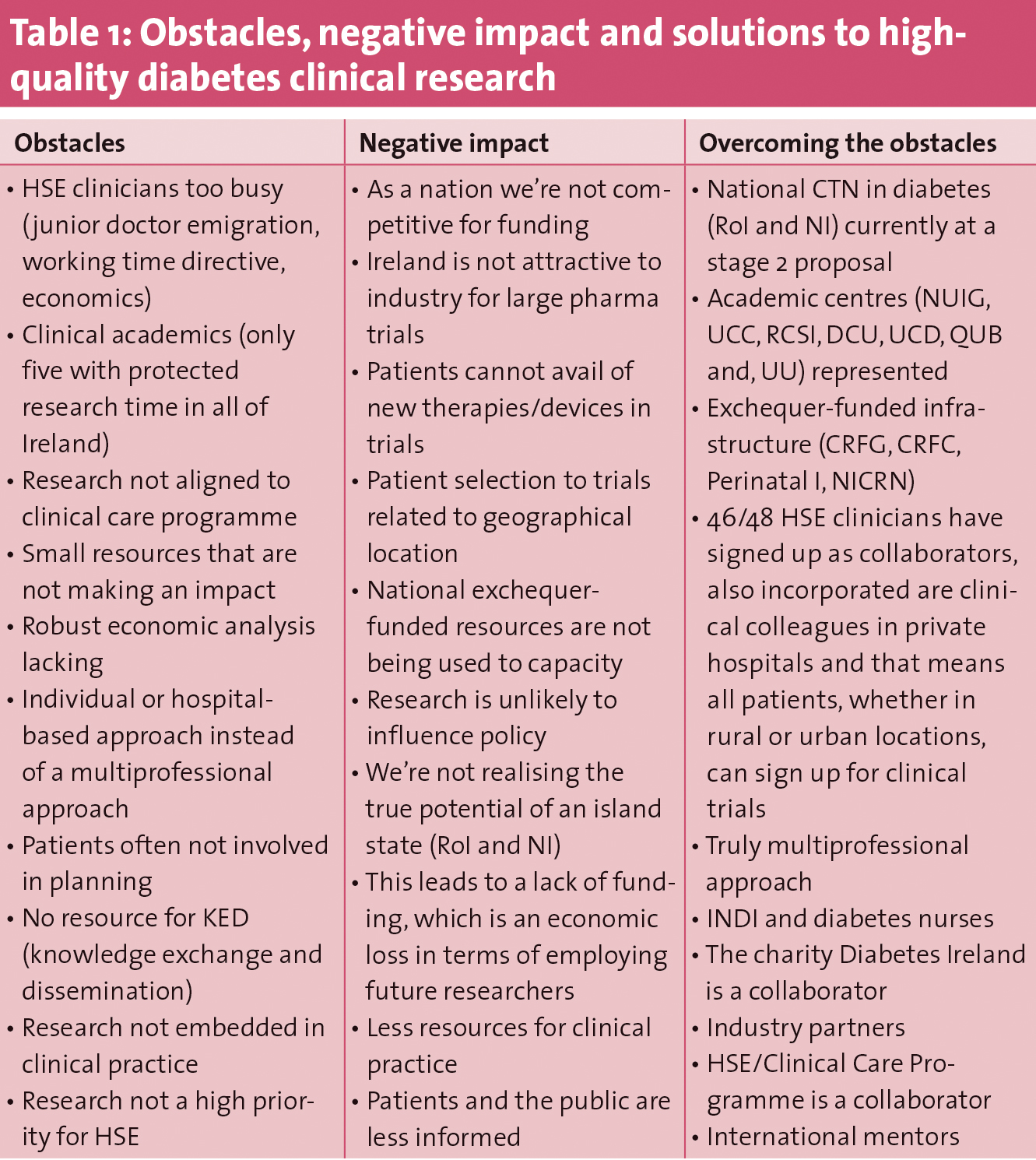
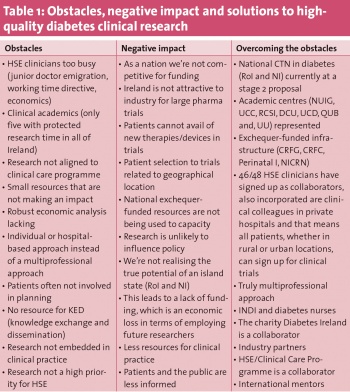
Prof Dunne first outlined the obstacles, the negative impact of these and how to overcome them in order to establish a clinical trials network (see Table 1).
(click to enlarge)
She pointed out that the current economic climate with many junior doctors emigrating has put an additional strain on HSE clinicians’ time, and that there are currently only five HSE clinicians employed in diabetes, herself included, with protected research time. She also pointed out the lack of knowledge exchange and dissemination.
“If we don’t tell people about the issue and how we might solve the issue, then we’re never going to have an outcome,” she said.
Negative impact of obstacles
One of the main negative impacts of the obstacles to high quality research in Ireland, Prof Dunne pointed out, was that as a nation, Ireland is not competitive for funding nor is it attractive to industry for large pharma trials.
“As a nation we haven’t realised our true potential as an island state, and that’s incorporating the Republic of Ireland and Northern Ireland as a large grouping’” said Prof Dunne.
When it comes to patient selection for trials, it is like a lottery and dependant of where you live.
“This means that a lot of patients can’t avail of new therapies or devices through clinical trials, and the patients that are selected don’t really provide a good spectrum of the patient population,” said Prof Dunne.
Overcoming the obstacles
The way to overcoming the obstacles to high-quality research in diabetes is by setting up a national clinical trial network. The Health Research Board is currently in the process of evaluating nine clinical network proposals, of which it will choose four to fund at a total of €2.5 million each over five years.
Prof Dunne is the principal investigator on the clinical trial network in diabetes, and it is hoped that if it gets HRB funding,
CTN in diabetes – aims and objectives
The overall aim of a CTN in diabetes would obviously be to improve the health and wellbeing for all patients with diabetes through research.
The objectives of the CTN would be to:
Improve health and wellbeing for patients with diabetes through an active portfolio of ambitious, internationally competitive multicentre trials
Develop a sustainable self-funding network built on peer-reviewed funding applications, industry/charity contribution, leveraged contributions, commissioning from the HSE or clinical care programmes and in-kind resources
Educate and train future diabetes clinical researchers for sustainability.
The strengths of a clinical trial network, Prof Dunne pointed out, would include:
Bringing together national expertise
Access to all hospitals for recruitment
Strong infrastructure, including biostatistics and trial methodologists
Applicants have a track record in attracting funds, which would lead to sustainability
Clinical research facilities have a track record in running large multicentre trials
Access to network of GPs who wish to participate (WestRen, IPCRN)
Research aligned to priorities of the clinical care programme
Engage patients and have knowledge exchange and dissemination through Diabetes Ireland
Industry partners – pharma and device trials
Strong international mentorship with a view to expand to international collaboration.
On the benefits of a CTN beyond the sum of individual benefits, Prof Dunne pointed out that it would allow for a multiprofessional expertise to come together in each project.
“It is allowing us to be able to employ and fund clinical research nurses that can be aligned to hospitals in the regions, and we will have help with grant writing and publications which can often be difficult for individuals,” said Prof Dunne.
“We will have a system and the resources for a proper knowledge exchange and dissemination , proper education and training programmes and ultimately I hope we will have the infrastructure to develop a national biobank to cover all aspects of diabetes,” she added,
Five-year plan
If the CTN in diabetes gets HRB funding, the five-year plan is to undertake one large multicentre study on gestational diabetes screening; seven pilot/feasibility studies in tandem, some/all of which will provide the basis for further DI and which will be aligned with the diabetes clinical care programmes; and network activities which will deliver on dissemination, training, industry engagement, sustainability, working with HSE/clinical care programme, grant writing, building international collaboration and managing growth and expansion of the clinical trial network.
“We realise and recognise that there are still people that we will need to bring into to this network over time,” commented Prof Dunne.
Network sustainability beyond five years
“Our sustainability would be built on national and international peer-reviewed grants, industry-generated trials which would be 40% of our research activity, ongoing HSE commitment and ongoing HSE commissioning of work on the network, university leveraged funding and when we get to it, philanthropic funding I hope,” said Prof Dunne.
Building on experience
That Prof Dunne is the principal investigator for the proposed CTN in diabetes is not random. Based in NUI Galway, her research group is currently conducting a number of studies as part of the HRB-funded ATLANTIC DIP (diabetes in pregnancy) programme. These studies are focusing on among other areas: pre-pregnancy care; screening for GDM; persistent glucose abnormalities following GDM; prevention of type 2 diabetes; genetics of GDM; process of care; screening in primary care; psychosocial implications of GDM; and economic evaluation of GDM.
What is required in order to set up a clinical trial network?
“You need someone with a real passion for the clinical area, with a research need and a clinical need.
“You need to identify the deficiency yourself, and then try to meet that deficiency through research.
“You really need to be committed and you need some funds initially to help you to develop a team around you of likeminded individuals.
“I think it’s really, really, important that there’s electronic data collection, and that has to be part of your clinical service so that electronic data collection has to be audited and cleaned on a ongoing basis.”
Prof Dunne also mentioned that HSE collegiality is important, and that using existing resources in a different way with small additional resources is a good way to start.
“And then you develop your clinical services around the research funds if possible,” said Prof Dunne.
Once a network is set up, how is it maintained?
According to Prof Dunne, one thing generally to leads to another:
“When you set up a network, it attracts researchers. The researchers then attract funds, funds allow outcomes and publications, and publications allow for improvements in your clinical service,” she said.
“You need to have ongoing data cleaning, ongoing education of both patients and staff and you really need to have a regional administrator or somebody that will contribute to the organisational structure around it,” added Prof Dunne.
Communication is also an essential part in maintaining a good CTN.
“It’s really important to package your research outcomes in a way that has meaning for the HSE, and to your clinical colleagues. And it’s important to engage patients in the design of your research and in the service development and in the dissemination of your results. And it’s really important to disseminate your findings locally, national and internationally so that people are well informed.”
The results of the ATLANTIC DIP regional network which was set up in 2006 have lead to a greater knowledge of GDM and the outcomes of pregnancies complicated by GDM. The knowledge gained from the study has lead to great improvements in services and GDM outcomes for mothers and babies, and it is hoped that extending this programme through a national clinical trial network would help mothers nationwide and fight the national disparities that exist in screening for GDM.
What will a national clinical trial network in diabetes do for services?
“From a pregnancy perspective it will allow us to move from a regional to a national approach, but for all the other areas in diabetes that are included in the pilot studies in the network, it will also allow them the opportunity to move in the same direction.”
“What is really the challenge here is that we ensure that the evidence we have collected impacts on national and international policy so that there are tangible benefits for our patients with diabetes, and, in my case, for women with diabetes and their offspring” Prof Dunne concluded.
 (click to enlarge)
(click to enlarge)