Antidepressant medication in breast cancer patients receiving tamoxifen
An exploration of current evidence regarding the co-prescribing of antidepressants and tamoxifen
Dr Muhammad Fahmi Ismail, Non-Consultant Hospital Doctor, South Lee Mental Health Service, Cork University Hospital, Cork and Dr Eugene Cassidy, Consultant Liaison Psychiatrist, Department of Psychiatry, School of Medicine, University College Cork, Cork
Breast cancer is one the most common cancer in women.1 Tamoxifen is an important endocrine therapy used as a component of breast cancer treatment.2 Up to one-in-four patients with breast cancer suffers from a depressive disorder.3 There have been some concerns over the use of antidepressants in this patient group, specifically on its potential risk to alter the effectiveness of tamoxifen.4 More recently, a study has found that co-prescribing certain antidepressants with tamoxifen is associated with an increase in mortality from breast cancer.5 This article explores current evidence regarding the co-prescribing of antidepressants and tamoxifen.
Tamoxifen treatment in breast cancer
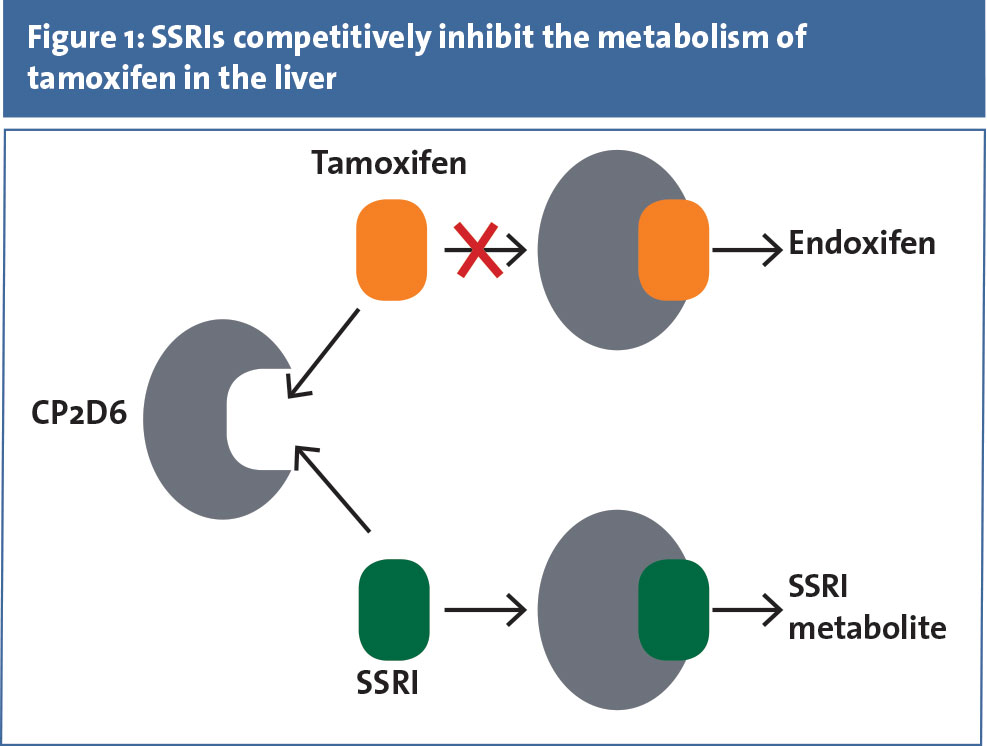
Tamoxifen has been used for four decades to treat oestrogen receptor-positive breast cancer6 and can be used in conjunction with chemotherapy. Tamoxifen reduces recurrence risk by half, and it reduces the risk of mortality from breast cancer by one-third.4 Tamoxifen is a prodrug that is metabolised by the liver via the cytochrome P450 enzyme system. It is then converted into active metabolites, 4-hydroxytamoxifen and 4-hydroxy-N-desmethyltamoxifen (endoxifen). The conversion of tamoxifen into its active metabolites is catalysed by the cytochrome P450 isoenzyme 2D6 (CYP2D6).4,7 CYP2D6 is involved in the oxidative metabolism in approximately 20% of drugs in clinical use.8
Antidepressants use in breast cancer patients
The prevalence of depressive disorders in breast cancer patients is estimated at up to 25%.4 Although breast cancer patients who suffer from depressive episodes may present with typical symptoms of depression (low mood, anhedonia, insomnia, poor appetite, anergia, poor concentration and poor libido), it is important for clinicians to be aware that they may present with aggravated subjective experience of side-effects from cancer treatments (flashes, cognitive impairment, pain, and sexual dysfunction).3 Somatic symptoms of depression may overlap with the side effects of cancer treatment which may lead to underdiagnosis.9 Depressive symptoms may be a risk factor for poor adherence to cancer treatment.10
Selective serotonin reuptake inhibitors (SSRIs) are typically used as antidepressants to treat clinical depression.11 SSRIs (such as fluoxetine, paroxetine, and sertraline) have been shown to be more effective in treating depression, compared to placebo in women with breast cancer.12,13,14 SSRIs also have inhibitory effects on CYP2D6.15 Paroxetine and fluoxetine, in particular, are potent inhibitors of CYP2D6 compared to other SSRIs 15 (see Figure 1).Although concerns were raised regarding the potential of antidepressants to reduce the effectiveness of tamoxifen through pharmacokinetic interaction, the adverse effects of co-prescribing SSRIs and tamoxifen remained unclear until as recently as 2010.5
(click to enlarge)
The adverse effect of co-prescribing SSRIs and tamoxifen
In 2010, Catherine Kelly and her team published the results of a population-based retrospective cohort study among females in Ontario, Canada, who were commenced on tamoxifen.5 The primary outcome of the study was the risk of death from breast cancer after completion of tamoxifen in those who were co-prescribed SSRIs. The SSRIs included in the study were paroxetine, fluoxetine, sertraline, citalopram, and fluvoxamine.
A total of 2,430 women participated in the primary analysis. Eighty three per cent were started on tamoxifen within one year of breast cancer diagnosis. Paroxetine was the most commonly prescribed SSRI (n = 630, 26%) followed by sertraline (n = 541, 22%), citalopram (n = 467, 19.2%) and venlafaxine (n = 365, 15%), respectively.
Just over a thousand women (n = 1,074, 44%) died by the end of the follow-up period. Researchers found that the use of paroxetine was associated with relative increases of 24% in the risk of death from breast cancer. There was no increased risk of breast cancer mortality found in the other SSRIs. The number needed to treat to harm (NNTh) was 20 women treated with paroxetine for every one additional breast cancer death at five years.5
Guidance for co-prescribing antidepressants and tamoxifen
Assessment and treatment of depressive disorder in breast cancer patients should be tailored to individual need.16 According to the American Psychiatric Association (APA) practice guidelines for treatment of major depressive disorder (MDD), patients with depressive episodes who receive tamoxifen should be treated with an antidepressant that has minimal effect on CYP2D6 metabolisms, such as citalopram, escitalopram, venlafaxine, or desvenlafaxine.11 In general, this can be managed by the primary treating physician. In complex clinical cases, a patient will benefit input from a psychiatrist.
Assessment by a psychiatrist will include history taking with emphasis on current presenting symptoms, how the symptoms impact on function, previous mental health illness, family history, evidence of negative cognition and risk assessment. On mental state examination, the assessor will be looking for any evidence of depressive symptomatology. If an SSRI antidepressant is indicated, the patient should be educated regarding the risk of interaction between SSRI and tamoxifen. A collobarative decision-making approach should be taken when weighing the risks and benefits of commencing antidepressants, and available alternative treatments should also be discussed.
In general, venlafaxine, citalopram and escitalopram remain a good choice for a patient who is on tamoxifen. However, some patients may not tolerate venlafaxine because of its less favourable side effect profile compared to citalopram.17
If a patient is already on a potent inhibitor of CYP2D6 (paroxetine, fluoxetine), in general, it is advisable to switch to another SSRI or a serotonin norepinephrine reuptake inhibitor (SNRI) that has less potential for interaction. Every patient should be educated regarding the risk and a collaborative decision should be made. If the patient is on an SSRI with no significant interaction with CYP2D6, the patient can be assessed as to whether there is an ongoing need to remain on an SSRI. If needed, generally the patient will be left on the same antidepressant.
References
Anderson BO, Yip CH, et al. Guideline implementation for breast healthcare in low-income and middle-income countries: overview of the Breast Health Global Initiative Global Summit 2007. Cancer 2008; 113(8 Suppl): 2221-43
Early Breast Cancer Trialists’ Collaborative Group (EVCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365: 1687-717
Fann JR, Thomas-Rich AM, Katon WJ, et al. Major depression after breast cancer: a review of epidemiology and treatment. Gen Hosp Psychiatry 2008; 30: 112-26
Stearns V, Johnson MD, Rae JM, et al. Active tamoxifen metabolite plasma concentrations after co-administration of tamoxifen and the selective serotonin reuptake inhibitor paroxetine. J Natl Cancer Inst 2003; 95: 1758-64
Kelly CM, Juurlink DN, Gomes T, et al. Selective serotonin reuptake inhibitors and breast cancer mortality in women receiving tamoxifen: a population based cohort study. BMJ 2010; 340: c693
Cole MP, Jones CT, Todd ID. A new anti-oestrogenic agent in late breast cancer. An early clinical appraisal of ICI46474. Br J Cancer 1971; 25: 270-5
Desta Z, Ward BA, Soukhova NV, Flockhart DA. Comprehensive evaluation of tamoxifen sequential biotransformation by the human cytochrome P450 system in vitro: prominent roles for CYP3A and CYP2D6. J Pharmacol Exp Ther 2004; 310: 1062-75
Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metab Rev 2009; 41(2): 89-295.
Spiegel D, Riba M. Psychological aspects of cancer. In: DeVita VT, Lawrence TS, Rosenberg SA, eds. Principles and practice of oncology. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008: 2817–2826
DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment. Arch Intern Med 2000; 160: 2101-2107
Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice guideline for the treatment of patients with major depressive disorder. 3rd ed. Arlington, VA: American Psychiatric Publishing, Inc. 2010
Navari RM, Brenner MC, Wilson MN. Treatment of depressive symptoms in patients with early stage breast cancer undergoing adjuvant therapy. Breast Cancer Res Treat 2008; 112(1): 197-201
Roscoe JA, Morrow GR, Hickok JT, et al. Effect of paroxetine hydrochloride on fatigue and depression in breast cancer patients receiving chemotherapy. Breast Cancer Res Treat. 2005; 89(3): 243-249
Kimmick GG, Lovato J, McQuellon R, et al. Randomised, double-blind, placebo-controlled crossover study of sertraline (Zoloft) for treatment of hot flashes in women with early stage breast cancer taking tamoxifen. Breast J 2006; 12(2): 114-122
Hiemke C, Härtter S. Pharmacokinetics of selective serotonin reuptake inhibitors. Pharmacol Ther 2000; 85(1): 11-28
Agarwal P, Riba MD. Tailoring depression treatment for women with breast cancer. Current psychiatry 2010; 9(11): 39-48
Smith D, Dempster C, Glanville J, et al. Efficacy and tolerability of venlafaxine compared with selective serotonin reuptake inhibitors and other antidepressants: a meta-analysis. Br J Psychiatry 2002; 180: 396-404
 (click to enlarge)
(click to enlarge)