Ireland's first national health outcomes prostate cancer registry will ultimately improve treatment regimes, patient care and quality of life
Dr Ray McDermott, Consultant Medical Oncologist, Tallaght Hospital, Dublin, Mr David Galvin, Consultant Urologist, St Vincent’s and the Mater Hospitals, Dublin, Prof Linda Sharp, Professor of Cancer Epidemiology, Newcastle University, UK, Dr Frank Sullivan, Director of the Prostate Cancer Institute and Consultant Radiation Oncologist, Galway Clinic, Galway and Ms Áine Murphy, Irish Prostate Cancer Outcomes Research Project Manager, Molecular Medicine Ireland, Dublin
Men in Ireland now have a one-in-seven chance of developing prostate cancer, with 3,384 men diagnosed with prostate cancer in Ireland in 2012.1 Prostate cancer is a significant clinical problem in Ireland: incidence rates here are the third highest in Europe2 and over 500 Irish men die of advanced prostate cancer each year.1
The 2006 Strategy for Cancer Control in Ireland specifically highlighted a deficit in epidemiological and health services research in cancer. A lack of information about prostate cancer patients and their care may negatively impact clinical outcomes for prostate cancer patients. Clinicians are unable to inform patients of their expected clinical outcomes with any accuracy as no data currently exists beyond overall and cancer-specific survival. Information is lacking on key intermediate clinical outcomes such as risk of recurrence or rates of treatment failure.
Recent population-based studies have investigated men’s functional wellbeing and health-related quality of life as well as treatment side-effects3,4,5 but there is little robust longitudinal data evaluating men’s experiences from diagnosis and throughout their treatments.
Novel agents have been developed for the treatment of advanced prostate cancer,6 however, the challenge remains to collect data that will inform clinicians on the most effective treatment regimes to improve progression-free survival and overall survival for metastatic prostate cancer patients. In order to address these issues, the Irish Prostate Cancer Outcomes Research study (IPCORS) is establishing a national registry to capture high-quality information about newly diagnosed prostate cancer patients. The registry will collect clinical data as well as patient-reported outcome measurements (PROMs) from the time of diagnosis and throughout their treatments.
The registry will generate robust data on a range of important clinical outcomes of men with prostate cancer and assess processes, consistency and quality of prostate cancer care. By providing evidence-based data and recommendations to clinicians, hospitals, decision-makers and the National Cancer Control Programme (NCCP), the registry will promote equity in access to services and improvements in care nationally.
By bringing together, for the first time, data on clinical and patient-reported outcomes that have been collected over time and fostering research on such data, the registry will ultimately lead to the improvement of treatment regimes, patient care and maximise quality of life for men diagnosed with prostate cancer in the Republic of Ireland.
(click to enlarge)
Participating hospitals
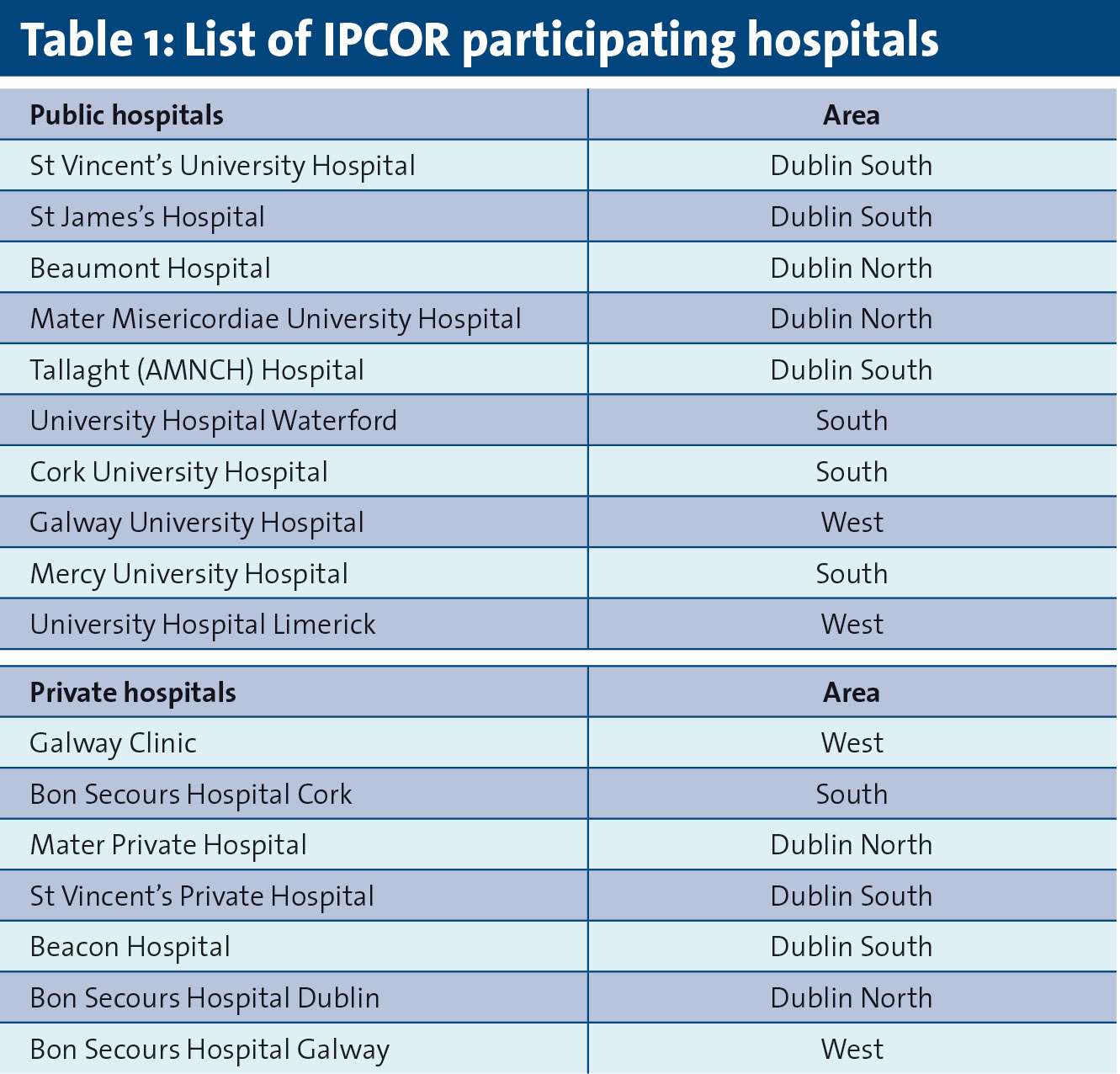
The IPCOR study will identify patients in and collect clinical data from 17 hospitals that diagnose over 88% of prostate cancer cases in the Republic of Ireland. The study will follow these men over time as they undergo treatment for prostate cancer. The study has received ethical approval from the relevant ethics committees.(See Table 1 for list of participating hospitals)
(click to enlarge)
Clinician recruitment
For the IPCOR study to succeed, it is essential to have the support and commitment of prostate cancer treating clinicians. IPCOR has recruited urologists, medical oncologists and radiation oncologists who have agreed to IPCOR collecting clinical data on their prostate cancer patients and contacting their patients to seek consent from them to take part in the PROMs components of the study. Clinicians who participate in the study will receive an annual report of their patients’ outcomes.
Patient identification
IPCOR represents an extension of the present registration and data collection system at the National Cancer Registry (NCR). IPCOR research officers will be employed by the NCR to identify patients and to collect the data required for IPCOR.
All men who have been newly diagnosed with prostate cancer in the 17 participating hospitals will be eligible for inclusion in the IPCOR study and will be identified through a rapid case ascertainment system which will be implemented in each hospital. The first patient-reported outcome data will be collected in the interval between diagnosis and commencement of treatment to obtain a baseline of men’s quality of life.
Due to this tight timeframe for data collection, IPCOR will establish mechanisms to ensure rapid routes for identification of men eligible to take part in the study. For example, currently approximately one-third of men with prostate cancer are diagnosed through the NCCP designated cancer centres either via their Rapid Access Prostate Clinics (RAPC) or directly through symptomatic services and/or urology clinics.
IPCOR research officers will set-up procedures to access lists from the RAPC and from weekly multidisciplinary team (MDT) meetings. Following current NCR processes, the research officers will access other data sources, eg. hospital patient administration systems, radiotherapy clinic records, chemotherapy clinic records, and local HIPE (hospital inpatient episode) records to identify and capture any missed cases.
Following their diagnosis, men will be sent written information about the study and asked to consent to the sharing of patient and hospital-level data within the IPCOR project team, participating in the patient-reported outcomes components of the study by filling in quality of life questionnaires annually, linking their clinical and PROMs data to their biological specimens and for the use of their biological specimens, including those taken for diagnostic tests, in future ethically approved research studies. Each patient will be assigned a unique IPCOR registration number at the time of initial identification which will link their data and their biological specimens.
Data collection
Clinical data
The NCR will extend their current database to incorporate the additional data items and the clinical follow-up of patients that IPCOR will collect. Utilising the NCR model of data collection ensures that IPCOR will create a population-based database with a high degree of completeness.
When potentially eligible cases are ascertained, the research officers will register the case and collect basic demographic and clinical information (including name, address, date of birth, grade, PSA result). The research officers will subsequently collect data on disease stage, morphology, and treatments received in the first year post-diagnosis (surgical procedures, radiotherapy, chemotherapy and hormonal treatment), hospitals attended and treating clinicians from the medical record and other sources such as radiotherapy and oncology clinic records. The patient’s IPCOR registration number will be used to track patients over time.
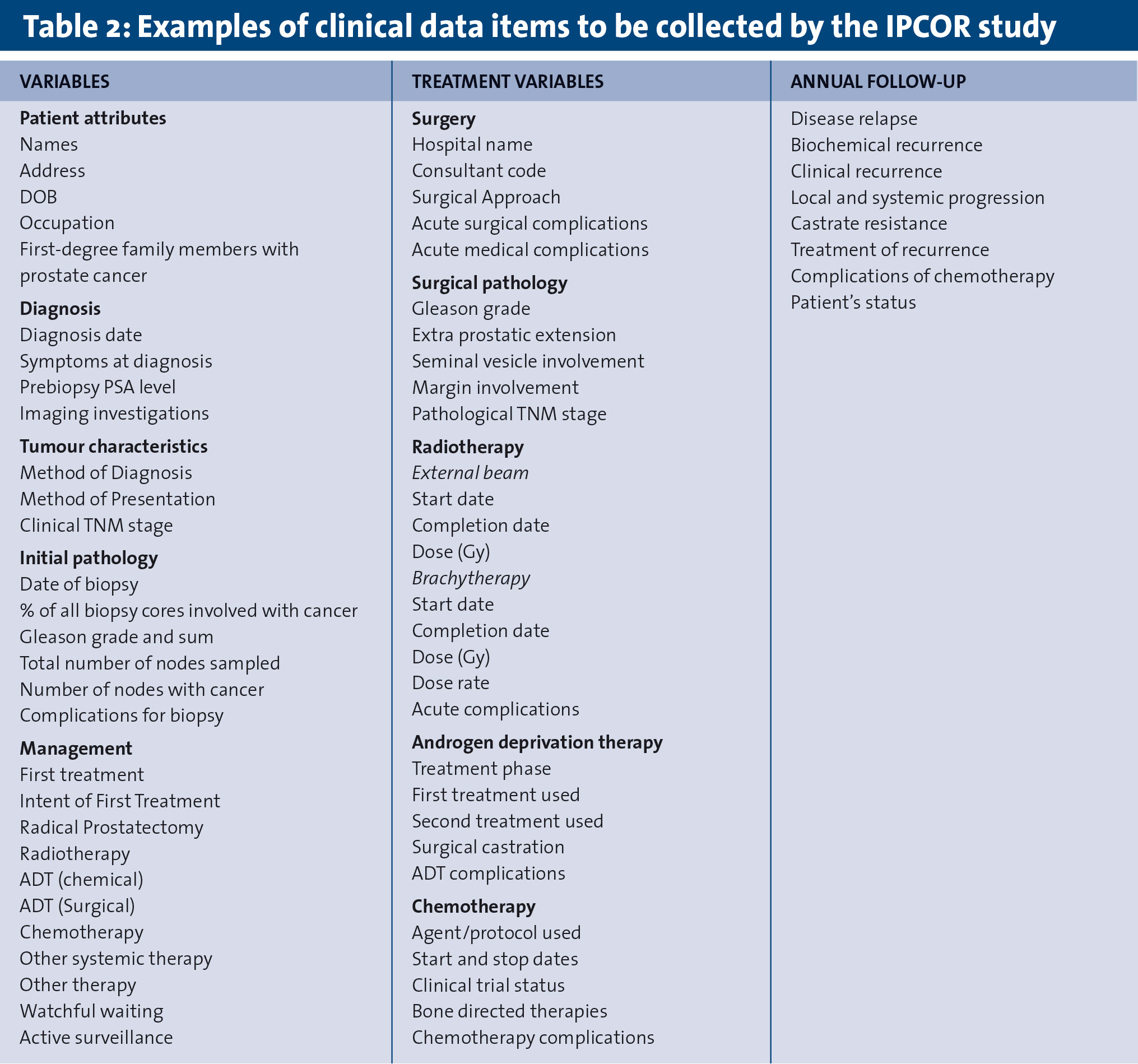
A unique aspect of the IPCOR study is the active follow-up of patients on a yearly basis by the research officers. The research officers will collect information on additional treatments received, treatment failure, recurrence, metastases etc. This will involve accessing various data sources and liaising with GPs. The NCR routinely links registrations with death certificates provided by the Central Statistics Office; this process will be used to provide robust information on date and cause of death. (Table 2. Examples of clinical data items to be collected by the IPCOR study)
(click to enlarge)
Patient-reported outcomes measurement (PROMs) data
IPCOR is committed to better understanding the patient experience throughout the disease course and will collect patient-reported outcomes at baseline and annually thereafter. Validated questionnaires will be used to collect general and disease-specific quality of life. The International Consortium of Health Outcome Measurement (ICHOM) Prostate Cancer Working Group has determined that the Expanded Prostate Cancer Index Composite (EPIC-26) should be used to assess prostate cancer-specific effects on quality of life.
IPCOR will also utilise EORTC QLQ-C30 and EuroQol EQ-5D-5L to assess general health-related quality of life. PROMs data will be collected using postal questionnaires and a web-based data collection system. In the future, particular clinical cohorts of men may be invited to complete questionnaires relating to areas of research interest such as treatment decision-making and service satisfaction.
Risk stratification
The Cancer of the Prostate Risk Assessment (CAPRA) model will be used to stratify patients according to their risk of metastasis, cancer-specific mortality, and overall mortality7 and patient outcomes will then be analysed.
The CAPRA score is calculated using points assigned to: age at diagnosis, PSA at diagnosis, Gleason score of the biopsy, clinical stage and per cent of biopsy cores involved with cancer.8 A CAPRA score is valid across multiple treatment approaches such as radical prostatectomy, radiation therapy (brachytherapy or external-beam), primary androgen deprivation therapy or active surveillance.7
Reporting outcomes
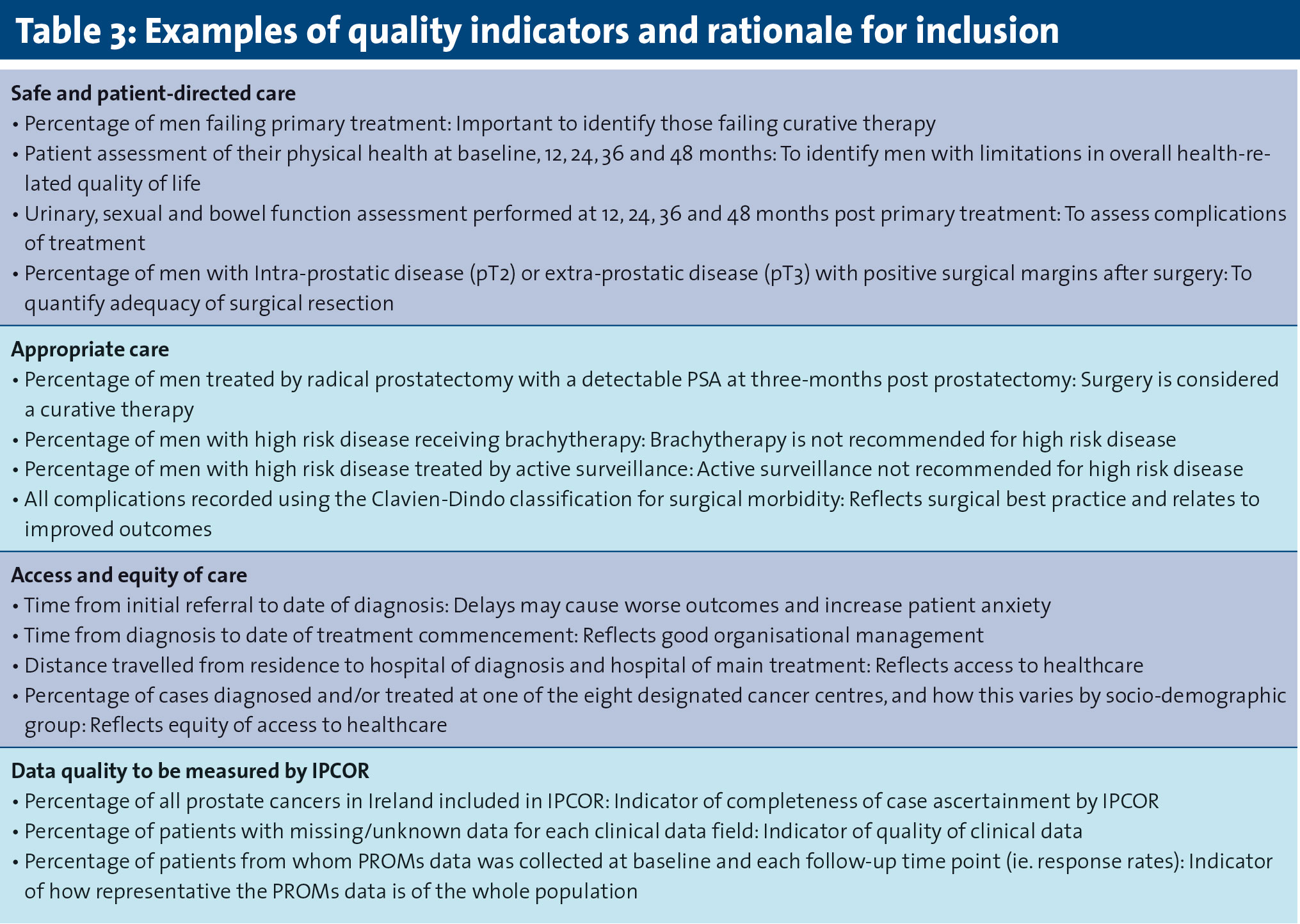
The public IPCOR annual report will contain outcomes for prostate cancer patients at a national level while clinical reports will be aimed at clinicians and decision-makers, such as the NCCP, with detailed reporting on quality indicators which can facilitate decision-making and drive service improvements. (Table 3. Examples of quality indicators and rationale for inclusion).
(click to enlarge)
Data access
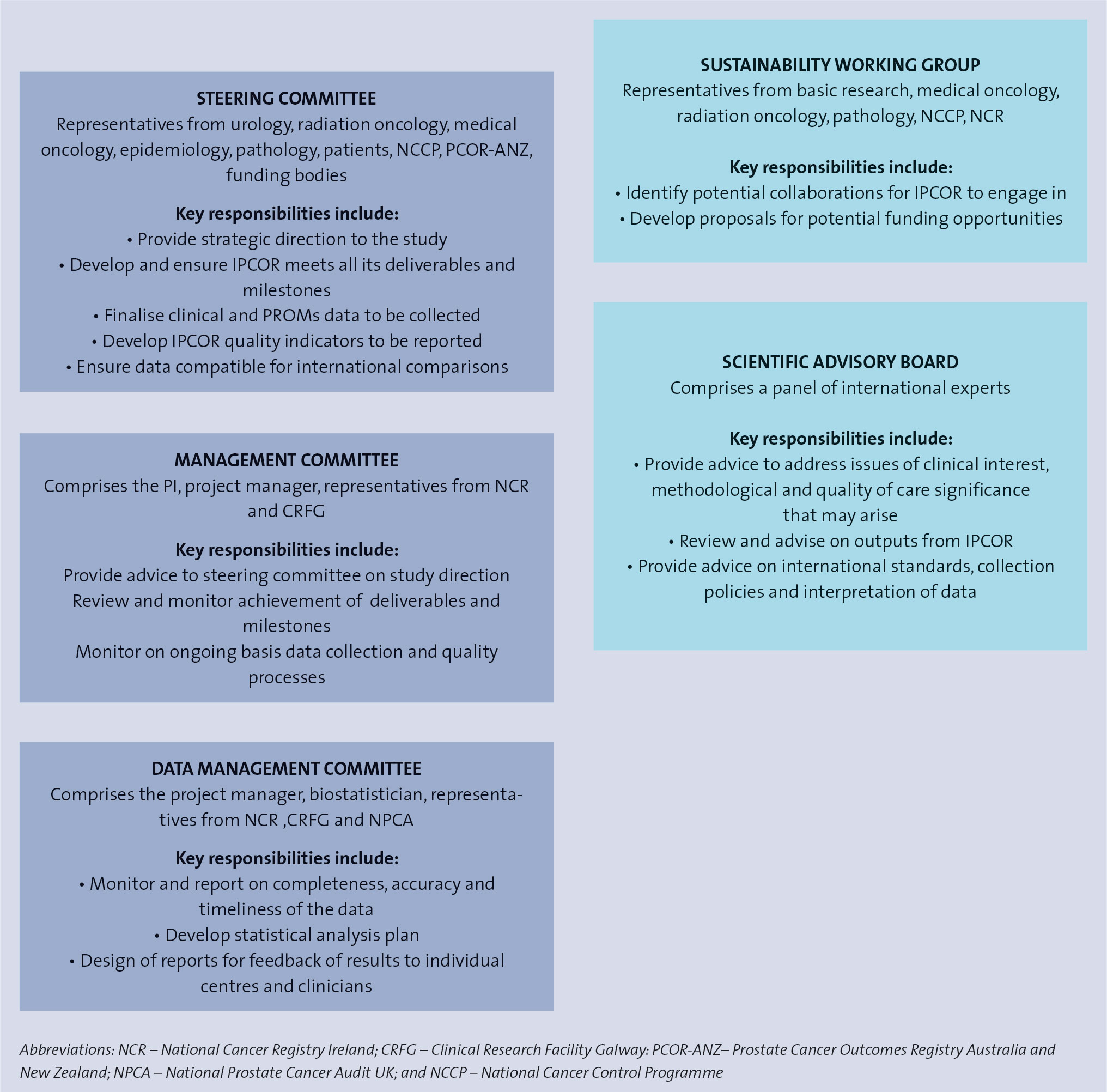
Information contained within the IPCOR registry will routinely be used by IPCOR personnel to assess quality of care provided to men with prostate cancer and foster research leading to improvements in care and survival. Cancer researchers may request access to de-identified IPCOR data. Data requests will be reviewed by the IPCOR Steering Committee and must be accompanied by relevant ethics committee certification.
Discussion
The IPCOR study is developing the first national health outcomes prostate cancer registry that will follow patients over time and provide a comprehensive overview of men’s prostate cancer journey through the health system in the Republic of Ireland. The registry will be used to monitor quality, benchmark outcomes and aid clinical research. It is hoped that this high quality disease registry will enable the identification of best practices and improve outcomes through the use of ‘real-life’ data.
The registry data will be utilised to identify treatment patterns and the optimal sequences or combinations of treatment regimens for patients with local and advanced prostate cancer in order to maximise positive outcomes for these patients. Randomised prospective trials to test all potential combinations or sequences of treatment are not feasible, thus the IPCOR registry provides a valuable resource for comparative effectiveness research using ‘real-life’ data to determine optimal treatment sequences and their outcomes.
The registry will provide a better understanding of the variation in care and treatment of prostate cancer across the country and between the public and private healthcare sectors. Registry data will help in the identification of relevant population cohorts for future clinical trials and diagnostic testing. The availability of this information could positively influence the pharmaceutical industry’s selection decisions and lead to increased inclusion of Irish patients in clinical trials.
The clinical and PROMs data in the registry will be linked to men’s diagnostic biological samples which have been consented for use in future ethically approved research. The registry will promote the use of the data and biological samples by researchers to maximise the registry’s potential and facilitate studies which investigate areas of oncology, particularly the identification of biomarkers that are predictive for response and resistance to treatments.
The IPCOR study will be a significant contributor to international prostate cancer research. IPCOR is collecting both clinical and PROMs data as recommended by the ICHOM Prostate Cancer Working Group and has aligned its data collection with that currently being carried out by the Prostate Cancer Outcomes Registry in Australia and New Zealand and the National Prostate Cancer Audit in the UK (England and Wales). These studies represent a unique opportunity to benchmark prostate cancer care internationally and promote improvements in care for patients with prostate cancer.
The IPCOR registry represents a novel model of translational research for both local and advanced prostate cancer care by improving our knowledge of patterns and quality of care; monitoring equity of access to treatments and care; discovery of optimal therapeutic sequences and improving compliance with best practice guidelines for prostate cancer treatment. The analysis of PROMs data will inform the development and implementation of strategies and supports to help men live better after prostate cancer. The IPCOR infrastructure provides a template for the establishment of enhanced cancer registries in Ireland.
Acknowledgements: This work is funded by the Irish Cancer Society Irish Prostate Cancer Outcomes Research Project, IPCOR14GAL, supported by the Movember Foundation. Any opinions, findings, conclusions or recommendations expressed are those of the authors and not necessarily those of the Irish Cancer Society or Movember Foundation. The authors would like to thank the IPCOR Steering Committee for reviewing and approving this manuscript.
References
Cancer Factsheet – Prostate. National Cancer Registry Ireland. Cork: 2015
Prostate Cancer Factsheet: Estimated incidence, mortality and prevalence. International Agency for Research on Cancer, World Health Organisation. France: 2012
Sharp L, O’Leary E, Kinnear H, et al. Cancer-related symptoms predict psychological wellbeing among prostate cancer survivors: results from the PiCTure study. Psycho-oncology 2015; DOI: 10.1002/pon.3909
Drummond FJ, Kinnear H, O’Leary E, et al. Long-term health-related quality of life of prostate cancer survivors varies by primary treatment. Results from the PiCTure (Prostate Cancer Treatment, your experience) study. J Cancer Surviv 2015; 9(2): 361-72
Gavin AT, Drummond FJ, Donnelly C, et al. Patient-reported ‘ever had’ and ‘current’ long-term physical symptoms after prostate cancer treatments. BJU Int 2015; 116(3): 397-406
Osanto S, Van Poppel H. Emerging novel therapies for advanced prostate cancer. Ther Adv Urol 2012; 4(1): 3-12
Cooperberg MR, Broering JM, Carroll PR. Risk assessment for prostate cancer metastasis and mortality at the time of diagnosis. J Natl Cancer Inst 2009; 101(12): 878-87
Cooperberg MR, Pasta DJ, Elkin EP, et al. The UCSF Cancer of the Prostate Risk Assessment (CAPRA) Score: a straightforward and reliable pre-operative predictor of disease recurrence after radical prostatectomy. J Urol 2005; 173(6): 1938-1942
 (click to enlarge)
(click to enlarge)