Recent decades have witnessed major changes in lifestyle that have led to steady increases in average body weight in both developed and less developed countries.1 A person whose weight is above the normal range is referred to as being overweight. This is determined by calculating the body mass index (BMI, defined as weight in kilograms divided by height in metres squared). Overweight is defined as a BMI of 25-29.9, obesity as a BMI > 30 and severe obesity is defined as a BMI > 40. Obesity is more prevalent in high-income countries, such as the US and the UK, than in low-income countries, such as Brazil and China. It is currently estimated that approximately 50% of men and 35% of women in Europe are overweight or obese.1
(click to enlarge)
The high prevalence of obesity in developed countries can be explained, in part, by a lifestyle characterised by over-consumption of energy combined with low physical activity.1 Lifestyle changes due to economic, social and technological advances have resulted in increased automation and computerisation in the workplace and in the home, a reduction in walking and cycling for transport, a decrease in recreational exercise and an increase in sedentary leisure-time occupations.1
Other influences on the increase in obesity are environmental and include increased marketing and advertising of food products, increased portion sizes and increased accessibility and availability of food.2,3
Effects of obesity
The morbidity and mortality associated with being overweight or obese have been known to the medical profession for more than 2,000 years.4-7 This association between BMI and cause-specific mortality was recently reiterated in the Prospective Studies Collaboration analysis where, in the upper BMI range, each 5kg/m2 increase in BMI was shown to be associated with a significant increase in mortality from ischaemic heart disease, stroke, diabetes and respiratory disease.8 Obesity also has important social, economic and psychological consequences.9-14
Epidemiological studies are now providing evidence for a link between increased body weight and a higher risk of developing cancer. In recent years there has been an improved understanding of the impact of obesity on the development of a number of cancer types, with current estimates of overweight and obesity causing approximately 20% of all cancer cases.15
A US prospective cohort study of over 900,000 men and women has claimed that overweight and obesity in the US could account for 14% of all cancer deaths in men and 20% of those in women.16 It is also estimated that the total health burden of overweight and obesity may now exceed that for cigarette smoking.17
Obesity and Ireland
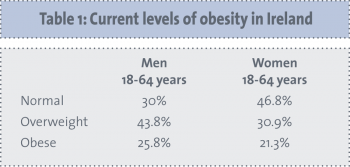
Obesity remains a major public health problem in Ireland. A 2011 Irish Nutrition Survey performed by the Irish Universities Nutrition Alliance has revealed that, among 18-64-year-olds in Ireland, a total of 24% are obese (men 26%, women 21%) and 37% are overweight (men 44%, women 31%).18
Within this age group, the percentage of the population classified as overweight or obese was shown to be increasing with advancing age. In those aged 65 and over, 49% of women and 59% of men are overweight and 24% of women and 25% of men are obese.18 The prevalence of obesity in 18-64-year-old adults has risen significantly since 1990, from 8% to 26% in men and from 13% to 21% in women, with the greatest increase observed in men aged 51-64 years.18
Obesity is also a common problem among children, with overweight and obesity now classed the most common childhood disorder in Europe.19 Over 20% of Irish 5-12-year-olds are now classified as overweight or obese,20 and overweight children tend to become overweight adults.21
It has been estimated that ingestion of 5% more calories than expended may result in 5kg of adipose tissue or body fat accumulation in one year.22 The cost of treating obesity in Ireland has been estimated at €0.4 billion, and approximately 2,000 premature deaths annually in Ireland have been attributed to obesity.23
Increased cancer rates
Parallel with this increase in obesity, we have witnessed a dramatic increase in the incidence of cancer in Ireland. Overall, cancer incidence in Ireland is high compared to other European countries, with females ranked second and males ranked fourth overall. International comparisons show that mortality rates for Irish men compare quite favourably with our European neighbours, but the incidence and mortality rates for women are among the highest in Europe.24
Oesophageal cancer
Obesity has been strongly implicated in the pathogenesis of oesophageal adenocarcinoma, with overweight and obese men and women reported to be twice as likely as those of a healthy weight to develop oesophageal adenocarcinoma.25-29 A smaller increased risk has been found for gastric cancer of the cardia.28‑29 A BMI > 30kg/m2 has been shown in a meta-analysis to be associated with a relative risk of 3.0 for developing oesophageal adenocarcinoma.30 This represents a higher association than for any other cancer. Evidence suggests that insulin and the insulin-like growth factor (IGF) axis play an important role in mediating obesity-associated malignancy.31 Studies have also highlighted an association between IGF with visceral obesity and a potential impact on the biology of oesophageal adenocarcinoma.32
Breast cancer
The first evidence that heavier women are at increased risk of breast cancer was obtained in the 1970s. The effect of obesity on breast cancer has been reported to depend on a woman’s menopausal status. Before menopause, obese women have a lower risk of developing breast cancer than do women of a healthy weight.33-36 After the menopause, obese women have a 1.5 times increased risk of developing breast cancer than women of a healthy weight.33,34,36,37 Indeed, weight gain during adult life is also consistently associated with increased risk of postmenopausal breast cancer.38-42
The increased risk of developing breast cancer in obese women is believed to be due to increased levels of oestrogen.43 It is also reported that breast cancer is more likely to be detected at a later stage in obese versus lean women and that overweight and obese women are less likely to be screened for breast cancer with mammograms.35,44
Colorectal cancer
Colon cancer has also been shown to occur more frequently in people who are obese than in those of a healthy weight.25,45‑49 The risk of colon cancer increases by 25% in overweight men and by approximately 50% in obese men.46,49-51 The relationship between BMI and colon cancer risk in women, however, has been found to be weaker or absent.46,50,52 Studies have reported a stronger association for colon than for rectal cancer and the distal colon appears more affected than the proximal colon.1,46,53,54
Endometrial cancer
Obese women have two to four times greater risk of developing endometrial cancer than women of a healthy weight, regardless of menopausal status, and this risk increases linearly with increases in BMI above 25.1,25,55-58
Renal cell cancer
Studies have consistently found a link between renal cell carcinoma and obesity in women, with some studies reporting the risk among obese women to be two to four times the risk of women of a healthy weight.25,59-62 Results of studies involving men have been more variable, ranging from an association similar to that seen in women, to a weak association, to no association at all.59,60,62
Pancreatic cancer
Two large prospective studies in the US support a link between obesity and pancreatic cancer and a meta-analysis has shown a 19% risk increase of pancreatic cancer for obese individuals.63-66
Other cancer types
An increased risk of gallbladder cancer has been found to be associated with obesity, especially among women.67-69 This may be due to the higher frequency of gallstones in obese individuals, which are considered a strong risk factor for gallbladder cancer.67‑69 Some studies report an increased risk of ovarian cancer among obese women, whereas others have found no association.70-74 Most studies on prostate cancer conclude that there is no association between prostate cancer and obesity.1,25,75-77
Studies evaluating the relationship between hepatic cancer and obesity have been inconsistent, with some studies reporting a link and others not.78,79 Lung cancer risk is shown to be inversely associated with BMI, but this association seems to be confounded by cigarette smoking history.25 Data are scarce on the relationship between haematopoietic cancers and BMI, and the findings have not been consistent.16
Mechanism of altered cancer risk
The mechanisms by which weight, diet and physical activity influence tumour formation and progression are not completely understood. As the pathophysiology of obesity is complex and multisystemic, it is unlikely that ‘one size fits all’. A number of putative processes have therefore been proposed.15 The mechanisms underlying the effect of obesity and weight change vary by tumour site. In part, these associations with cancer risk may be explained by alterations in the metabolism of endogenous hormones, including sex steroids, insulin, and insulin-like growth factors, which can lead to distortion of the normal balance between cell proliferation, differentiation and apoptosis.1 Female hormones would appear to be implicated in breast and endometrial cancer, but have much less impact on other cancers. Insulin may be the drive behind colon cancer and inflammation is thought to drive other malignancies.15
Effect of obesity on survival
For both men and women increasing BMI has been shown to be associated with higher death rates from a variety of cancers, including oesophageal cancer, colorectal cancer, pancreatic cancer and renal cell cancer.16
Obese women have been shown to be at increased risk of dying from cervical cancer, ovarian, endometrial and postmenopausal breast cancer compared with lean women.16,25,33-35,80,81 Obese men are also at increased risk of death from stomach cancer.16 Although prostate cancer is not associated with obesity there is emerging evidence that higher risk of death from prostate cancer has been shown in obese men.82
Weight control and physical activity
A recent review of the current evidence pertaining to dietary factors and cancer incidence and progression, has concluded that despite epidemiological evidence suggesting a link between dietary factors and cancer development, confounding evidence such as obesity, physical activity and the sheer variety of bio-active compounds in a normal diet, pose a great challenge to the study of mechanisms linking diet and cancer.83
While cancer incidence is clearly increased in obese individuals, it is unclear whether weight loss decreases cancer incidence. Nonetheless, avoidance of weight gain should become one of the mainstays of chronic disease prevention in modern societies.
Studies have shown that many adults are not aware of the link between obesity and cancer.84 A Canadian study has reported that only 31% of Canadians thought that being overweight was a risk factor for cancer and only 28% thought that lack of exercise was linked to cancer. In contrast, the majority of Canadians (83% and 78%) associated overweight with heart disease and diabetes, respectively.84
The best way to achieve a healthy body weight is by balancing energy expenditure with energy intake. Excess weight can be reduced through increasing physical activity and by restricting calorific intake. The association between physical activity and decreased risk for breast cancer and colon cancer has been demonstrated across levels of obesity.85-87 Limited evidence suggests that increased physical activity offers some protection against endometrial and prostate cancer.15,47,88,89
Several mechanisms have been proposed to explain the possible effect of physical activity, including: 90-92
Reduction in circulating levels of insulin, hormones and other growth factors
Impact on prostaglandin levels
Improved immune function
Altered bile metabolism.
Only a limited number of studies have addressed this issue and the results are difficult to interpret due to a lack of, or insufficient, information on the cause of the weight loss.1 Thus, the optimal duration, intensity and frequency of physical activity that may afford cancer protection is unknown.
(click to enlarge)
Conclusion and future directions
Obesity remains a major public health problem on a national as well as on an international basis. Overweight and obesity are the most important known avoidable causes of cancer after tobacco smoking. The burden of obesity on society continues to increase and warrants closer attention by clinicians. It is estimated that 90,000 cancer deaths could be prevented each year in the US if men and women could maintain normal weight.16
A better understanding of the mechanisms that link obesity to cancer may help in the development of targets for intervention. Drugs currently under development that inhibit IGF-1 receptor function may prove useful targeted therapies for certain cancers, including adenocarcinoma of the oesophagus, which express IGF-1 receptor.32
The problem of childhood obesity must be viewed on a global level. The World Health Organization has taken a strong stance on the prevention of obesity, underscoring its global health threat.93
The challenge for providers is to engage the patient in understanding the importance of weight control and increased physical activity. Concerted effort and substantial investment on the part of policy makers, educators and clinicians must be employed in order to achieve this important goal.
References
Bianchini F, Kaaks R, Vainio H. Overweight, obesity, and cancer risk. Lancet Oncology 2002; 3(9): 565-574.
International Obesity Taskforce and European Association for the Study of Obesity. Obesity in Europe – The Case for Action. 2002.
European Heart Network. The Marketing of Unhealthy Food to Children in Europe. A report of Phase 1 of the ‘Children, obesity and associated avoidable chronic diseases’ Project. Brussels, 2005.
Alpert MA, Hashimi MW. Obesity and the heart. Am J Med Sci 1993; 306(2): 117-123.
Sjöström LV. Morbidity of severely obese subjects. Am J Clin Nutr 1992; 55(2 Suppl): 508S.
Bray, GA .Topography of body fat. Adv Endocrinol Metab. 1994; 5: 297.
Sjöström LV. Mortality of severely obese subjects. Am J Clin Nutr 1992; 55(2 Suppl): 516S.
Prospective Studies Collaboration, Whitlock G, Lewington S, et al. Body-mass index and cause-specific mortality in 900,000 adults: collaborative analyses of 57 prospective studies. Lancet 2009; 373(9669): 1083-1096.
Wadden TA, Stunkard AJ. Social and psychological consequences of obesity. Ann Intern Med 1985; 103(6 Pt 2): 1062-1067.
Gortmaker SL, Must A, Perrin JM, et al. Social and economic consequences of overweight in adolescence and young adulthood. NEJM 1993; 329: 1008-1012.
Miller TM, Coffman JG, Linke RA. Survey on body image, weight, and diet of college students. J Am Diet Assoc 1980; 77: 561-566.
Dawson DA. Ethnic differences in female overweight: data from the 1985 National Health Interview Survey. Am J Public Health 1988; 78: 1326-1329.
Caldwell MB, Brownell KD, Wilfley DE. Relationship of weight, body dissatisfaction, and self-esteem in African American and white female dieters. Int J Eat Disord 1997; 22: 127-130.
Stevens J, Kumanyika SK, Keil JE. Attitudes toward body size and dieting: differences between elderly black and white women. Am J Public Health 1994; 84: 1322-1325.
Wolin K, Carson K, Colditz G. Obesity and cancer. The Oncologist 2010; 15 :556-565.
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of US adults. NEJM 2003; 348(17): 1625-1638.
Stewart ST, Cutler DM, Rosen AB. Forecasting the effects of obesity and smoking on U.S. life expectancy. NEJM 2009; 361: 2252-2260.
World Health Organisation. Fact sheet on Obesity and Overweight. 2003.
Irish Universities Nutrition Alliance. National Children’s Food Survey. 2006. Available from www.iuna.net
Serdula MK, Ivery D, Coates RJ, et al. Do obese children become obese adults? A review of the literature. Prev Med 1993; 22(2): 167-77.
Klein S, Wadden T, Sugerman HJ. AGA technical review on obesity. Gastroenterol 2002; 123(3): 882-932.
National Taskforce on Obesity. Obesity – the Policy Challenges. Department of Health and Children. Dublin: Government Publications Office, 2005.
Lung Cancer Incidence, Mortality, Treatment and Survival in the Republic of Ireland: 1994-2008. National Cancer Registry, 2011. Available from www.ncri.ie/pubs/pubfiles/LungCancer2011.pdf
Vainio H, Bianchini F. IARC Handbook of cancer prevention. Volume 6: Weight control and physical activity. Lyon, France: IARC Press, 2002.
Lagergren J, Bergström R, Nyrén O. Association between body mass and adenocarcinoma of the esophagus and gastric cardia. Ann Internal Med 1999; 130(11): 883-890.
Brown LM, Swanson CA, Gridley G, et al. Adenocarcinoma of the esophagus: Role of obesity and diet. J Nat Cancer Inst 1995; 87(2): 104-109.
Chow WH, Blot WJ, Vaughan TL, et al. Body mass index and risk of adenocarcinomas of the esophagus and gastric cardia. J Nat Cancer Inst 1998; 90(2): 150-155.
Li SD, Mobarhan S. Association between body mass index and adenocarcinoma of the esophagus and gastric cardia. Nutrition Reviews 2000; 58(2 Pt 1): 54-56.
Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer 2004; 4(8): 579-91.
Donohoe CL, Doyle SL, Reynolds JV Visceral adiposity, insulin resistance and cancer risk. Diabetol Metab Syndr 2011 Jun 22; 3: 12.
Donohoe CL, Doyle SL, McGarrigle S, et al. Role of the insulin-like growth factor 1 axis and visceral adiposity in oesophageal adenocarcinoma. Br J Surg 2012; 99(3): 387-396.
Trentham-Dietz A, Newcomb PA, Storer BE, et al. Body size and risk of breast cancer. Am J Epidemiol 1997; 145(11): 1011-1019.
Huang Z, Hankinson SE, Cloditz GA, et al. Dual effects of weight and weight gain on breast cancer risk. JAMA 1997; 278(17): 1407-1411.
Cui Y, Whiteman MK, Flaws JA, et al. Body mass and stage of breast cancer at diagnosis. Int J Cancer 2002; 98(2): 279-283.
Friedenreich CM. Review of anthropometric factors and breast cancer risk. Eur J Cancer Prev 2001; 10(1): 15-32.
Yoo KY, Tajima K, Park S, et al. Postmenopausal obesity as a breast cancer risk factor according to estrogen and progesterone receptor status (Japan). Cancer Letters 2001; 167(1): 57-63.
Brinton LA, Swanson CA. Height and weight at various ages and risk of breast cancer. Ann Epidemiol 1992; 2: 597-609.
Magnusson C, Baron J, Persson I, et al. Body size in different periods of life and breast cancer risk in post-menopausal women.Int J Cancer 1998; 76: 29-34.
Huang Z, Hankinson SE, Colditz GA, et al. Dual effects of weight and weight gain on breast cancer risk. JAMA 1997; 278: 1407-1411.
Tretli S. Height and weight in relation to breast cancer morbidity and mortality. A prospective study of 570,000 women in Norway. Int J Cancer 1989; 44(1): 23-30.
Petrelli JM, Calle EE, Rodriguez C, Thun MJ. Body mass index, height, and postmenopausal breast cancer mortality in a prospective cohort of US women. Cancer Causes and Control 2002; 13(4): 325-332.
Toniolo PG, Levitz M, Zeleniuch-Jacquotte A, et al. A prospective study of endogenous estrogens and breast cancer in postmenopausal women. J Nat Cancer Inst 1995; 87(3): 190-197.
Wee C, McCarthy E, Davis R, Phillips R. Screening for Cervical and Breast Cancer: Is Obesity an Unrecognized Barrier to Preventive Care? Ann Intern Med 2000; 132: 697-704.
Ford ES. Body mass index and colon cancer in a national sample of adult U.S. men and women. Am J Epidemiol 1999; 150(4): 390-398.
Caan BJ, Coates AO, Slattery ML, et al. Body size and the risk of colon cancer in a large case-control study. Int J Obesity Related Metabolic Dis 1998; 22(2): 178-184.
Kono S, Handa K, Kayabuchi H, et al. Obesity, weight gain and risk of colon adenomas in Japanese men. Japanese J Cancer Res 1999; 90(8): 805-811.
Shike M. Body weight and colon cancer. Am J Clin Nutrition 1996; 63(3 Suppl): 442S-444S.
Giacosa A, Franceschi S, La Vecchia C, et al. Energy intake, overweight, physical exercise and colorectal cancer risk. Eur J Cancer Prev 1999; 8 Suppl 1: S53-S60.
Murphy TK, Calle EE, Rodriguez C, et al. Body mass index and colon cancer mortality in a large prospective study. Am J Epidemiol 2000; 152(9): 847-854.
Moghaddam, AA, et al. Obesity and Risk of Colorectal Cancer: A Meta-analysis of 31 Studies with 70,000 Events. Cancer Epidemiol Biomarkers Prev 2007; 16(12): 2533-2547.
Phillips RL, Snowdon DA. Dietary relationships with fatal colorectal cancer among Seventh-Day Adventists. J Nat Cancer Inst 1985; 74(2): 307-317.
Gerhardsson de Verdier M, Hagman U, Steineck G, et al. Diet, body mass and colorectal cancer: a case-referent study in Stockholm. Int J Cancer 1990; 46: 832-838.
Martinez ME, Giovannucci E, Spiegelman D, et al. Leisure-time physical activity, body size, and colon cancer in women. Nurses’ Health Study Research Group. J Natl Cancer Inst 1997; 89: 948-955.
Salazar-Martínez E, Lazcano-Ponce EC, Lira-Lira GG, et al. Case-control study of diabetes, obesity, physical activity and risk of endometrial cancer among Mexican women. Cancer Causes and Control 2000; 11(8): 707-711.
Shoff SM, Newcomb PA. Diabetes, body size, and risk of endometrial cancer. Am J Epidemiol 1998; 148(3): 234-240.
Weiderpass E, Persson I, Adami HO, et al. Body size in different periods of life, diabetes mellitus, hypertension, and risk of postmenopausal endometrial cancer (Sweden). Cancer Causes and Control 2000; 11(2): 185-192.
Goodman MT, Hankin JH, Wilkens LR, et al. Diet, body size, physical activity, and the risk of endometrial cancer. Cancer Res 1997; 57(22): 5077-5085.
Chow WH, McLaughlin JK, Mandel JS, et al. Obesity and risk of renal cell cancer. Cancer Epidemiol Biomarkers and Prevention 1996; 5(1): 17-21.
Yuan JM, Castelao JE, Gago-Domingues M, et al. Hypertension, obesity and their medications in relation to renal cell carcinoma. Br J Cancer 1998; 77(9): 1508-1513.
Lindblad P, Wolk A, Bergstrom R, et al. The role of obesity and weight fluctuations in the etiology of renal cell cancer: A population-based case-control study. Cancer Epidemiol Biomarkers Prevention 1994; 3(8): 631-639.
Mellemgaard A, Lindblad P, Schlenhofer B, et al. Role of weight, height, physical activity, and use of amphetamines. Int J Cancer 1995; 60(3): 350-354.
Silverman DT, Swanson CA, Dridley G, et al. Dietary and nutritional factors and pancreatic cancer: A case-control study based on direct interviews. J Nat Cancer Inst 1998; 90(22): 1710-1719.
Silverman DT. Risk factors for pancreatic cancer: A case-control study based on direct interviews. Teratogenesis, Carcinogenesis, and Mutagenesis 2001; 21(1): 7-25.
Patel, AV, et al., Obesity, recreational physical activity, and risk of pancreatic cancer in a large US Cohort. Cancer Epidemiol Biomarkers Prev 2005. 14(2): 459-466.
Berrington de Gonzalez, A, et al, A meta-analysis of obesity and the risk of pancreatic cancer. Br J Cancer, 2003; 89(3): 519-523.
Lowenfels AB, Maisonneuve P, Boyle P, et al. Epidemiology of gallbladder cancer. Hepato-Gastroenterol 1999; 46(27): 1529-1532.
Moerman CJ, Bueno-de-Mesquita HB. The epidemiology of gallbladder cancer: Lifestyle-related risk factors and limited surgical possibilities for prevention. Hepato-Gastroenterol 1999; 46(27): 1533-1539.
Hartz AJ, Rupley DC, Rimm AA. The association of girth measurements with disease in 32,856 women. Am J Epidemiol 1984; 119(1): 71-80.
Mori M, Nishida T, Sugiyama T, et al. Anthropometric and other risk factors for ovarian cancer in a case-control study. Japanese J Cancer Res 1998; 89(3): 246-253.
Mink PJ, Folsom AR, Sellers TA, Kushi LH. Physical activity, waist-to-hip ratio, and other risk factors for ovarian cancer: A follow-up study of older women. Epidemiol 1996; 7(1): 38-45.
Farrow DC, Weiss NS, Lyon JL, et al. Association of obesity and ovarian cancer in a case-control study. Am J Epidemiol 1989; 129(6): 1300-1304.
Greggi S, Parazzini F, Paratore MP, et al. Risk factors for ovarian cancer in central Italy. Gynecologic Onco 2000; 79(1): 50-54.
Hartge P, Schiffman MH, Hoover R, et al. A case-control study of epithelial ovarian cancer. Am J Obstet Gynecol 1989; 161(1): 10-16.
Giovannucci E, Rimm EB, Stampfer MJ, Colditz GA, Willett WC. Height, body weight, and risk of prostate cancer. Cancer Epidemiol Biomarkers Prev 1997; 6(8): 557-563.
Nomura AM. Body size and prostate cancer. Epidemiol Rev 2001; 23(1): 126-131.
Lee IM, Sesso HD, Paffenbarger RS Jr. A prospective cohort study of physical activity and body size in relation to prostate cancer risk (United States). Cancer Causes and Control 2001; 12(2): 187-193.
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 2008; 371(9612): 569
Larsson SC, Wolk A. Overweight, obesity and risk of liver cancer: a meta-analysis of cohort studies. Br J Cancer. 2007; 97(7): 1005-1008.
Allison DB, Fontaine KR, Manson JE, et al. Annual deaths attributable to obesity in the United States. JAMA 1999; 282: 1583-1588.
Garfinkel L. Overweight and cancer. Ann Intern Med 1985; 103(6 Pt 2): 1034-1036.
Freedland SJ, Platz EA. Obesity and prostate cancer: Making sense out of apparently conflicting data. Epidemiol Rev 2007; 29: 88-97.
Reynolds JV, Donohoe CL, Doyle SL. Diet, obesity and cancer. Ir J Med Sci 2011; 180(2): 521-527.
The Cancer Prevention – Attitudes, Awareness and Behaviours Survey was conducted by Environics Research Group on behalf of the Canadian Partnership Against Cancer in 2008.
Inoue M, Yamamoto S, Kurahashi N, et al. Daily total physical activity level and total cancer risk in men and women: results from a large-scale population-based cohort study in Japan. Am J Epidemiol 2008; 168: 391-403.
Rockhill B, Willett WC, Hunter DJ, et al. A prospective study of recreational physical activity and breast cancer risk. Arch Intern Med 1999; 159: 2290-2296.
Hu FB, Willett WC, Li T, et al. Adiposity as compared with physical activity in predicting mortality among women. NEJM 2004; 351: 2694-2704.
Antonelli JA, Jones LW, Bañez LL, et al. Exercise and prostate cancer risk in a cohort of veterans undergoing prostate needle biopsy. J Urol 2009; 182: 2226-2231.
Patel AV, Rodriguez C, Jacobs EJ, et al. Recreational physical activity and risk of prostate cancer in a large cohort of US men. Cancer Epidemiol Biomarkers Prev 2005; 14: 275-279.
McKeown-Eyssen G. Epidemiology of colorectal cancer revisited: are serum triglycerides and/or plasma glucose associated with risk? Cancer Epidemiol Biomarkers Prev 1994; 3: 687-695.
Giovannucci E, Ascherio A, Rimm EB, et al. Physical activity, obesity, and risk for colon cancer and adenoma in men. Ann Intern Med 1995; 122: 327-334.
Martínez ME, Heddens D, Earnest DL, et al. Physical activity, body mass index, and prostaglandin E2 levels in rectal mucosa. J Nat Cancer Inst 1999; 91:950-953.
Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ Tech Rep Ser, 2000; 894: i-xii, 1–253.
 (click to enlarge)
(click to enlarge)
