Cancer-associated malnutrition, cachexia and sacropenia in the era of obesity
Nutritional deterioration has become an accepted part of the pathogenesis of cancer and its treatment
Dr Derek Power, Consultant in Medical Oncology, Cork University Hospital, Cork, Ms Aoife Ryan, Lecturer in Nutritional Sciences, Department of Food and Nutritional Sciences, University College Cork and Ms Louise Daly, PhD Student, Department of Food and Nutritional Sciences, University College Cork, Cork
Nutritional deterioration has unfortunately become an accepted part of the pathogenesis of cancer and its treatment. For the past 35 years several large-scale studies have reported that involuntary weight loss affects 50-80% of cancer patients1,2,3 with the degree of weight loss dependent on tumour site, size, type and stage. In patients with gastric or pancreatic cancer more than 80% of patients are affected, whereas approximately 50% of patients with lung, prostate or colon cancer lose weight.1,2,3
Within each tumour type, survival times are significantly shorter for patients who experience weight loss than in those who are weight stable2 and it is now well accepted that cancer cachexia is indirectly responsible for the death of at least 20% of cancer patients.4
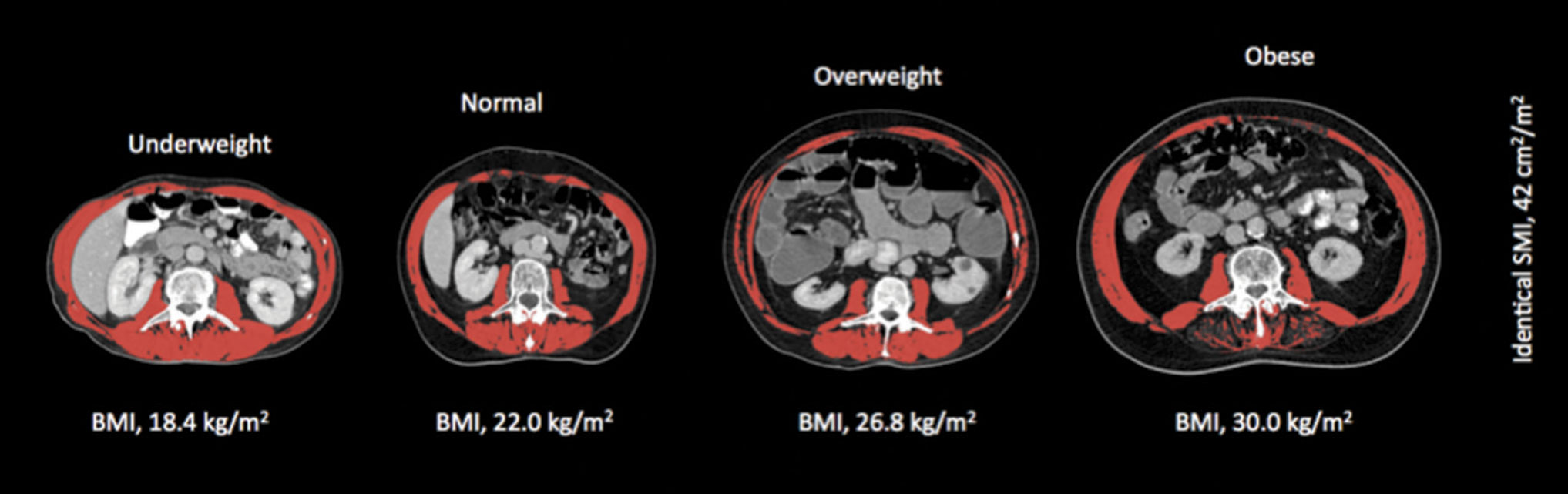
Figure 1A. Shows the variation in fat mass and body mass index (BMI) for four males with identical amounts of skeletal muscle(click to enlarge)
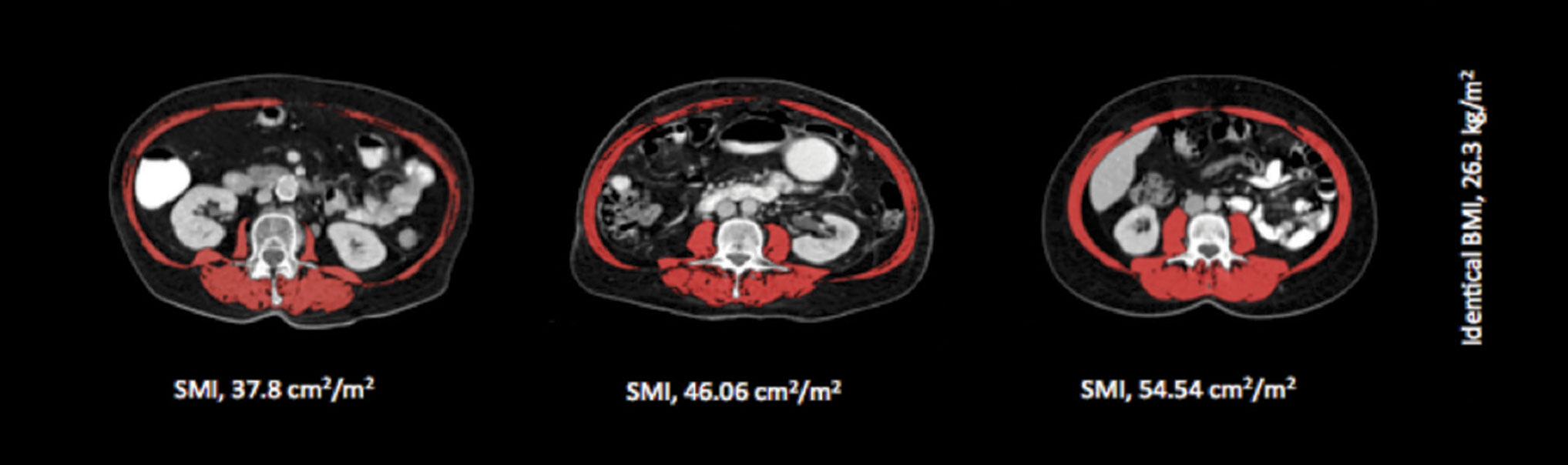
Figure 1b. Highlights skeletal muscle variation in three female patients with an identical BMI(click to enlarge)
Aetiology
The aetiology of cancer-induced weight loss is multifactorial and complex. Changes in nutritional status can occur at any point in the timeline of cancer diagnosis, treatment or support.5 These changes may occur as a result of metabolic changes, mechanical blockages or abnormalities, side effects of treatment, or psycho-social issues.
Insufficient oral intake
A wide variation in energy intake has been reported in cancer, ranging from 4 to 53kcals/kg/day.6 Several factors may directly lead to insufficient energy intake, eg. dysphagia, nausea, anorexia, xerostomia, early satiety, and changes in taste and smell.5 Other factors may have an indirect influence on energy intake by affecting appetite and the drive to eat, eg. pain, fatigue and psychological problems.6
Studies have suggested that a high prevalence of taste changes are associated with poor intakes as little as 900 to 1,100kcal/day,7 with other studies reporting energy deficits of up to 55,000 calories during chemo-radiotherapy in head and neck cancer.8
Host response to tumour
A variety of metabolic and endocrine changes, and activation of catabolic pathways also account for weight loss, which is typically greater than would be expected from the prevailing level of oral intake.5 Pro-inflammatory cytokines (secreted by either immune cells or tumours) play a central role and are key signals for lipolysis and proteolysis. Cytokines alter macronutrient metabolism, suppress appetite and also initiate an acute phase protein response (APR). This APR is energy-intensive with high requirements for essential amino acids, which drives the loss of muscle. In addition, inflammatory cytokines directly induce signalling pathways that up-regulate enzymes, inducing muscle protein turnover.
The pathway most involved in muscle wasting is protein degradation that is mediated by the activation of the ubiquitin-dependent proteasome pathway. Additionally, there are abnormalities in protein synthesis and degradation, amino acid metabolism, as well as increased apoptosis and an impaired capacity for regeneration.9
Physical inactivity
Many studies have shown that cancer patients are very inactive. In a study of hypermetabolic, cachectic pancreatic cancer patients, it was shown that the measured mean physical activity level (PAL) was much lower (mean 1.24) than that recorded in healthy adults of similar age (mean 1.62).10 This level of physical activity is comparable with that observed in spinal cord injury patients living at home11 or that observed in cerebral palsy (mean PAL 1.23).12 Levels of physical activity as low as this may exacerbate muscle wasting13,14 and it is well understood in any individual that lack of physical activity will cause deconditioning and deterioration in muscle mass,15 which in turn impacts the ability to exercise. This vicious cycle leads to progressive decline in physical activity and of muscle mass.
Cancer cachexia
The wasting in cancer is often termed cancer cachexia (CC), which has been defined as ‘a complex metabolic syndrome associated with underlying illness and characterised by loss of muscle with or without loss of fat mass’.16 In 2011, a consensus definition of CC was published by Fearon et al (2011) that proposed new criteria for diagnosing CC. Briefly, this definition requires any one of the following criteria to be met:
• Involuntary weight loss >5% over the past six months in the absence of simple starvation
• Weight loss >2% with a BMI <20kg/m2, or
• Weight loss >2% with an appendicular skeletal muscle index consistent with sarcopenia as measured by either computed tomography (CT) or dual-energy x-ray absorptiometry (DXA) (males <7.26kg/m2; females <5.45kg/m2).17
It is important to recognise that cachexia actually represents a spectrum of conditions. The first stage is precachexia where patients may first notice weight loss, sometimes even before the cancer diagnosis has been made. The second stage is the cachexia syndrome, which is characterised by weight loss in combination with evidence of systemic inflammation and reduced food intake. Those with advanced cachexia have depletion of fat reserves, severe muscle wasting, and are immunocompromised.
Whether a patient progresses down the pathway of worsening cachexia depends on the success of treating the primary disease and on addressing cachexia as well. Not all patients will progress down this spectrum to full cachexia. Some will die of their primary disease before they develop advanced cachexia, others will stabilise as a result of treatment of their primary disease.
Malnutrition, cancer cachexia and survival
If left untreated, cancer-related weight loss will progressively worsen. There is a vast array of published studies showing reduced survival in weight-losing cancer patients and in those with cachexia.18,19,20,21 A recent study by Martin et al (2015) on 8,160 cancer patients developed a robust grading system based on percentage weight loss and BMI which predicted survival. This study demonstrated that the loss of the ability to maintain weight (even a weight loss of 2.4%) significantly reduces survival, and those cancer patients with the lowest BMI and highest level of weight loss experienced survival rates consistent with Common Terminology Criteria for Adverse Events (CTCAE) grade 4, which is consistent with a life-limiting toxic side effect from chemotherapy.2
Overweight and obesity in cancer
While the majority of cancer patients present with involuntary weight loss at the time of diagnosis,2 in the era of obesity cancer patients may not ‘look’ malnourished, with recent studies reporting that 40-60% are overweight or obese, even in the setting of metastatic disease.2,22,23,24 As the most clinically relevant phenotypic feature of cancer cachexia is muscle loss, identifying those with muscle loss becomes a huge challenge in overweight and obese patients as the loss of muscle is masked by excessive adiposity.
Sarcopenia
Sarcopenia comes from the Greek ‘sarx’ for flesh and ‘penia’ for loss, and is defined as ‘the age-associated loss of skeletal muscle mass and function’, often described as a muscle mass two standard deviations below normal.25 The best way to diagnose sarcopenia is by direct measurement of lean mass by DXA or CT. Despite the presence of high BMI in cancer patients, sarcopenia is present in 20-70% depending on the tumour type. Cancer patients with sarcopenia have a poor prognosis regardless of overall body weight.24 Recently it has emerged that the co-existence of obesity and sarcopenia is the worst-case scenario.26
As discussed previously, an additional challenge for cancer care providers is the fact that sarcopenia is a phenomenon that may be obscured within the bulk of body weight and body weight change and this is now recognised as a clinically important phenomenon.
Sarcopenia and chemotherapy
Variability in body composition of cancer patients may be a source of disparities in the metabolism of cytotoxic agents. There is mounting evidence that sarcopenia increases the risk of toxicity to many drugs including epirubicin,27 capecitabine,28 sunitinib,29 sorafenib,30,31 5-FU and leucovorin,32 which are used in the treatment of a variety of cancers. Clinical trials investigating dose reductions in patients with sarcopenia and dose-escalating studies based on pre-treatment body composition assessment are currently underway and have the potential to alter cancer treatment paradigms.
Sarcopenia and survival
Several studies have recently identified sarcopenia as an independent predictor of poorer survival. Sarcopenia has also been identified as a predictor of overall survival after nephrectomy for metastatic renal cell carcinoma,30 following pancreatic surgery33 and following curative resection of colorectal cancer.34 Recently Martin et al (2013) in a large sample of 1,473 lung and gastrointestinal cancer patients reported significantly shorter overall survival in patients with weight loss, sarcopenia and low muscle density of 8.4 months (95% CI: 6.5-10.3) compared with an overall survival of 28.4 months (95% CI: 24.2-32.6, p < 0.001) in non-sarcopenic patients.24
In more recent years the importance of muscle density has come to the forefront with research highlighting its importance in treatment response, progression-free survival, and overall survival. Higher skeletal muscle density (SMD) has been associated with improved survival in renal cell carcinoma,27 melanoma35 and in a number of other solid tumours.24 SMD could potentially be a more accurate measure of muscle function and therefore precede the development of sarcopenia. Low SMD may be reflective of patients with a lower performance status.
Quality of life
Cancer-associated malnutrition and cachexia have also been shown to have profound negative effects on patient’s performance status, psychological wellbeing, and overall quality of life (QoL).5,17,21,36 A recent systematic review reported a negative correlation between QoL and weight loss in 23/27 studies of patients with CC.37 It is not surprising that weight loss has a negative impact on QoL, considering sarcopenia is a major cause of fatigue38,39 and weight loss is associated with reduced functional ability.40
Nutritional care of cancer patients
Unfortunately cachexia has perhaps suffered more from selective neglect and therapeutic nihilism than any other symptom requiring palliative care.41 While there are some new promising drugs undergoing phase III trials to treat CC, these are unavailable outside the research setting. There is currently no consensus on the optimal treatment for cancer cachexia, yet there is urgency for improving management. The fundamental difference between the weight loss observed in CC and that seen in simple starvation is the lack of reversibility with feeding alone. This seems to be caused by metabolic changes produced by the tumour. Therefore, attempts to modify these changes have the potential to improve both quality and length of life.
Several trials have examined single therapies for CC, including oral nutritional supplements (ONS), exercise or anti-inflammatory drugs, however the results of individual therapies have been disappointing. The role of physical activity has also been neglected in the past but has more recently been the subject of major ongoing studies. Studies targeting cachectic patients have demonstrated that, even in advanced disease, peripheral muscle has the capacity to respond to exercise training.42
Benefits of exercise include enhancing muscle protein synthesis, attenuating the catabolic effects of cachexia, and modulating levels of inflammation. However, there are challenges and limitations to cachectic patients engaging in exercise and many are not able or willing to undertake programmes.
Multimodal approaches
As multi-factors are responsible for the development of cachexia, it has recently been argued that multimodal therapy is required for this multidimensional problem.15,42,43 This approach would incorporate ONS, exercise and anti-inflammatory medications and nutritional supplementation (eg. high dose omega 3 fats, extra calories and protein). Underpinning this approach are meta-analyses suggesting that each of the intervention components, while not unequivocally associated with improved outcome, is more likely than not to be beneficial.44,45,46,47
The MENAC trial (a Multimodal Intervention [Exercise, Nutrition, Anti-inflammatory medication] plus standard versus standard care alone) to prevent/attenuate cachexia will test the efficacy of this multi-dimensional approach over the coming years. Patients with advanced lung and inoperable pancreatic cancer about to start chemotherapy will be randomised to standard care or standard care plus ONS enriched with eicosapentaenoic acid, exercise and non-steroidal anti-inflammatory drugs. The primary objective is to determine whether the intervention achieves a difference in skeletal muscle index at six weeks.
Conclusions
Levels of malnutrition in 2015 are similar to those reported more than 35 years ago, but today less than 7% of cancer patients are underweight (BMI < 18.5 kg/m2). The majority ‘look’ normal and 40-63% are overweight or obese. However, cachexia and sarcopenia are highly prevalent across all BMI categories with approximately one-third of obese cancer patients meeting the criteria for cachexia and 17-19% meeting criteria for sarcopenia. Cachexia and sarcopenia impact significantly on patients’ quality of life, tolerance to chemotherapy and survival.
Nutrition screening and early intervention should be mandated in oncology. However, not all cancer patients can avail of one-to-one dietetic care and all too often they are referred too late in the course of their disease/cachexia for a meaningful benefit to be achieved.
In an ideal world nutrition care should begin in parallel with medical care with weight stabilisation as an immediate priority, bearing in mind that this may not be achievable with nutrition alone. Anti-inflammatory agents along with physical activity are critical in the multimodal approach.
References
DeWys WD, Begg C, Lavin PT et al. Prognostic effect of weight loss prior to chemotherapy in cancer patients. Eastern Cooperative Oncology Group. Am J Med 1980; 69(4): 491-97
Martin L, Senesse P, Gioulbasanis I et al. Diagnostic criteria for the classification of cancer associated weight loss. J Clin Oncol 2015; 33(1): 90-99
Bozzetti F; SCRINIO Working Group. Screening the nutritional status in oncology: a preliminary report on 1,000 outpatients. Support Care Cancer 2009; 17(3): 279-84
Skipworth RJ, Stewart GD, Dejong CH et al. Pathophysiology of cancer cachexia: much more than host – tumour interaction? Clin Nutr 2007; 26(6): 667-76.
Blum D, Omlin A, Baracos VE et al. Cancer cachexia: a systematic literature review of items and domains associated with involuntary weight loss in cancer. Crit Rev Oncol Hematol 2011; 80(1): 114-44
Bye A, Jordhøy MS, Skjegstad G et al. Symptoms in advanced pancreatic cancer are of importance for energy intake. Support Cancer Care 2013; 21(1): 219-27
Hutton JL, Baracos VE, Wismer WV. Chemosensory dysfunction is a primary factor in the evolution of declining nutritional status and quality of life in patients with advanced cancer. J Pain Symptom Manag 2007; 33(2): 156-65
Kubrak C, Olson K, Jha N et al. Clinical determinants of weight loss in patients receiving radiation and chemo-irradiation for head and neck cancer: a prospective longitudinal view. Head Neck 2013; 35(5): 695-703
Argilés JM, Busquets S, Stemmler B, López-Soriano FJ. Cancer cachexia: understanding the molecular basis. Nat Rev Cancer 2014; 14(11): 754-62
Moses AW, Slater C, Preston T et al. Reduced total energy expenditure and physical activity in cachectic patients with pancreatic cancer can be modulated by an energy and protein dense oral supplement enriched with n-3 fatty acids. Br J Cancer 2004; 90(5): 996-1002
Mollinger LA, Spurr GB, el Ghatit AZ et al. Daily energy expenditure and basal metabolic rates of patients with spinal cord injury. Arch Phys Med Rehab 1985; 66(7): 420-6
Stallings VA, Zemel BS, Davies JC et al. Energy expenditure of children and adolescents with severe disabilities: a cerebral palsy model. Am J Clin Nutr 1996; 64(4): 627-34
Biolo G, Ciocchi B, Stulle M et al. Metabolic consequences of physical inactivity. J Ren Nutr 2005; 15(1): 49-53
Kortebein P, Symons TB, Ferrando A et al. Functional impact of 10 days of bed rest in healthy older adults. J Gerontol A Biol Sci Med Sci 2008; 63(10): 1076-81
Fearon FC. Cancer Cachexia: developing a multimodal therapy for a multidimensional problem. Eur J Cancer 2008; 44(8): 1124-32
Evans WJ, Morley JE, Argilés et al. Cachexia: a new definition. Clin Nutr 2008; 27(6): 793-99
Fearon KC, Strasser F, Anker SD et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011; 12(5): 489-95
Deans Da, Tan BH, Wigmore SJ et al. The influence of systemic inflammation, dietary intake and stage of disease on rate of weight loss in patients with gastro-oesophageal cancer. Br J Cancer 2009; 100(1): 63-69
Hess LM, Barakat R, Tian C et al. Weight change during chemotherapy as a potential prognostic factor for stage III epithelial ovarian carcinoma: a Gynecologic Oncology Group Study. Gynecol Oncol 2007; 107(2): 260-65
Buccheri G, Ferrigno D. Importance of weight loss definition in the prognostic evaluation of non-small-cell lung cancer. Lung Cancer 2001; 34(3): 433-40
Bachmann J, Heiligensetzer M, Krakowski-Roosen H et al. Cachexia worsens prognosis in patients with resectable cancer. J Gastrointest Surg 2008; 12(7): 1193-201
Ramos Chaves M, Boléo-Tomé C, Monteiro-Grillo I et al. The diversity of nutritional status in cancer: new insights. Oncologist 2010; 15(5): 523-30
Gioulbasanis I, Martin L, Baracos VE et al. Nutritional assessment in overweight and obese patients with metastatic cancer: does it make sense? Ann Oncol 2015; 26(1): 217-21
Martin L, Birdsell L, MacDonald N et al. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol 2013; 31(12): 1539-47
Baumgartner R, Koehler K.M, Gllagher D et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998; 147(8): 755-63
Prado CM, Lieffers JR, McCargar LJ et al. Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Lancet Oncol 2008; 9(7): 629-35
Antoun S, Lanoy E, Lacovelli R et al. Skeletal muscle density predicts prognosis in patients with metastatic renal cell carcinoma treated with targeted therapies. Cancer 2013; 119(18): 3377-84
Prado CM, Baracos VE, McCarger LJ et al. Sarcopenia as a determinant of chemotherapy toxicity and time to tumour progression in metastatic breast cancer patients receiving capecitabine treatment. Clin Cancer Res 2009; 15(8): 2920-26
Cushen SJ, Power DG, Teo M et al. Body composition by computed tomography as a predictor of toxicity in patients with renal cell carcinoma treated with sunitinib. Am J Clin Oncol 2014; [Epub ahead of print] DOI: 10.1097/COC.0000000000000061
Antoun S, Baracos VE, Birdsell L et al. Low body mass index and sarcopenia associated with dose-limiting toxicity of sorafenib in patients with renal cell carcinoma. Ann Oncol 2009; 21(8): 1594-98
Mir O, Coriat R, Blanchet B et al. Sarcopenia predicts early dose-limiting toxicities and pharmacokinetics of sorafenib in patients with hepatocellular carcinoma. PloS One 2012; 7(5): e37563
Prado CM, Baracos VE, McCargar LJ et al. Body composition as an independent determinant of 5-flurouracil-based chemotherapy toxicity. Clin Cancer Res 2007; 13(11): 3264-68
Sharma P, Zargar-Shoshtari K, Caracciolo et al. Sarcopenia as a predictor of overall survival after cytoreductive nephrectomy for metastatic renal cell carcinoma. Urol Oncol 2015; 33(8): 339.e17-23
Peng P, Hyder O, Firoozmand A et al. Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma. J Gastrointest Surg 2012; 16(8): 1478-86
Sabel MS, Lee J, Cai S et al. Sarcopenia as a prognostic factor among patients with stage III melanoma. Ann Surg Oncol 2011; 18(13): 3579-85
Ravasco P, Monteiro I, Vidal P et al. Cancer: disease and nutrition are key determinants of patients’ quality of life. Support Care Cancer 2004; 12(4): 246-52
Wheelwright S, Darlington AS, Hopkinson JB et al. A systematic review of health-related quality of life instruments in patients with cancer cachexia. Support Care Cancer 2013; 21(9): 2625-36
Evans WJ, Lambert CP. Physiological basis of fatigue. Am J Phys Med Rehabil 2007; 86 (1): S29-S46
Ryan JL, Carroll JK, Ryan EP et al. Mechanisms of cancer-related fatigue. Oncologist 2007; 12(1): 22-34
Fearon KC, Voss AC, Hudstead DS. Definition of cancer cachexia: effect of weight loss, reduced food intake, and systemic inflammation on functional status and prognosis. Am J Clin Nutr 2006; 83(6): 1345-50
Ross O, Ashley S, Norton A et al. Do patients with weight loss have a worse outcome when undergoing chemotherapy for lung cancers? Br J Cancer 2004; 90(10): 1905-11
Maddocks M, Murton AJ, Wilcock A. Therapeutic exercise in cancer cachexia. Crit Rev Oncog 2012; 17(3): 285-92
Solheim TS, Laird B. Evidence base for multimodal therapy in cachexia. Curr Opin Support Palliat Care 2012; 6(4): 424-31
Ryan AM, Reynolds JV, Healy LA et al. Enteral nutrition enriched with eicosapentaenoic acid preserves lean body mass following esophageal cancer surgery: Results of a double-blinded RCT. Ann Surg 2009; 249(3): 355–63
Ries A, Trottenberg P, Elsner F et al. A systematic review on the role of fish oil for the treatment of cachexia in advanced cancer: an EPCRC cachexia guidelines project. Palliat Med 2012; 26(4): 294-304
Balstad TR, Kaasa S, Solheim TS. Multimodal nutrition/anabolic therapy for wasting conditions. Curr Opin Clin Nutr Metab Care 2014; 17(3): 226-35
Caro MMM, Laviano A, Pichard C. Nutritional intervention and quality of life in adult oncology patients. Clin Nutr 2007; 26(3): 289-301
 Figure 1A. Shows the variation in fat mass and body mass index (BMI) for four males with identical amounts of skeletal muscle(click to enlarge)
Figure 1A. Shows the variation in fat mass and body mass index (BMI) for four males with identical amounts of skeletal muscle(click to enlarge)