To screen or not to screen, that is the question explored by Jane Sze Yin Sui, who investigates whether cancer screening programmes are helping or harming patients
Dr Jane Sze Yin Sui, Medical Oncology Specialist Registrar, Cork University Hospital, Cork
Cancer care is so much more than just treatment. Planning, prevention, early detection, diagnosis and treatment, palliative care and lastly policy and advocacy are the six-control plan released by World Health Organisation.1 Early detection represents an important aspect, with two strategies proposed: early diagnosis involving a patient’s awareness of early signs and symptoms, and national or regional screening of asymptomatic healthy individuals.1
Screening for cancer
Screening is defined as the presumptive identification of unrecognised disease in an apparently healthy, asymptomatic population by means of tests, examinations or other procedures that can be applied rapidly and easily to the target population.2 A screening programme must include all the core components in the screening process from inviting the target population to accessing effective treatment for individuals diagnosed with disease.2
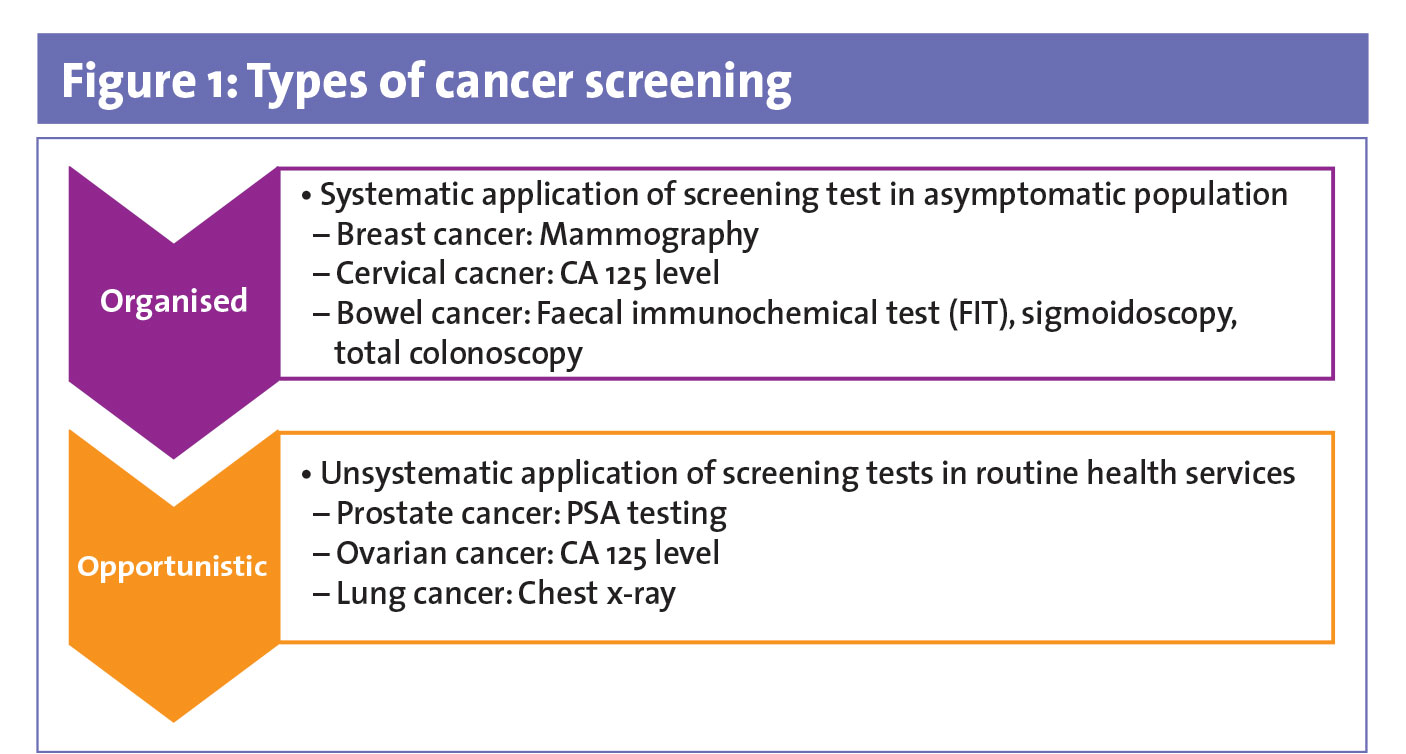
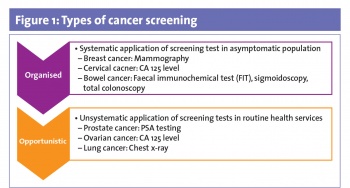
There are two types of screening: organised or opportunistic screening (see Figure 1).1 Organised screening is a systematic application of screening tests in asymptomatic population,1 such as mammography in breast cancer, Papanicolaou smear in cervical cancer and faecal immunochemical test (FIT) for bowel cancer. Meanwhile, opportunistic screening is the unsystematic application of screening tests in routine health services,1 eg. PSA testing in prostate cancer, CA 125 level in ovarian cancer and chest radiograph for lung cancer.
(click to enlarge)
For a screening programme to be effective, an acceptable test needs to be applied to over 70% of the population at risk.1 Early detection should lead to effective treatment leading to better outcomes.2 There should be strong evidence of improved mortality, morbidity or quality of life as a result.2
Recommendations regarding cancer screening vary from country to country, and may also vary within countries depending on the organisation making the recommendations.3 For example, in the US, the American Cancer Society, American College of Obstetrics and Gynecology, American College of Radiology and American Urological Association makes recommendations on screening depending on speciality, while the US Preventive Services Task Force (USPSTF) is an independent, volunteer panel of national experts making recommendations on prevention and evidence-based medicine. Both the UK and Canada have a national guideline committee to make these recommendations.3
In order for a screening programme to be successful, the implementation is important. In Ireland, the following three national cancer screening programmes were implemented under the National Screening Service:
BreastCheck commenced in February 2000 and offers screening mammogram every two years to women aged 50 to 64 years4
CervicalCheck commenced in September 2008 and offers free Pap smear tests to women aged 25 to 60 years4
BowelScreen, launched in 2012, offers FIT for men and women aged 60 to 69 years, and is expected to be extended to include people aged 55 to 74 years.5
These participants are invited to be screened. In the United States, the USPSTF recommends screening for breast cancer, cervical cancer, colorectal, lung cancer and breast cancer susceptibility genes (BRCA 1 and 2) in women with strong family history of breast, ovarian, tubal, or peritoneal cancer.6
Conceptually, cancer screening has myriad benefits. However, cancer screening is a double-edged sword. There is a recent shift in paradigm where expert groups are now proposing less screening, suggesting that screening may cause harm. Why the change now?
Cancer screening saves lives
In general, the benefit of cancer screening is apparent: early diagnosis of the disease or early detection of a pre-cancerous condition, in which intervention and treatment can reduce the likelihood of death from cancer.
In Ireland, there is a significant improvement in lifetime risk of cervical cancer from 1 in 96 prior to CervicalCheck to a lifetime risk of 1 in 135 post-implementation of screening.7 Studies suggested cervical cancer screening prevents cervical cancer deaths8 and reduces age-adjusted cervical cancer incidence.9 However, cervical cancer remains a significant public health issue in many developing countries due to limited resources and facilities. In India, screening using visual inspection with acetic acid every five years for women aged 30-65 years showed a reduction of cervical cancer mortality by approximately 30%.10
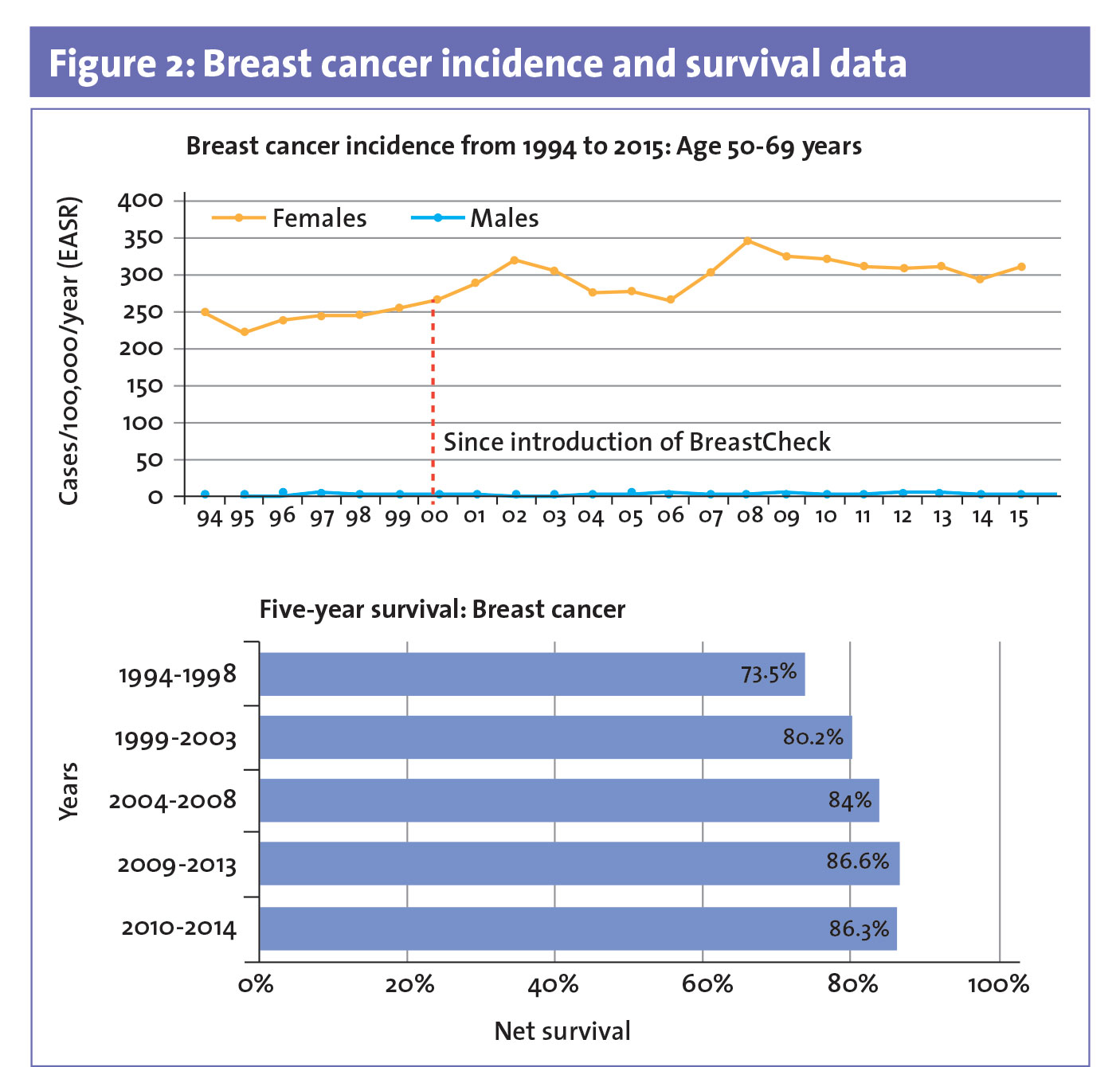
Since commencement of breast screening in Ireland, the incidence of breast cancer has increased, however survival rates have improved by approximately 20% (see Figure 2).7 In developing countries, such as the Philippines and Malaysia, pilot studies on breast cancer screening with physical examination, motivation and education of patients leads to improvement in survival by six months11 and reduction of breast cancer diagnosed in Stage III and IV by 25%.12
(click to enlarge)
The benefits of cancer screening have also been observed in colon and lung cancers: FIT screening detects colon cancer by 2.65 per 1000 cases with over 71% detected in stage I and II,5 therefore, long-term survival is excellent; and lung cancer screening using low-dose computed tomography (CT) detects 645 cases per 100,000 person-years, with a reduction in the mortality rate of 20%13 up to 61% depending on gender.14,15
Overall, despite differences in cancer screening among different countries, there is improvement in survival rates.
The potential risks of screening
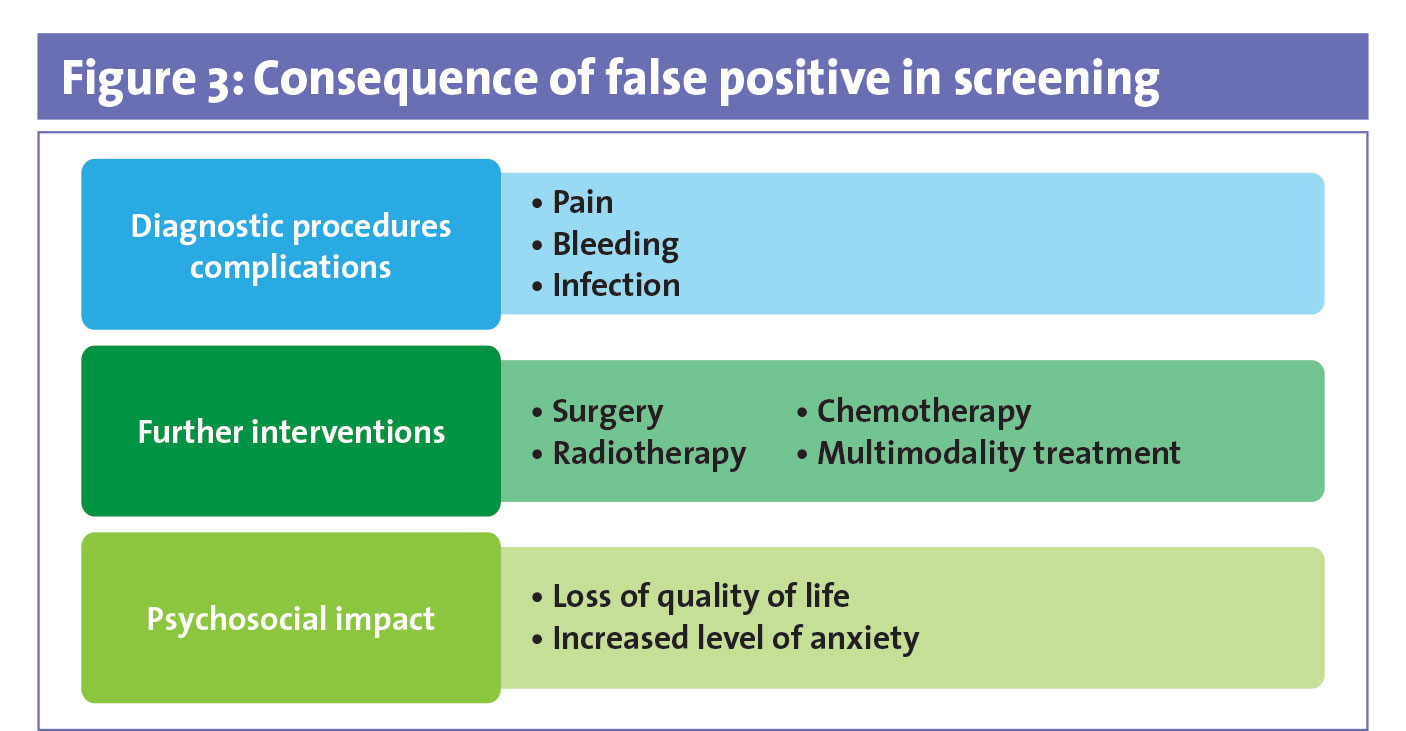
What is often understated or insufficiently addressed is the potential risks of cancer screening (see Figure 3). Positive screening tests often lead to diagnostic procedures which are associated with up to 1.4% of biopsy-related complications.13 Medical complications from the diagnostic process can cause bleeding, infection and pain.16,17
(click to enlarge)
Studies have shown that high false positive results leading to increased referral for further investigations18,19 resulted in needless surgical interventions, radiotherapy, chemotherapy, or some with multi-modality treatments.18 Multiple extra investigations from a false positive result lead to follow up testing incurring substantial loss of quality of life,20 negative psychological effects21 and possibly increased risk of preterm birth for many women.22
With cancer screening, there is a risk of a false negative. The consequences of false negative results may impact on delaying diagnosis and treatment, false reassurance and economic and legal implications.23
In 2018, cervical cancer screening became the centre of a major controversy in Ireland as 221 women had their smear test wrongly interpreted, leading to the death of 20 women secondary to screening errors.24
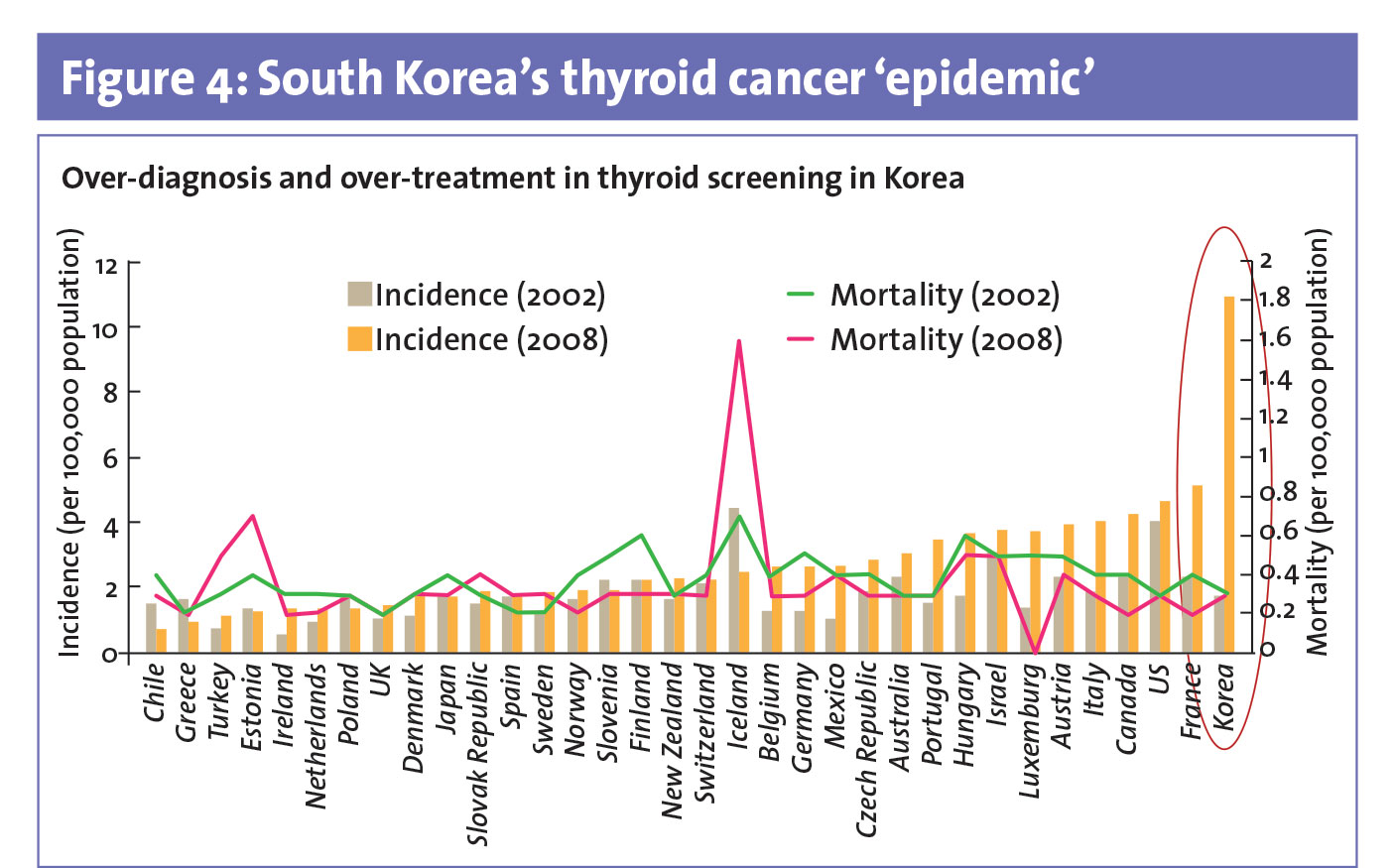
Last but not least, cancer screening can lead to over-diagnosis, which may lead to over-treatment. This is best exemplified with thyroid cancer screening in Korea25 where the over-diagnosis of thyroid cancer increased the incidence of thyroid cancer exponentially over the last 10 years (see Figure 4).26
(click to enlarge)
With thyroid screening, more than 90% of patients have thyroid removal without improvement of mortality rate leading to potential harm from cancer screening and failure of health-care policy.25,27
An often-debated risk of cancer screening is the excessive diagnosis of a malignancy that would most likely die with the patient, instead of killing the patient. In an autopsy study of women who died from other causes, 40% of these women had evidence of ductal carcinoma in-situ (DCIS).28 In Ireland, 21.2% of DCIS are diagnosed in women who are screened for the first time.29
Are we improving the survival data due to over-detection of DCIS, many of which would not have been diagnosed prior to screening? Or is this due to improvement in treatments available? In fact, this has led some countries such as. Switzerland to move away from breast cancer screening.
The Swiss Medical Board released a report on systematic screening with mammogram, acknowledging that screening prevented one death attributed to breast cancer for every 1000 women screened, with no reduction in overall mortality rate.30 Risk of over-diagnosis increased to 21.9%.31
Precision medicine beyond therapeutics
In Asia, countries such as Japan, Korea and Matsu Island of Taiwan have implemented the national screening programme for gastric cancer.32 However, in the United States, two studies showed that endoscopy screening is not cost-effective.33,34
Neither study stratifies according to race or ethnicity. A recent study showed that endoscopic screening in high-risk races and ethnicities could be cost-effective in the United States.35 Thus, is it reasonable to screen high-risk races and ethnicities in the US? We know gastric cancer risk decreases with successive generations.36 Therefore, is it really cost effective to screen when gastric cancer might decrease with successive generations?35
Similarly, in China, screening for hepatocellular carcinoma (HCC) in high-risk groups, Hepatitis B virus infection and chronic hepatitis, using six monthly alpha-fetoprotein and ultrasonography examination showed a reduction of HCC mortality by 37%.37 A meta-analysis showed HCC screening in patients with cirrhosis improves early tumour detection, recipient of curative treatment and improves overall survival.38
Women who have one or more family members with a known potentially harmful mutation in the BRCA1 or BRCA2 genes should be offered genetic counselling and testing.39 High-risk women and those who are BRCA mutation carriers who underwent risk reduction surgery substantially reduced their risk of breast or ovarian cancer.40 However, surgery leads to complications,41,43 postsurgical symptoms42 and impact on the spousal relationship.44
Future of screening
With rapid developments in cancer genomics and precision medicine, cancer screening approaches may evolve over time. The National Cancer Strategy recently outlined the priority of more personalised and tailored cancer screening.45 The current targeted screening based on family-history is missing an abundance of patients who are at risk. For example, studies using genomic profiling have found a higher incidence of germline mutations in genes mediating DNA-repair in men with metastatic prostate compared to previously known.46,47,48
In early 2018, there was hype surrounding the future of cancer screening using a new multianalyte blood test, called CancerSEEK, that can screen for eight common forms of cancer and help to identify the tumour location.49 Could this be the future in cancer screening? Unfortunately, not at the moment but this research may represent an important beginning of future screening.
To screen or not to screen?
Screening can deliver benefits and save lives but we must never forget that it may also cause harm. As we continue to expand our understanding of disease biology, molecular subtypes, and a higher rate of adoption of precision medicine in the treatment of cancers, exercising caution before implementing more screening programmes, and improving current programmes, is a reasonable option. Nevertheless, both healthcare professionals and members of the public should be adequately informed about the balance between the benefits and harms of cancer screening.
 (click to enlarge)
(click to enlarge)