Type 2 diabetes is an emerging global epidemic, largely due to increasing levels of obesity.1 More than 90% of the world’s 285 million people with diabetes have type 2 diabetes. In Ireland it is estimated that the condition will increase by 62% between 2007 and 2020.2
The prevalence of type 2 diabetes increases with age and ranges from 0.7% among those aged 18-44 years to 8.9% among adults aged 45 years and over.3 Approximately one-third of the latter group are undiagnosed.3 It is difficult to work out exact figures as each GP practice is different. However, most average practices should expect to have well over 100 patients with diabetes. As complications develop, the cost of treating diabetes increases alarmingly.
The CODEIRE study estimated in 2003 that the annual cost of treating a type 2 diabetes patient with no complications was Ä1,985 whereas the cost for a patient with macro- and microvascular complications was Ä49,345. Approximately 10% of the entire healthcare budget goes towards treating diabetes.5
The best way to manage patients with established type 2 diabetes, therefore, is to find cases early on in the course of the disease, before complications have developed, and to monitor these patients regularly, treating their vascular risk factors to prevent the development of complications.
Case finding in practice
Screening for diabetes in practice is not currently recommended.5 However, case finding is eminently possible and rewarding. The initial diagnostic testing may be elevated random blood glucose levels (over 11mmol/l), elevated fasting blood glucose (over 7mmol/l), usually with an elevated glycosylated haemoglobin (HbA1c) level of over 48mmol/mol. In the glucose tolerance test, a post load of over 11.1mmol/l is also diagnostic.
This means testing for people with diabetes among the following groups:
• Those with pre-diabetes
• Obesity
• Age over 50 years
• Those with positive family history
• GP attendees (two to three times the risk of the general population)
• Those with established vascular disease
• Those with a history of large babies
• History of gestational diabetes
• History of repeated infections
• Lower socio-economic groups
• Certain ethnic groups (eg. South Asian)
• Those taking certain drugs, eg. steroids.
In addition to this, diabetes patients may be found by searching the practice computer system for patients on diabetes drugs and those with elevated glucose levels. The local pharmacist may also be able to assist in the search.
Diet and lifestyle
The GP and practice team are central to the management of patients with type 2 diabetes in the community. After the patient is diagnosed by active case finding as described above, initial patient education should take place soon after. This involves simple dietary advice using the food pyramid, as well as simple lifestyle advice. The latter usually centres around moving more and eating less.6
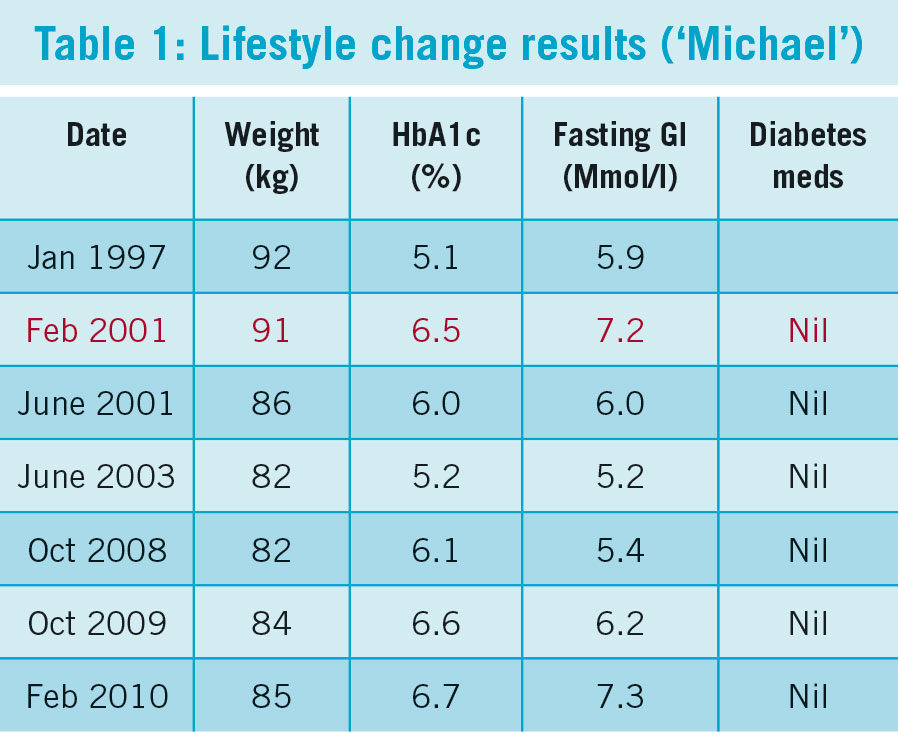
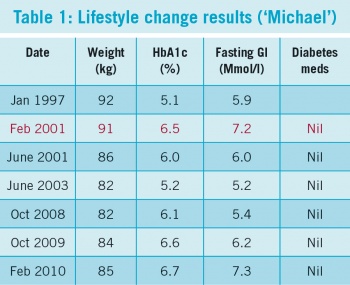
Table 1 illustrates how powerful the effect of lifestyle can be. Michael (not his real name) was aged 65 years when first diagnosed in 2001, early in the course of his disease through active case finding, as he was hypertensive.
(click to enlarge)
He adhered strongly to lifestyle advice and within two years had lost 9kg and was no longer biochemically diabetic. This was done using no oral hypoglycaemic agents (OHA). Over time he did regain some of the initial weight loss. This, coupled with the inevitable beta cell failure in the pancreas that occurs over time, led him to become diabetic again almost seven years later. Today, his HbA1c is still around 55mmol/mol on metformin 1,000mg BD.
Appropriate monitoring, prescribing and referral
Patients should be enrolled in the practice diabetes review programme (usually nurse-run). The aim of this is to have regular reviews to check on concordance with diet, lifestyle advice and medication in order to control risk factors. The idea is that long-term complications are prevented, detected early and managed appropriately. This involves prescribing for lipid control, hypertension, contraception and OHA where appropriate.
Managing cardiovascular risk should also include advice on smoking cessation, moderate alcohol intake and avoidance of illicit drugs.
Foot review, vaccination with influenza and pneumococcal vaccines, reviewing results, agreeing targets and planning until next review completes the picture.
All patients should be referred for:
• Diabetic retinopathy screening
• Dietary advice from the community dietitian if available
• Structured diabetes education programme eg. DESMOND or CODE for patients with type 2 diabetes.
Other possible areas of referral include:
• Chiropody, especially if patients are unable to manage to care for their own feet or have complex foot issues such as deformity
• Podiatry if appropriate and in accordance with local guidelines
• Community-based clinical nurse specialist (CNS) for those with difficult to manage glucose control
• Diabetes Ireland. All patients should be given the contact details of the local branch of this support group – www.diabetes.ie Services (such as the CODE education programme) and support are very helpful
• Referral to secondary care should only be done if problems remain that cannot be handled by the above measures. This might include, for example, initiation of insulin in certain areas.
The legacy effect
In UKPDS 80, good glucose control for about 10 years started at the onset of diabetes sets the patient on a trajectory that results in reduced complications 10 years later.7 This has come to be known as the ‘legacy effect’. It is therefore important that patients with newly diagnosed type 2 diabetes have their glucose levels tightly controlled for the first 10 years if there are no contraindications. Such contraindications would include risk of hypoglycaemia (eg. in an elderly patient living alone), the presence of co-existing illness (eg. severe COPD), patient capacity/life expectancy (eg. those with a terminal illness) and side-effect profile of drugs (eg. those who cannot tolerate OHAs).
It’s not all about sugar
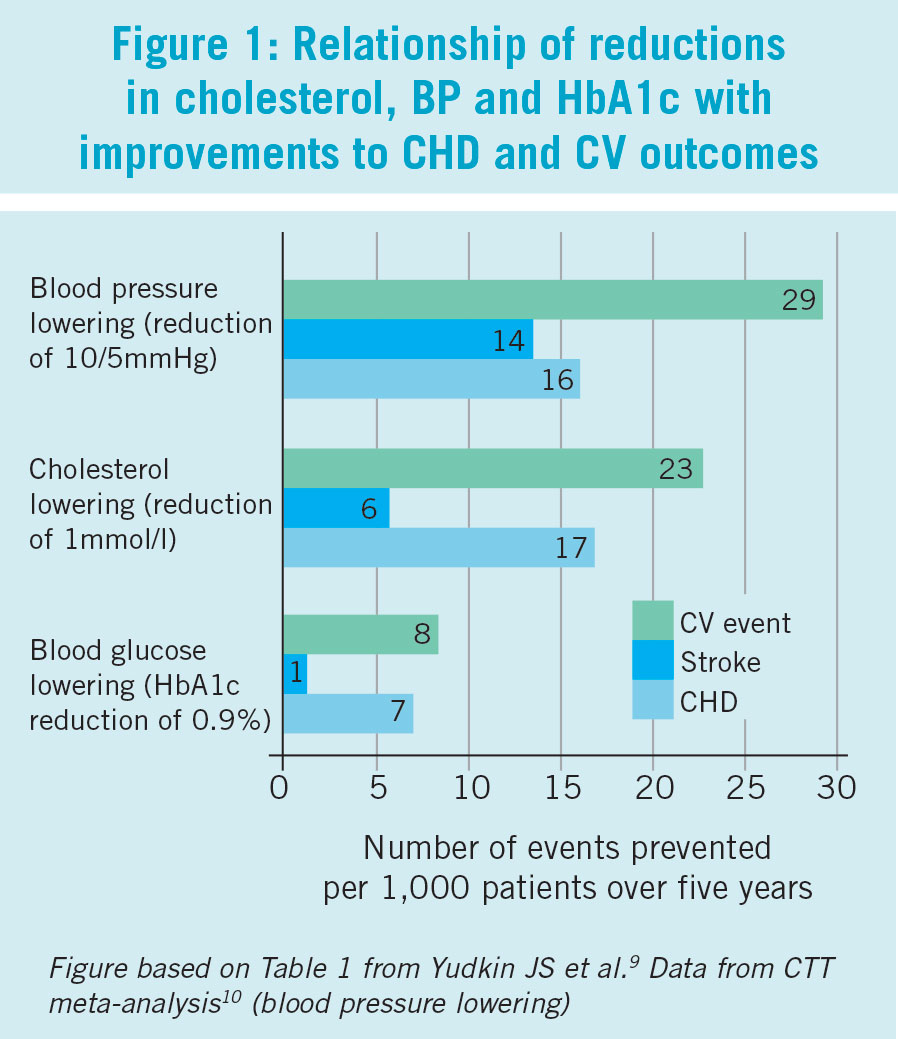
Figure 1 shows the different effects that altering three different risk factors has on vascular complications in patients with diabetes.8 It can be clearly seen that lowering blood pressure and cholesterol have far greater beneficial effect than lowering glucose levels. This figure also clearly illustrates the multifactorial nature of diabetes complications which are largely vascular in origin.
(click to enlarge)
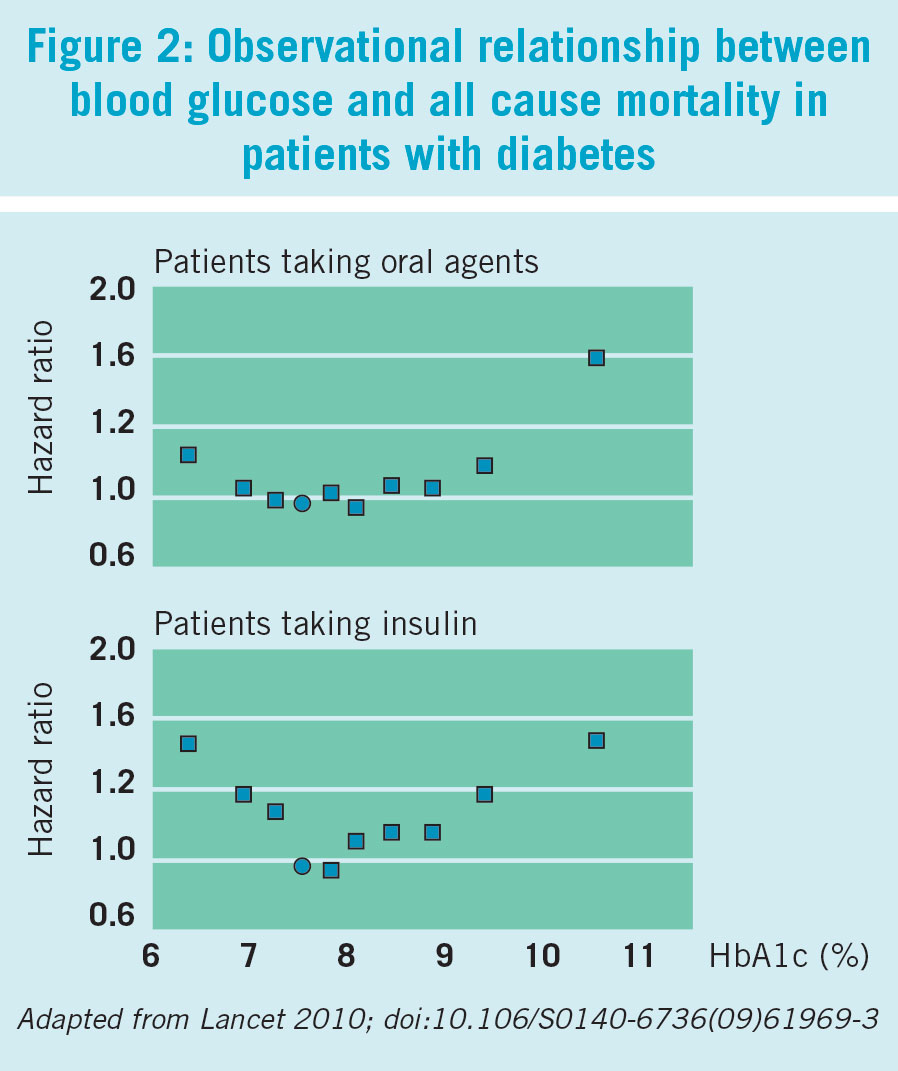
Figure 2 is taken from an observational study published in the Lancet9 based on the UK GP research database on a population of over 27,000 patients with diabetes. This showed the lowest risk of mortality with a glucose level of around 7.5% (59mmol/mol).
(click to enlarge)
Other targets
These need to be individualised to each patient.
Blood pressure (BP)
The effectiveness and safety of treating BP to intensive targets (< 130/80) compared with standard targets (140–160/85–100) showed only a small reduction in the risk for stroke and no reduction in the risk for overall mortality or myocardial infarction.10 Another Cochrane review has concluded that “at present, evidence from randomised trials does not support blood pressure targets lower than the standard targets”.11 More recently NICE in the UK12 has also stated that one should add medications if lifestyle advice does not reduce blood pressure to:
• Below 140/80 mmHg in the absence of complications
• Below 130/80mmHg if kidney, eye or cerebrovascular damage are present.
NICE also recommends antihypertensive medication:12
• Angiotensin-converting enzyme inhibitor or angiotensin receptor blocker (ACEI or ARB)
• Calcium channel blocker (CCB, first-line if pregnancy a possibility)
• Thiazide diuretic
• Others:
– Alpha blocker
– Beta blocker
– Potassium-sparing diuretic with caution.
Antiplatelets
Initial enthusiasm for widespread use of aspirin in people with diabetes has waned with the realisation that its benefits are not proven in the absence of overt cardiovascular disease, and it is not without its dangers.13,14,15,16
NICE12 recommends not to offer antiplatelet therapy (aspirin or clopidogrel) for adults with type 2 diabetes without cardiovascular disease. This is in keeping with the latest evidence.
Lipids
The complications of diabetes are largely vascular. There is substantial evidence that modifying lipid levels in diabetes is of benefit.17,18,19 There is also some evidence that statins can increase the risk of new onset diabetes, but the overall effect is still beneficial if appropriately prescribed.20
The 2015 NICE guideline reflects this balance and recommends use of the ‘qrisk-2’ cardiovascular risk assessment tool.21 It is recommended that we offer atorvastatin 20mg for the primary prevention of cardiovascular disease (CVD) with 10% or greater 10-year risk.12
NICE also recommend that for people 85 years or older consider atorvastatin 20mg if appropriate.12
Glucose control
This has already been discussed in the overview given above. For newly diagnosed patients who are otherwise healthy, tight control is important for the first 10 years at least, in order to maximise the ‘legacy effect’.7
However many patients diagnosed with type 2 diabetes for more than 10 years are elderly and infirm and have multiple comorbidities. For these patients a much more conservative approach is recommended. The ACCORD and VA trials22,23 showed that intense control in these patients made no difference to complications or indeed could cause harm.
A recent study on patient risks and preferences concluded: “For most patients over age 50 with an A1c below 9% on metformin, further glycaemic treatment usually offers at most modest benefits” and “Treating A1cs less than 9% should be individualised based on estimates of benefit versus patient’s views of the… burden”.24
Thus, for elderly and/or infirm patients, those with longstanding disease and who have comorbidities, it is important that treatment be individualised.
Glucose self monitoring
Self-monitoring of glucose should be limited to the following groups:12,25
• Those using insulin
• Those using oral hypoglycaemics that are likely to result in hypoglycaemia
• To assess changes in glucose control, eg. in response to treatment change
• During intercurrent illness
• Prior to activities, eg. driving
• Those who are pregnant.
Overall, the effect of glucose self-monitoring is not very convincing as was shown in a recent meta analysis.26 Another review concluded that “the overall effect of self-monitoring on glycaemic control in … people with type 2 diabetes who are not using insulin is small up to six months after initiation and subsides after 12 months.”27
There is an increased risk of dementia in elderly patients who suffer severe hypoglycaemia and this is another reason why such patients should not be controlled too tightly.28
HbA1c: how often
The recent NICE guideline12 recommends that this should be checked at three to six monthly intervals until the HbA1c is stable. Thereafter, it should only be checked at six monthly intervals once the HbA1c level and blood glucose lowering therapy are stable. Excessive testing has been shown to be wasteful and unnecessary.29
Oral hypoglycaemic agents
The drug of first choice is the biguanide metformin. It was first extracted from French lilac (Galega officinalis) and used in medieval times to relieve the frequent urination accompanying the disease that is today known as diabetes mellitus. It was first marketed in 1957.
A second biguanide marketed soon afterwards called phenformin was associated with lactic acidosis and withdrawn from the market. Metformin suffered by association. However metformin very rarely causes lactic acidosis. It should be used with caution in renal impairment and consultation with a renal or diabetes physician in such cases is advised.
It may cause nuisance side-effects such as nausea and diarrhoea, but it is usually weight neutral.
The UK Prospective Diabetes Study (UKPDS) showed clearly what a good drug metformin is.30 This was a multicentre randomised controlled trial that followed 4,209 patients over 10 years. Those on metformin had fewer diabetes-related major complications and diabetes-related deaths. Metformin reduced heart attack risk by 39%. Much of this risk reduction is unexplained and is independent of the effect of metformin on glucose control.
The 10-year follow-up study7 also showed that in the metformin group, significant risk reductions persisted for any diabetes-related endpoint (21%, P = 0.01), myocardial infarction (33%, P = 0.005) and death from any cause (27%, P = 0.002).
After metformin, and in the case that it is not tolerated or contraindicated, there is no uniform agreement on what OHA should be used next.
Many tables of recommendations exist. The American Diabetes Association and European Association for the Study of Diabetes Table of Recommendations is relatively easy to follow.31
Lifestyle is the first consideration, followed by metformin. After this, one or two drugs are added to metformin to give dual or triple therapy. An important consideration here is the presence of a functioning pancreas.
With passing time, the islet cells in the pancreas fail and the beta cells make less insulin. Thus after a while drugs that depend on the presence of functioning islet cells such as sulphonylureas do not work and need to be replaced by drugs that work independently of the pancreatic islet cells.
For a full side-effect profile for individual medicines, GPs should refer to the SmPC of each drug.
(This paper is based on a presentation given at the ICGP Diabetes Roadshow held in Limerick in January 2016.)
 (click to enlarge)
(click to enlarge)