GPs play a significant role in the diagnosis and management of food allergy in the community. There is also a role for all primary care health professionals to advise parents regarding allergy prevention for their children, a relatively new concept
Dr Aideen Byrne, Consultant in Paediatric Allergy, Tallaght Children’s Hospital and Our Lady’s Children’s Hospital, Dublin and Dr Fiona Magee, GP and Author, ICGP Quick Reference Guide to Food Allergy in Children in Primary Care, Dublin
Food allergy affects up to 6% of children in Ireland.1 Although some allergies typically resolve over time (cow’s milk, egg), others typically persist for life (peanut, tree nuts).2 Food allergy can be associated with significant morbidity and a negative impact on quality of life.3
In this module we will look at an overview of food allergy, explaining some key concepts. In terms of specific allergens, we will focus mostly on cow’s milk and egg allergy, two common types of food allergy where GPs play a key role in diagnosis and management. We will briefly introduce the concept of allergy prevention, which will be explained in more detail in the forthcoming ICGP Quality in Practice Guide to Food Allergy in Children in Primary Care.
Throughout the document, where ‘referral to a specialist’ is indicated, this can include an allergist or paediatrician with an interest in allergy.
Food allergy is an adverse reaction to food that is immune-mediated. It is important not to confuse food allergy with ‘food intolerance’, which is a less clearly defined term referring to any adverse reaction to food and does not describe an immune process. Lactose intolerance (rare in northern Europeans) is not an allergy, yet is commonly confused with cow’s milk protein allergy. The two conditions are unrelated other than both involving cow’s milk.
Types of food allergy
Food allergy can be divided into IgE-mediated (immediate) and non-IgE-mediated (delayed) types:
IgE-mediated allergy
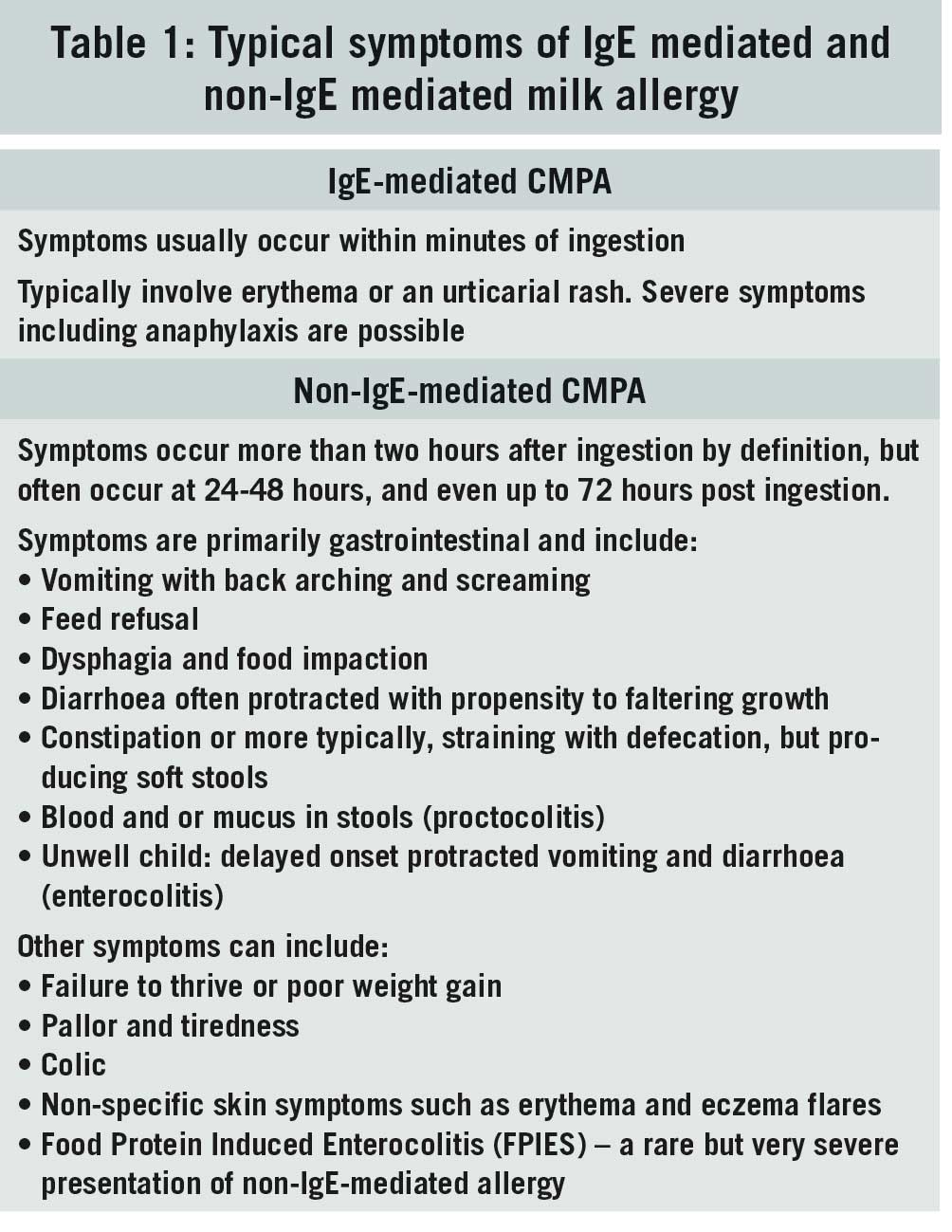
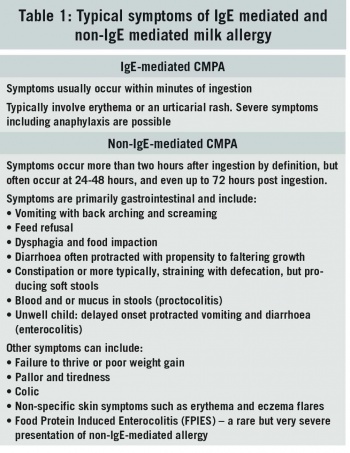
Symptoms occur typically within minutes of ingestion of the allergen and always < 2 hours post-ingestion.
Symptoms of IgE-mediated allergy can range from mild to severe. They include urticaria and sudden erythema of the skin, angioedema, acute rhinitis, abdominal pain and vomiting (along with the cutaneous symptoms) and in severe cases, signs of respiratory and/or circulatory compromise.
Respiratory compromise can include wheeze, shortness of breath, tongue-swelling, or even sudden onset hoarseness or cough indicating upper airway involvement. Circulatory compromise can include feeling weak or faint, lethargy, and collapse. Severe symptoms equate to anaphylaxis. Lip or facial angioedema alone are not considered severe symptoms. Examples of common allergens in IgE-mediated allergy are: egg, peanut and cow’s milk.
Non-IgE-mediated allergy
Symptoms are delayed > two hours and can occur as late as 24-48 or even 72 hours following ingestion of the allergen.
Symptoms of non-IgE-mediated allergy vary and are predominantly gastrointestinal. See Table 1 for typical symptoms of non-IgE-mediated cow’s milk protein allergy (CMPA). Food protein induced enterocolitis (FPIES) is a rare but serious complication of non-IgE-mediated allergy, involving shock-type symptoms and requiring urgent management.
(click to enlarge)
The most common allergen in non-IgE-mediated allergy is cow’s milk.
Most common food allergies in children in Ireland
The most common food allergies < 3 years of age are: egg, cow’s milk, peanut.
The most common food allergies > 3 years of age are: peanut, tree nuts.
This is because of resolution of egg and milk allergy. Most of the children who develop peanut allergy have had cow’s milk and/or egg allergy in their earlier years
Peanut is strictly not a nut, but rather a legume. Tree nuts include almonds, brazil nuts, hazelnuts, cashews, walnuts, pecans, macadamia, pistachio. All true nuts are ‘tree nuts’.
As diets in Ireland have expanded, allergens more commonly recognised abroad are now causing reactions here. Sesame, kiwi, fish, and pulses (peas, beans, chickpea, lentil) are all common food allergies in > 3 year olds in Ireland. Soya and wheat are rarely allergenic.
Risk factors for food allergy
The presence of eczema, especially if severe or early onset, is a significant marker of increased risk of food allergy4
The presence of one food allergy is a significant risk factor for developing another. IgE-mediated cow’s milk allergy indicates increased risk of subsequent egg5 and peanut allergy6, and egg allergy is a significant marker for subsequent peanut allergy7
Having a sibling with food allergy does not confer a significantly increased risk.
Food allergy prevention
In Ireland and much of the western world, allergenic foods such as nut products have tended to be avoided in the infant diet due to a fear that giving them to infants could cause allergies. The opposite is now known to be true.
Food allergy can be prevented by early introduction of allergens in the infant’s diet, as demonstrated in the landmark Learning Early About Peanut (LEAP) study, and subsequently Enquiring About Tolerance (EAT)9 study.8 LEAP demonstrated that introducing peanut to high-risk infants before 11 months and from as early as four months of age, the relative risk of peanut allergy at five years was reduced by 70-86%.8 The EAT study looked at an exclusively breastfed population without increased risk of food allergy and demonstrated a significant reduction in relative risk of egg and other food allergies, again by early introduction of the allergens in the infants’ diets. EAT also demonstrated no negative impact on breastfeeding with earlier introduction of solids.9
In terms of implications for our patients in general practice following these studies – what advice should we give?:
Parents of infants with the risk factors above (severe or early onset eczema, or the presence of one food allergy – similar to the inclusion criteria for the LEAP study) should be advised to introduce peanut and egg as early as possible in the weaning diet, in forms that are safe for small infants (eg smooth pure peanut butter, well-cooked mashed egg). They should be given these regularly in the diet, about three times a week and on an ongoing basis, at least for the first five years, to have the desirable effect of allergy prevention
Advice for the general population of infants without additional risk factors for food allergy should be to give these and other common allergens in the infant weaning diet without any need to delay their introduction. There is sense in giving one allergenic food at a time, so if a reaction occurs, the culprit is clearer. Allergenic foods should not be excluded in diets of pregnant women (unless the pregnant woman herself is allergic).
Allergy prevention as a public health priority is gathering traction worldwide. ‘Nip allergy in the bud’ is part of the Australian National Allergy Project. UK-based guidance documents for healthcare professionals and parents regarding allergen introduction to this effect are accessible online.10 It is imperative that this healthcare message reaches the parents of all at-risk infants in Ireland also.
Diagnosing food allergy
The greatest tool of allergy diagnosis is the clinical history. The first challenge is to gather adequate information to determine whether the adverse event (reaction) was allergic in nature. A history of urticaria or angioedema makes this more likely. A careful history should elicit a clear association between intake of the suspected allergenic food and the reaction in question. The reaction should recur if the allergen was encountered again. The absence of such a reproducible association makes allergy unlikely.
The allergy-focused history should obtain clear information about feeding history, being specific regarding breast or formula feeding and all solids already taken in the diet. Detail about the reaction that occurred, the setting where it happened, and all food ingested prior to it should be obtained. Other factors such as exercise and illness around the time of the reaction are relevant as these can worsen the severity of a reaction. Information regarding any history of other food allergies, eczema, rhinitis or asthma must be gleaned, including any family history of food allergies or atopy. Examination should involve an assessment of growth and centiles, assessing for pallor and any evidence of atopy.
On completion of the history, it is usually possible to either rule out food allergy as a likely cause and pursue another explanation, or to make a diagnosis of likely food allergy, without performing any tests.
Testing in food allergy
Food allergy testing is not required when assessing food allergy in most cases in primary care. It is primarily the remit of allergists or paediatricians/GPs with a special interest in allergy. The allergy-focused history is the key tool in either ruling out or making a diagnosis of food allergy, although in limited circumstances testing may play a role in primary care assessment.
The only valid ‘allergy tests’ for use in assessment of IgE-mediated food allergy are:
Skin prick testing (SPT) – to be carried out only by specially trained practitioners
Specific IgE serology (SpIgE).
There are a number of tests still being advertised in Ireland that purport to aid the diagnosis of food allergy. These include IgG testing, applied kinesiology, and hair-testing. There is no evidence base to support the use of these tests as stated by the HPRA.11,12
Specific IgE serology (SpIgE)13,14
GPs may utilise this test in certain circumstances (see ‘specific allergies’). It has replaced the now obsolete term ‘RAST test’.
It has very low sensitivity, therefore false positives are very common and tests should not be done without clinical suspicion of allergy to that food
It has high specificity – so a negative test can usually rule out allergy. However, in the case of a very convincing and clinically severe reaction, seek advice from a specialist before providing reassurance to a patient
It should never be used to test for Non IgE-mediated food allergy – there is no laboratory test for this type of allergy
It should never be used to test for a food currently being tolerated in the diet – by definition the child is not allergic to it
Broad panels of food allergens should not be tested, only the suspected allergen(s), usually one or two . Sometimes a likely co-allergen may be tested for
The term sensitisation refers to a positive test. The term allergy means that the child has had an allergic reaction
If an allergic reaction occurred, and the test is positive, the allergy is confirmed.
Cow’s milk allergy
Cow’s milk protein allergy (CMPA) occurs in approximately 1% of infants and children under two years in Ireland.1 It arises in infancy and does not develop de novo in childhood or adulthood.5 It typically resolves following infancy, and the majority of cow’s milk-allergic children tolerate cow’s milk in their diet by the age of five years.5 CMPA can be IgE-mediated or non-IgE-mediated.
Non-IgE-mediated CMPA
The presentation of non-IgE CMPA is predominantly with gastrointestinal symptoms. See Table 1 for a list of typical symptoms. As the symptoms are delayed and can occur as late as 24-72 hours post-ingestion, the relationship between ingestion and the reaction is not always immediately obvious.
Many of the symptoms are quite non-specific, with significant overlap with other very common presentations in early infancy such as colic and gastro-oesophogeal reflux. Non-IgE-mediated CMPA can usually be managed exclusively in primary care.
In infants who are formula fed from birth or soon after, non-IgE-mediated CMPA will usually present in the first few weeks of life (standard formulas in Ireland are cow’s milk based)
In infants who are breastfed initially and later changed to formula feeding, CMPA allergy may present at that time
It is also possible for non-IgE-mediated CMPA to present soon after birth in exclusively breastfed infants (whose mothers have dairy in their diet).
Diagnosis of non-IgE CMPA
The diagnosis is clinical – there is no test available for non-IgE-mediated allergy. If the diagnosis is suspected, a trial period of a completely dairy-free diet must be followed for approximately four weeks. This means using extensively hydrolysed formula (EHF) if formula fed.
If they are breastfed, the mother should be advised to do a trial of four weeks dairy-free diet. If the symptoms resolve, the diagnosis is deemed likely – but to confirm the diagnosis, a trial reintroduction of cow’s milk must be carried out. If the symptoms then recur, there is no need to prolong the reintroduction period – the diagnosis is now clinically confirmed, and milk should be excluded again.
Thus, the diagnosis is made clinically when symptoms improve on trial exclusion and recur following trial reintroduction of milk.
Management of non-IgE CMPA
The infant should return to EHF14 (or dairy-free diet for mother) once the diagnosis was confirmed on reintroduction of cow’s milk, now for a longer period of exclusion. Advice should be given regarding calcium and vitamin D supplementation. Ideally this would involve referral to a dietician for both infants and breastfeeding mothers, where this service is available.
In some more severe cases of CMPA where symptoms did not fully resolve with EHF, an amino acid (AA) formula may be used.14 In EHF the milk proteins (the allergenic part of cow’s milk) are broken into segments, whereas in AA formula, they are fully broken down into individual amino acids and are therefore the least allergenic form.
There is no role for partially hydrolysed formulas (often marketed as ‘comfort’ formulas), lactose-free formulas, goat, sheep or other mammalian formulas in the management of CMPA. Soy formula is not advised in non-IgE CMPA as it can cause similar GI symptoms.
Referral to a specialist is not usually required in non-IgE CMPA. In infants with CMPA who also have failure to thrive, referral to a paediatrician should be made.
Milk ladder
As CMPA typically resolves over time, the Cow’s Milk Ladder15 can be used to assist with the gradual reintroduction of cow’s milk in the diet (this is separate and later to the brief ‘trial reintroduction’ for the purpose of confirming the diagnosis).
For now, it is only recommended to use the Cow’s Milk Ladder in primary care in the case of non-IgE CMPA (not the IgE type, see below).
Typically, an attempt to start the Cow’s Milk Ladder will only be made several months after the initial presentation. The lower rungs of the ladder involve small quantities of baked milk, which is the least allergenic form, and it gradually increases to pure cow’s milk at the top.
In the context of non-IgE CMPA, the ladder is a way of assessing tolerance cautiously without inducing severe symptoms. If difficult symptoms recur with a step up the ladder, it is not advisable to persist or ‘push through’ at this time. Parents should be advised to return down to the ‘rung’ on the ladder that the child was tolerating.
IgE-mediated CMPA
It can be seen from Table 1 that the presentation of IgE CMPA is very different to the non-IgE delayed type. Symptoms occur immediately, or very soon after ingestion, and typically involve urticaria or erythema, often around the neck and face. Severe symptoms are possible. IgE CMPA requires specialist input.
IgE-mediated CMPA is less common in infants established on formula milk from birth
IgE-mediated CMPA rarely presents while infants remain exclusively breastfed, never having been given formula or dairy-containing solids
However, as breastfed infants wean to formula or dairy-containing foods, CMPA tends to reveal itself. It is likely that these infants were sensitised early in infancy
Tolerance typically develops later in infancy/childhood than with the non-IgE type but the majority will eventually tolerate cow’s milk.5
Diagnosis of IgE-mediated CMPA
A diagnosis of IgE CMPA can be made following a good clinical history where the story fits the picture of an immediate type reaction following milk ingestion. Testing should generally be deferred in general practice until the infant is seen in a specialist setting.
Management of IgE-mediated CMPA
Cow’s milk should be excluded from the diet. In a formula fed infant, the formula should be changed to EHF (or AA formula if symptoms do not resolve with EHF).14 In an infant taking solids, or when the time arrives for solid food, cow’s milk should be excluded. It is important to make parents aware of the presence of cow’s milk in many infant foods such as baby cereals, and they should be advised to read food labels accordingly. Again, vitamin D and calcium supplementation should be managed.
Soy formula can be used in infants over six months (although note that it is not advised in non-IgE CMPA). Again, other mammalian formulas or milk (such as goat and sheep milk) should not be used due to significant crossover of animal proteins. There is no role for excluding dairy in the diet of breastfeeding mothers in the case of IgE CMPA - only the infant’s diet should be manipulated.
The infant with suspected or likely IgE CMPA should be referred to a specialist. It is important to specify the severity of symptoms on the referral to allow for appropriate triage. Adrenaline autoinjectors are not generally required in CMPA and should not be prescribed in primary care for this purpose – if there was concern that the symptoms were severe/in the anaphylaxis category, the case should be discussed directly with a specialist. At present, reintroduction of milk using the Cow’s Milk Ladder15 to aid with developing tolerance in IgE CMPA is carried out only in the specialist setting.
Egg allergy
Egg allergy is the most common food allergy in Ireland, occurring in 3% of Irish infants.1 It is usually an immediate type (IgE-mediated) allergy. The presentation typically coincides with the introduction of egg in the diet, often in late infancy. As with for CMPA, the majority of children will outgrow their allergy to egg. Well-cooked egg is less allergenic than raw or lightly cooked egg, especially if baked with wheat. The majority of egg-allergic infants (70-90%) can tolerate egg baked with wheat.16
Diagnosis of egg allergy
Diagnosis is clinical, based on the allergy-focused history. As it is common practice to give infants scrambled (very lightly cooked) egg as their first exposure to egg, reactions commonly involve quite extensive cutaneous involvement (eg. urticaria and angioedema) with or without vomiting. Angioedema of the face and lips is common. In contrast, severe symptoms (respiratory and/or circulatory compromise), which equate to anaphylaxis, are less common. Beware a history of an infant becoming floppy, even if it self-resolves. This is indicative of a more severe reaction.
Testing for egg allergy is rarely required in primary care. However, if there is uncertainty regarding the diagnosis or the offending allergen despite a thorough history, specific IgE serology to egg can be considered.
Management of egg allergy
Once a diagnosis of egg allergy is clinically established, complete exclusion of egg is almost never required. In the case of a mild- moderate immediate-type reaction to egg (most reactions fall in this category), the infant should continue to be given any form of egg previously tolerated. For example, they may have reacted to their first exposure to scrambled egg, but have already been tolerating scones (containing small amounts of baked egg) without any adverse effects.
Mild-moderate cases can be started on the IFAN Egg Ladder18 in the community, ie. by the parents at home. The lowest rungs of the ladder are the least allergenic with small amounts of egg baked with wheat, progressing gradually to lightly cooked egg and then almost raw egg at the top. The purpose of this approach is to improve the quality of life of infant and carers, reduce anxiety amongst carers and promote the development of tolerance to egg.
However, if severe symptoms (anaphylaxis) occurs, all egg should be avoided and an urgent specialist referral made.
Adrenaline autoinjectors (AAI) are not often required in egg allergy. If a history of anaphylaxis to egg seems clear from the story, AAI can be initiated in primary care,17 but if in any doubt, discuss the case with a specialist before prescribing.
All infants with egg allergy, even those in the mild-moderate category being started on the IFAN Egg Ladder18 in the community, should currently be referred to or at least discussed with a specialist at the time of diagnosis. This is because egg allergy is a strong marker for other food allergies (eg. peanut)7 and allergy specialists wish to assess all of this egg-allergic cohort in their clinics.
Remember that infants with egg allergy fall in the category for early introduction of peanut.
Vaccines and egg allergy16,19
The MMR vaccine does not contain egg and can be given in the usual manner in the community to egg allergic children. The flu vaccine has a variable egg (ovalbumin) content from year to year. Those with an ovalbumin content < 0.1µg per dose can be given in primary care to egg allergic children without higher risk (ie. a history of anaphylaxis or severe uncontrolled asthma). Children who do fall in this higher risk group are probably still candidates to be given the flu vaccine in the community but it is advisable to discuss with their specialist first.
The yellow fever vaccine contains egg and should not be given to an egg-allergic child in the community. Discussion should be held with a specialist.
For all the above vaccines, consult the HSE immunisation guidelines19 for the most up-to-date advice.
Peanut allergy
We will only deal with this briefly as all cases will be under the care of a specialists. However, many cases present for the first time in primary care and GPs play a key role in the ongoing support of atopic children.
Peanut allergy refers to a clinical reaction to peanut and not just a positive allergy test (see ‘testing’) which is termed peanut sensitisation. Sensitisation may or may not present a health risk
The incidence of peanut allergy is approximately 2% of children in Ireland1
Unlike milk and egg allergy, tolerance does not usually develop – the allergy persists in 80% of children20
Severe reaction (anaphylaxis) is more common than with the other allergies described here; 30-40% of reactions are severe
Most children will have other atopic conditions (80-90%)20
Recent data has shown that 60% of peanut allergic children go on to develop tree nut allergies without preventative intervention strategies.21 Such strategies are the remit of specialist care
Referral to a specialist should be made without delay for suspected peanut allergy specifying as urgent if the reaction was severe
Consider doing specific IgE to peanut if available on the basis of clinical suspicion. Do not allow testing to delay the referral – although consider forwarding the results when available
All peanuts (and tree nuts not yet tried or tolerated) should be avoided until seen by the specialist22
Adrenaline autoinjectors (AAAs) are ultimately required in most children with peanut allergy, but immediate initiation of these in primary care is not always necessary- discuss with an allergy specialist if in doubt.
Adrenaline autoinjectors (AAIs)
On occasion, it may be appropriate to initiate AAIs in primary care.17 This should only be following a clear history of severe immediate type allergic reaction ie anaphylaxis. If there is any doubt regarding the indication the case should be discussed with a specialist before prescribing. Specialists may prescribe AAIs without a history of anaphylaxis to children considered to be at high risk of it.
If prescribing an AAI in primary care, the dosing is as follows (all brands):
150µg for children 15-30kg
300µg for children > 30kg
500µg for those > 50kg.
Infants weighing < 15kg should not be prescribed AAIs in primary care.
AAIs contain adrenaline 1/1,000 and are always given as an intramuscular injection into the anterolateral thigh. A child requiring AAI should have two devices with them at all times.
References
Kelleher MM, Dunn-Galvin A, Gray C, Murray, Deirdre M., Kiely M, , Kenny L, et al. Skin barrier impairment at birth predicts food allergy at 2 years of age. Journal of Allergy and Clinical Immunology, The. 2016;137(4):1111,1116.e8
Savage, Jessica, MHS, Sicherer S, Wood R,. The natural history of food allergy. Journal of Allergy and Clinical Immunology: In Practice. 2016;4(2):196-203
Cummings AJ, Knibb RC, King RM, Lucas JS. The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their families: a review. Allergy 2010 Aug; 65(8):933-945
Oosthuizen L, Mc Aleer MA, Watson RM, O’Regan GM, Byrne A, Crispino-O’Connell G, et al. Nottingham Eczema Severity Scoring tool can identify children at high risk of food allergy to cow’s milk, egg and peanut. Clinical and Translational Allergy. 2015;5(S3)
Saarinen KM, Pelkonen AS, Mäkelä MJ, Savilahti E. Clinical course and prognosis of cow’s milk allergy are dependent on milk-specific IgE status. The Journal of Allergy and Clinical Immunology. 2005;116(4):869-75
Sicherer SH, Wood RA, Perry TT, Jones SM, Leung DYM, Henning AK, et al. Clinical factors associated with peanut allergy in a high-risk infant cohort. Allergy. 2019;74(11):2199-211
Du Toit, George, Roberts G, Sayre, Peter H., Plaut M, Bahnson HT, Mitchell H, et al. Identifying infants at high risk of peanut allergy: The Learning Early About Peanut Allergy (LEAP) screening study. Journal of Allergy and Clinical Immunology, The. 2012;2013;131(1):135,143.e12
Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015 Feb 26; 372(9):803-813
Perkin MR, Logan K, Marrs T, Radulovic S, Craven J, Flohr C, et al. Enquiring About Tolerance (EAT) study: Feasibility of an early allergenic food introduction regimen. J Allergy Clin Immunol 2016 May; 137(5):1477-1486.e8
BSACI, BDA Food Allergy Specialist Group, Preventing allergy in higher risk infants: guidance for healthcare professionals, available from bsaci.org
https://www.nice.org.uk/guidance/cg116
HPRA Medical Devices Information Notice: Food Intolerance Testing, 2018
HSE. Laboratory testing for total IgE and Specific IgE. National Laboratory Handbook Dublin: HSE; 2017
Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C, et al. EAACI food allergy and anaphylaxis guidelines: diagnosis and management of food allergy. Allergy 2014 Aug; 69(8):1008-1025
Clark AT, Skypala I, Leech SC, Ewan PW, Dugue P, Brathwaite N, et al. British Society for Allergy and Clinical Immunology guidelines for the management of egg allergy. Clin Exp Allergy 2010 Aug; 40(8):1116-1129
Ewan P, Brathwaite N, Leech S, Luyt D, Powell D, Till S, et al. BSACI guideline: prescribing an adrenaline auto-injector. Clinical & Experimental Allergy. 2016;46(10):1258-80
Skolnick HS, Conover-Walker MK, Koerner CB, Sampson HA, Burks W, Wood RA. The natural history of peanut allergy. The Journal of Allergy and Clinical Immunology. 2001;107(2):367-74
Brough HA, Caubet J, Mazon A, Haddad D, Bergmann MM, Wassenberg J, et al. Defining challenge-proven coexistent nut and sesame seed allergy: A prospective multicenter European study. The Journal of Allergy and Clinical Immunology. 2020;145(4):1231-9
Vander Leek TK, Liu AH, Stefanski K, Blacker B, Bock SA. The natural history of peanut allergy in young children and its association with serum peanut-specific IgE. The Journal of Pediatrics. 2000;137(6):749-55
 (click to enlarge)
(click to enlarge)