With food allergies on the increase, and an important cause of concern for children and families, GPs need to acquire the skills to assess and diagnose children with potential allergies
Dr John Fitzsimons, Consultant Paediatrician, Our Lady of Lourdes Hospital, Drogheda
Food is an essential part of life. It defines cultures, marks occasions and punctuates our days. For children and parents, sharing food and eating together enhances feelings of fulfilment, security and happiness. Understandably then, when a child has an adverse reaction to food, all of these elements are threatened and fear may replace the safety and joy of simple normality.
Food hypersensitivity is the umbrella term used to describe adverse reactions to food and includes food allergy, which involves the immune system, and food intolerances, which do not. This is a common problem with up to a third of parents describing their children as having food hypersensitivity at some stage during childhood.
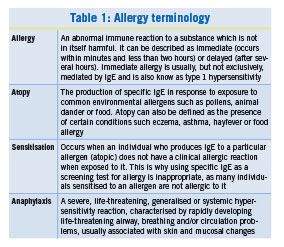
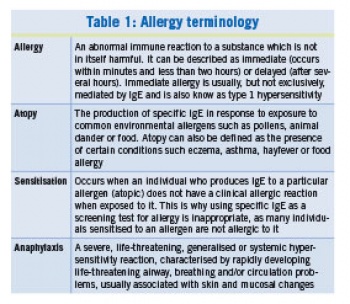
In 2013, the Irish Food Allergy Network (IFAN) launched its website www.ifan.ie, aimed at supporting frontline practitioners in primary and secondary care to recognise and diagnose food allergy in children. The website also provides information and supporting materials for the management of food allergy. This article provides an overview of childhood food allergy and makes reference to several of the resources that can be found on the IFAN website. In order to understand food allergy in childhood, it is important to be aware of the specific definitions of the terms listed in Table 1.1
(click to enlarge)
Food allergy is the biggest single cause of food hypersensitivity in childhood. It is common, with a reported prevalence in young children of between 5-10%. Food allergy can be classified into IgE-mediated (immediate) reactions or non-IgE-mediated (delayed) reactions. It is important to recognise food allergy among other hypersensitivity reactions so that appropriate treatment and dietary advice can be given.
Of particular importance is exploring the risk of anaphylaxis so that foods that must be avoided are known and plans are in place to manage accidental reactions. Equally, it is important to avoid unnecessary or unsupervised diets which may impact on a child’s growth and quality of life.
Food allergy in childhood
Cow’s milk, hen’s egg, wheat, soya, peanut, tree nut, sesame, fish and kiwi fruit are responsible for the majority of food-induced allergic reactions in children, although any food may be implicated. Most children with food allergy are allergic to more than one food. In general, children with milk, egg or wheat allergies are likely to outgrow them during childhood, while those with nut, fish or shellfish allergies are likely to remain allergic into adulthood.
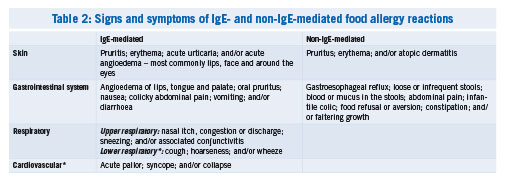
The first indication that an individual has a food allergy is usually when they display signs consistent with an allergic reaction after contact with a particular food or substance (the allergen). The use of an allergy-focused history and examination will help distinguish the type of food hypersensitivity (ie. allergy or intolerance) and if it is thought to be an allergy, whether it is IgE- or non-IgE-mediated. Many signs and symptoms of food allergy reactions, both IgE- and non-IgE-mediated, are included in Table 2.
(click to enlarge)
An allergy-focused examination should look for evidence of other allergic conditions such as urticaria, eczema or allergic rhinitis. It is very important to assess the child’s nutritional status noting weight, length and subcutaneous fat stores. Eczema is a major risk factor for the development of IgE-mediated food allergy; 20% of children with moderate to severe eczema will develop peanut allergy and 90% of children with peanut allergy have or had a history of eczema. It is important to stress however that beyond infancy at least, food rarely causes eczema to flare (as distinct from acute urticarial reactions), with most eczema exacerbations reflecting the cyclical nature of the disease.
IgE-mediated allergy is also referred to as type 1 hypersensitivity or immediate allergy with most immediate reactions occurring within minutes and usually no later than a couple of hours after exposure. Other features of the reaction will support or refute a diagnosis of IgE-mediated allergy such as those listed in Table 3. A template for taking an allergy-focused history (under the ‘food allergy in summary’ tab) and algorithms for the diagnosis of allergy (under the ‘primary and community care’ tab) are available on www.ifan.ie
(click to enlarge)
Finally, food intolerance is a non-immunological reaction that can be caused by enzyme deficiencies, pharmacological agents and naturally occurring substances. They are usually idiosyncratic reactions and are often not reproducible. In-depth consideration of food intolerances is beyond the scope of this article other than to say that dietitian input is always valuable.Non-IgE-mediated – also referred to as delayed or cell-mediated hypersensitivity – occurs hours or days after exposure. Most non-IgE-mediated food allergy is non-specific and is usually considered among a large list of alternative diagnoses, especially in young children. There are however, constellations of symptoms and an index of suspicion must be maintained. Whereas common conditions such as infant colic or gastro-oesophageal reflux may be caused by food allergy, in general they are not.
Allergy testing
Confirming a diagnosis of food allergy is important as it justifies the avoidance of the suspect food allergen(s) and the implementation of the appropriate management plan. Conversely, a negative allergy diagnosis allows for safe dietary expansion or prompts other diagnostic investigations being performed. The NICE guideline on Food Allergy in Children and Young People2 recommends that a health professional has the ‘relevant competencies’ needed to undertake and interpret allergy testing before requesting them. What these competencies are is not specified but includes utilising the concepts outlined below.
IgE to specific allergens may be measured by blood testing (for specific IgE, previously called RAST testing) or by skinprick testing (SPT). When considering IgE testing it is important to be aware of allergic sensitisation. Only when an individual who demonstrates raised IgE to foods or environmental allergens (eg. pollen) reacts clinically on contact with an allergic reaction (eg. urticaria, swelling, wheezing) are they considered to be allergic. Many individuals have a raised specific IgE but do not react on contact with the allergen; these individuals have allergic sensitisation, but not allergy. This is important in order to understand allergy testing, as to indiscriminately measure specific IgE or SPTs will yield as many people who are sensitised as are allergic, reiterating the importance of the allergy-focused history and examination when choosing tests.
Blood-specific IgE is available in most primary care settings and should be used (judiciously) to confirm suspected food allergy. It is important to note that the specific in ‘specific IgE’ means just that: it is important to specify, milk or egg or cod, not just ‘food’ or specify hazelnut or peanut rather than ‘nut’.
In recent years, recombinant allergen testing has become available. These tests measure specific IgE to components of allergens in the hope of increasing specificity. This has been very useful in peanut allergy with the Ara h2 component, but the usefulness of other components remains controversial for now.
The ultimate test for food allergy is the oral food challenge (OFC). Food challenges help to distinguish between sensitisation and allergy and to confirm that an individual has outgrown a food allergy. Food challenges must be carried out by trained individuals in an environment prepared to manage a severe allergic reaction or anaphylaxis. In the case of non-IgE-mediated food allergy there is currently no validated, reliable test with the exception of dietary exclusion and re-evaluation. Because these reactions are generally mild (although troublesome) it is usually safe to reintroduce foods at home provided there is no evidence of IgE-mediated allergy nor a history of a previously severe reaction.
It is important that practitioners have awareness of some of the ‘alternative’ allergy tests available to patients in the community, many of which are expensive. The NICE guideline on food allergy recommended against using Vega testing, kinesiology and hair testing on the basis that there are no studies to support their use. It also advises against using IgG testing to foods, as there is no validated evidence to support it. These are also the recommendations of the European and American allergy associations.
Common childhood food allergies
Cow’s milk protein allergy
Cow’s milk protein allergy (CMPA) is the most common childhood allergy. It is well recognised that there is IgE- and non-IgE-mediated CMPAs, and occasionally they may be mixed.
IgE-mediated CMPA
Babies may present dramatically after their first exposure to a CMP formula, often having been breastfed for several months. In babies who have been formula-fed since birth, the presentation may be more insidious. Babies usually develop the typical features outlined in Table 3. These symptoms will only occur on exposure to CMP formula milk or products containing it. As for all childhood food allergy, eczema is a risk factor. Blood specific IgE or SPT to milk will confirm the diagnosis and exclusion of CMP is the mainstay of treatment. There are several alternative formulas available for those allergic to cow’s milk (see below). There is evidence that regular exposure to baked milk, if tolerated, accelerates the acquisition of tolerance to regular milk.
Non-IgE-mediated CMPA
For a small number of children with common conditions of infancy such as constipation, infant colic and gastro-oesophageal reflux, their symptoms may be caused by non-IgE-mediated CMPA. Clues are often to be found in the association with other atopic features (eg. eczema), multiple symptoms (eg. GOR and constipation) or a family history of atopy. Non-IgE-mediated CMPA should be considered on the basis of severity of symptoms and their impact on family life. The ultimate test for this group of conditions is the withdrawal and reintroduction of milk at home, unless there are concerns about IgE-mediated disease.
Formula milks
Where possible, breast milk is the preferred feed for all infants. Rarely, an infant may react to the very small amounts of CMP secreted intact into human breast milk. If this is considered possible then, with dietitian input, a mother should be requested to exclude CMP from her diet for a trial period. Where breastfeeding is not possible, there are many formula milks available. Most are based on CMP.
Regular formula contains unadulterated CMP. The process of hydrolysation can be used to break down the protein into small fragments which are less recognisable to the immune system. Partially hydrolysed formulae do not have a role in the management of suspected milk protein allergy, although they may have a role in the prevention of allergy in high-risk individuals. Extensively hydrolysed (Aptamil Pepti, Nutramigen) and amino acid formulae (Neocate, Nutramigen AA) are used for confirmed CMPA. Most babies with CMPA will tolerate extensively hydrolysed formula, which is less expensive than amino acid formulae.
Babies who have not tolerated extensively hydrolysed formula or who had an initial severe reaction may require an amino acid formula. These adapted CMP formulae are recommended for any baby under six months. Soy-based formulae may be used for babies over six months, but are avoided in younger babies because of the likelihood of developing soy allergy. Other mammalian milks are not recommended (sheep/goat) because of high cross-reactivity and poor nutritional composition. Other plant-based milks (oat, pea, almond milk, etc) are not recommended in children less than two years because they will not meet nutritional requirements. Rice milk is not recommended in children less than five years old because of concerns regarding arsenic levels.
Lactose intolerance
Lactose intolerance is due to an inability to digest lactose, the disaccharide found in milk and other dairy products. There are three major types of lactose intolerance in infancy: congenital, primary and secondary. Congenital absence of intestinal lactase is a rare but severe condition, which presents in the neonatal period with loose stools from initial exposure to either human or formula milk, which contains lactose. There is subsequent failure to gain weight, poor growth and lifelong symptoms if a diet excluding lactose is not followed. Primary lactase deficiency (hypolactasia) is a relatively common condition caused by a deregulation of the lactase gene expression. In Ireland, up to 4% of the total population may have deficiency in intestinal lactase; however in the majority of patients symptoms may not develop until late childhood or adulthood. Secondary lactose intolerance refers to those infants who have previously tolerated lactose-containing feeds, but subsequently lose lactase enzyme activity secondary to inflammatory or structural damage to the small intestinal mucosa. The most common cause of secondary lactose intolerance is postviral gastroenteritis, in particular post rotavirus infection.
The symptoms of lactose intolerance include abdominal cramps, excessive flatus, explosive loose stools, abdominal distension and perianal excoriation due to an increased lactic acid concentration in stools. In infancy, the diagnosis is usually made by trial on lactose elimination diet followed by re-challenge and therefore invasive testing is rarely needed. There are several lactose-free infant formulas available including those based on whole CMP, extensively hydrolysed, amino acids or soy. Children on a diet excluding conventional dairy products, eg. milk, cheese and yogurt, should receive appropriate dietary supplementation to prevent deficiency in important fat-soluble vitamins and other elements, in particular calcium and vitamin D.
Egg allergy
Egg allergy is unusual in that when egg is baked it becomes less allergenic. Raw or lightly cooked egg (scrambled egg, omelette) is most allergenic, included in this group are mayonnaise and meringues. Baked egg products are less so, with children often becoming tolerant to cakes and sponges while remaining reactive to lightly cooked products. Eating baked egg seems to accelerate the resolution of allergy to lightly cooked egg. It is import to stress that the MMR vaccine does not contain egg and that children with egg allergy should be vaccinated in the community the same as everyone else. Influenza and yellow fever vaccines may contain egg and should be avoided or discussed with a paediatrician.
Nut allergy
Up to 2% of children in the UK are estimated to be nut (peanut and/or tree nut) allergic. Peanut (a ground nut) is the most common nut allergy. The most common tree nut allergies are hazelnut and cashew nut. There are some cross-reactivities between tree nuts. Nuts seem to provoke more severe reactions than other foods and therefore adrenaline is prescribed even if previous reactions were mild. As with all food allergies, it is not possible to predict the nature of future reactions on the basis of previous reactions; they may be more or less severe. Avoiding nuts is difficult because they are in many foods and because of labels such as ‘may contain traces’. While efforts are afoot to improve labelling, parents should be encouraged to avoid foods with such warnings. This cautious approach can be summed up as ‘No label, no eat. No adrenaline, no eat’. Most children with nut allergies do not outgrow them; however they will need assessment to see if they are among the many or the few.
Management of diagnosed food allergy
Once a diagnosis of food allergy is confirmed, then a management plan should be recommended to the child and family. An important feature of this plan is a risk assessment as to the likelihood of a severe reaction or anaphylaxis occurring. Elimination diets and the prescription of adrenaline or other medications is outlined below.
Children and families should have a written allergy plan which can be shared with school. The plan should name the food which the child is avoiding and clearly define the features of a (mild to moderate or severe) reaction and the appropriate action needed in response.
An example of a food allergy plan is available under the ‘medication for food allergy’ tab on www.ifan.ie
Elimination diets
In one sense the management of food allergy is simple in that the implicated food should be excluded from the diet. In the case of non-IgE-mediated allergy, this may be for a period of four to six weeks before reintroduction to see if symptoms recur. In the case of IgE-mediated allergy, once confirmed the food is usually excluded for longer periods until further testing suggests that it is safe to reintroduce the food. For most foods this will mean a formal food challenge in hospital although in certain cases (eg. baked egg) this could be undertaken at home once a thorough risk assessment has occurred to ensure this would be safe to do.
In reality, avoiding eg. milk, eggs and nuts is difficult as they are often ingredients in other foods. Educating parents in this regard and ensuring they can read food labels is an essential component of management. Printed information is freely available for the dietary management of many food allergies (see www.bsaci.org). Dietitian input is always helpful but is usually not necessary for single food allergies. It is however essential for children with multiple food allergies or where there are difficulties finding suitable foods or whenever there are concerns about faltering growth.
Advice about high-risk situations or times is useful. Eating outside of home, especially if abroad, requires caution. Always inform the chef (not the waiter) of the specific allergy at a restaurant and encourage finger dipping a small amount before eating a mouthful are useful tips. Teenage years are seen as higher risk as many teenagers push the safer boundaries of home. Education and awareness often help here.
Medication – adrenaline and antihistamines
Although avoidance is the cornerstone of treatment, many children will have accidental exposures to the food to which they are allergic to, and some will react to new foods. Whether medication is required after exposure is dependent on the severity of the reaction that occurs. The most commonly used medication to treat allergic reactions is antihistamine. A non-sedating antihistamine should be easily accessible to all children with known food allergy for the management of mild to moderate reactions. The management of severe allergic or anaphylactic reactions requires intramuscular adrenaline as the first-line treatment. Other medications such as oxygen, bronchodilators and antihistamines may also be required once the adrenaline is administered (or while waiting for it). There are international guidelines as to who requires an adrenaline autoinjector (see Table 4). Although included among the relative indications, it is our practice to recommend adrenaline to all children with a confirmed nut allergy.
(click to enlarge)
If adrenaline is prescribed then it is incumbent upon the prescriber that the indications for use and how to use it are clearly explained and demonstrated. Currently there are three devices on the Irish market: Anapen, Epipen and Jext. Materials to assist with training are available on www.ifan.ie (under the ‘medication for food allergy’ tab).Adrenaline autoinjectors contain adrenaline 1:1,000. Children greater than 10kg and less than 30kg should be prescribed 150µg (0.15mg) of adrenaline. Children over 30kg require 300µg (0.3mg) of adrenaline. Children less than 10kg who require adrenaline should be managed by a paediatrician. It is advisable that two devices are with the child at all times because in a quarter of cases where adrenaline is given a second dose will be required. Adrenaline has a short shelf life so it is important to check devices regularly to ensure they are ‘in date and in weight’.
A major risk factor for having a severe or even fatal food allergic reaction is the presence of asthma, especially when poorly controlled. Special attention must be given to children with co-existing food allergy and asthma and they must have their asthma treatment stepped up until it is well controlled.
Natural history of food allergy
The common food allergies of early childhood (milk, egg and wheat) are likely to be outgrown by most (over 90% of children by middle childhood). Unfortunately for other common allergies such as peanut, tree nut, fish or shellfish the odds are almost reversed with only 10-20% of these conditions resolving spontaneously. Allergy testing is helpful for predicting when children are likely to have outgrown their allergy and who may need a food challenge to confirm this. A recent change in practice is the recommendation that if baked egg or baked milk products are tolerated that they should be eaten regularly (a few times each week) to accelerate the acquisition of tolerance to uncooked or lightly cooked products. Whereas there is much research ongoing into treatments for nut allergy, with some well publicised successes, most treatments are experimental and are not currently available in Ireland.
Who needs referral?
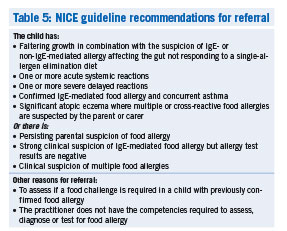
Many children with food allergy will need assessment by a paediatrician or a paediatric allergist. There is good evidence now that seeing a paediatrician with experience in managing allergic disease improves patient outcomes and reduces the risk of more severe reactions. The recommendations for referral made in the recent NICE guideline on diagnosis and assessment of food allergy in children and young people in primary care and community settings are included in Table 5. Outside of the scope of this guideline are children with previously confirmed IgE-mediated allergy, who will need referral to assess if a food challenge is required so as to cease unnecessary elimination diets. All of the recommendations in the NICE guideline are dependent on the healthcare professional having the appropriate competencies to diagnose and assess. If a practitioner does not consider themselves competent in this regard then referral is also indicated.
Food hypersensitivities are commonly seen in primary care. With an allergy-focused history, examination and testing it is possible to identify those with food allergy and even to distinguish between IgE- and non-IgE-mediated allergies. This is important as some of these children are at risk of severe or even life-threatening reactions. Once food allergy is confirmed, an elimination diet with dietary advice and an allergy plan describing when and how to use the correct medications are what most patients require.
(click to enlarge)
Conclusion
Children require ongoing assessment as to whether they should continue an elimination diet as many will outgrow the need for this. In most cases an oral food challenge, which can only be performed in hospital, is required to make this decision safely. Finally, because food allergy is common, on the increase and an important cause of concern for children and families, GPs need to acquire the competencies to diagnose and assess children. It is important that this is recognised at a national level to make provision for these children and their families in primary and secondary care and that plans are put in place to facilitate the training required.
 (click to enlarge)
(click to enlarge)