GENERAL MEDICINE
Clinical case teaching – hospital vs community
A Donegal study found that clinical case teaching in the community was more frequent and of longer duration than that in the hospital setting
February 7, 2014
-
We undertook an analysis of trainee’s experience of clinical case teaching on the Donegal Specialist General Practice Training Scheme (DSGPTS). We compared clinical case teaching opportunities in hospital with those in community settings. We examined what impact if any, changes in hospital work practices to facilitate the implementation of the European Working Time Directive (EWTD) had on clinical case teaching opportunities.1
William Osler observed “the clinical case should be at the centre of clinical teaching”.2 Linda Hutchinson described the clinical teaching of cases in the real world as the basis of the ‘apprenticeship model’ of medical education. She acknowledges that the pressure for clinicians to provide a service is impacting on teaching commitments. She contests “the apprenticeship model is open to abuse, but should be the basis of all healthcare education”.3
Background
The DSGPTS has 24 trainees. First year trainees rotate through medicine, medicine for the elderly and emergency medicine. Second year trainees spend four months in each of paediatrics, obstetrics and gynaecology, and psychiatry. All hospital rotations are based in Letterkenny General Hospital (LGH). Third-year trainees spend six months each in two different training practices in the community. Fourth year trainees spend either the full year in a training practice in Donegal or, 10 months in a Donegal training practice followed by two months in a training practice in Australia.
Aim of the study
We believe that there is a perception amongst GP trainees that clinical case teaching is superior in community settings, perhaps due to closer mentoring and more GP focused teaching. We wished to analyse whether this was the case, following changes in working practices across the hospital. These changes included reduction in medical staffing numbers and the use of a ward-based system introduced in 2010 in certain specialties to facilitate implementation of the EWTD. Senior house officers (SHOs) previously worked under one consultant for four months and provided clinical care to that consultant’s patients. With the ward-based system, SHOs are based on a particular ward and care for all patients on that ward regardless of which consultant is responsible for the patient. We wished to establish whether clinical case teaching had been impacted by these changes.
Methods
A 33-item questionnaire was designed by Dr Browne to measure qualitative and quantitative data related to clinical case teaching. This was distributed at the DSGPTS half-day release on March 31, 2011 and again on April 6, 2011.
The questionnaire contained four sections. Section A contained demographic questions, Section B examined exposure to clinical case teaching in hospital including frequency, duration of each session and total duration of teaching per week. Section C was similar to section B, focusing on clinical case teaching in community settings. Section D questions examined what worked well and what could be improved with regard to clinical case teaching. Section D also included questions on what effects, if any, implementation of the European Working Time Directive had on clinical case teaching.
Results
A total of 21/24 (87.5%) questionnaires were completed, (12 males, 12 females), 83% of males and 92% of females completed questionnaires.
Trainee feedback re ETWD effect on clinical case teaching
GP trainee No 3: “Teaching used to be on ward rounds. Now, as the consultant has a new SHO every day, this can affect teaching. Also, with constantly changing teams, journal clubs and case presentations cannot be organised”.
GP trainee No 4: “On call is regular, so lunchtime teaching is frequently missed, as you can’t go on call, and we finish at 11am post-take and cannot be around at lunchtime.”
GP trainee No 7: “Working hours are the same now as before EWTD”. GP trainee No 8: “EWTD? I will do 71 hours this week and have not been EWTD-compliant in any of the hospital jobs bar psychiatry”.
Discussion
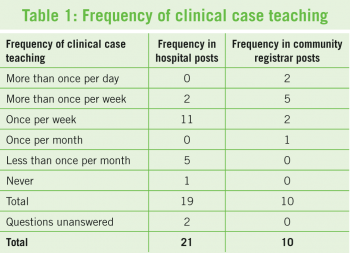
Our study found that 95% of hospital-based trainees were receiving clinical case teaching; however only 19% of this group (three out of 16 trainees), had clinical case teaching for more than one hour per week. The majority of trainees were receiving clinical case teaching despite changes to rosters and the introduction of a ward-based system in certain hospital specialties in LGH. EWTD compliance was not consistent through the hospital specialties. To facilitate compliance with EWTD some specialties released SHOs at 11am post-call. This resulted in some formal clinical teaching opportunities for GP trainees, including lunchtime teaching being missed.
Clinical case teaching in the community was more frequent and of longer duration than that received in hospital settings, with 100% of trainees having formal teaching each week. Despite busy surgeries and brief appointment times, GP trainers were still finding significant time for teaching, and in 89% of cases (eight out of nine trainees), this was for more than one hour per week.
Conclusions and recommendations
The majority of trainees were receiving clinical case teaching despite changes to rosters and the introduction of a ward based system to facilitate the implementation of the EWTD in Letterkenny General Hospital. To lessen the impact of EWTD compliance on clinical case teaching opportunities, consideration could be given to review scheduling of teaching sessions to facilitate attendance of post-call SHOs. Clinical case teaching has not been affected in the community setting. Feedback from the hospital-based trainees and general practice registrars on the DSGPTS was generally positive, reflecting enthusiastic hospital consultants and GP trainers who continue to provide significant clinical case teaching time, despite increased demands on their time and resources.
 (click to enlarge)
(click to enlarge)

