Colorectal metastases from cutaneous malignant melanoma
A 56-year-old man was referred by his GP with a three-month history of vague central abdominal pain, alteration of bowel habit and passage of dark stool
Dr Abed Mhomad, Surgical Registrar, South Infirmary Victoria University Hospital, Cork, Dr Amr Kazim, Surgical SHO, South Infirmary Victoria University Hospital, Cork, Dr Dean Moore, Surgical Intern, South Infirmary Victoria University Hospital, Cork and Mr Noel O'Brien, Consultant General Surgeon, South Infirmary Victoria University Hospital, Cork
Although metastases from malignant melanoma to the gastrointestinal tract (GIT) are found at autopsy in up to 60% of patients who died from disseminated melanoma, only 1-4% of all patients with malignant melanoma have clinically apparent GIT involvement and are diagnosed ante-mortem (as in this case).
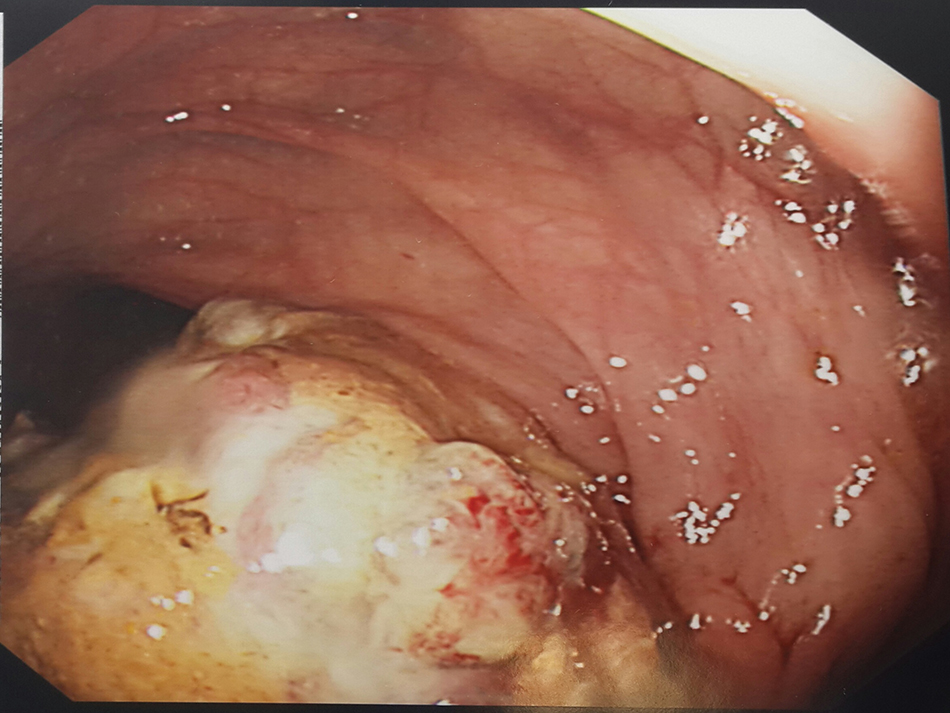
Figure 1. Colonic metastases from malignant melanoma(click to enlarge)
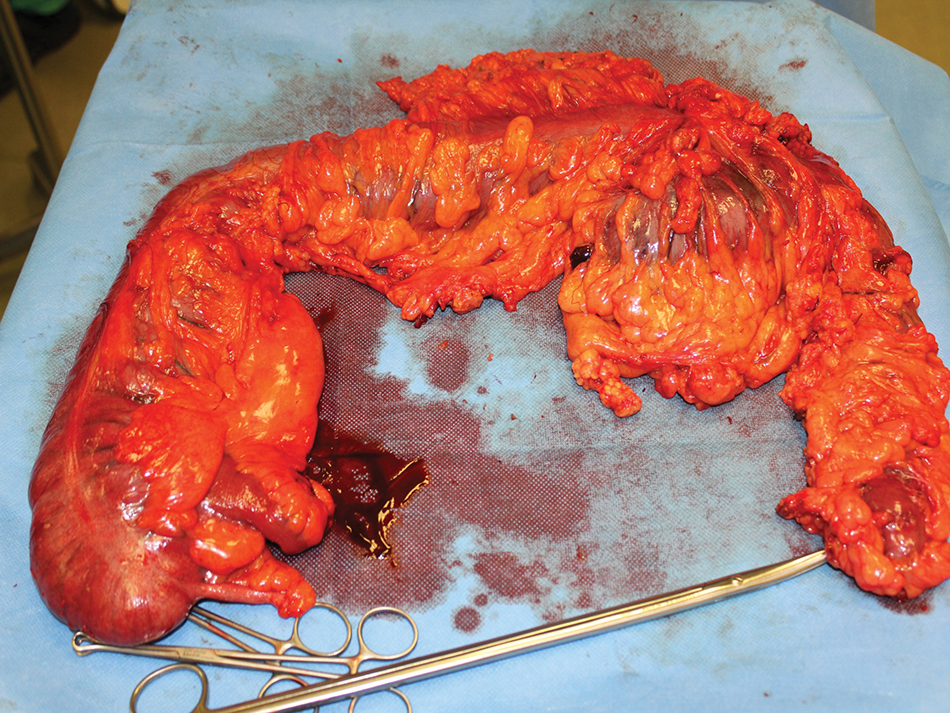
Figure 2. Right haemicolectomy(click to enlarge)
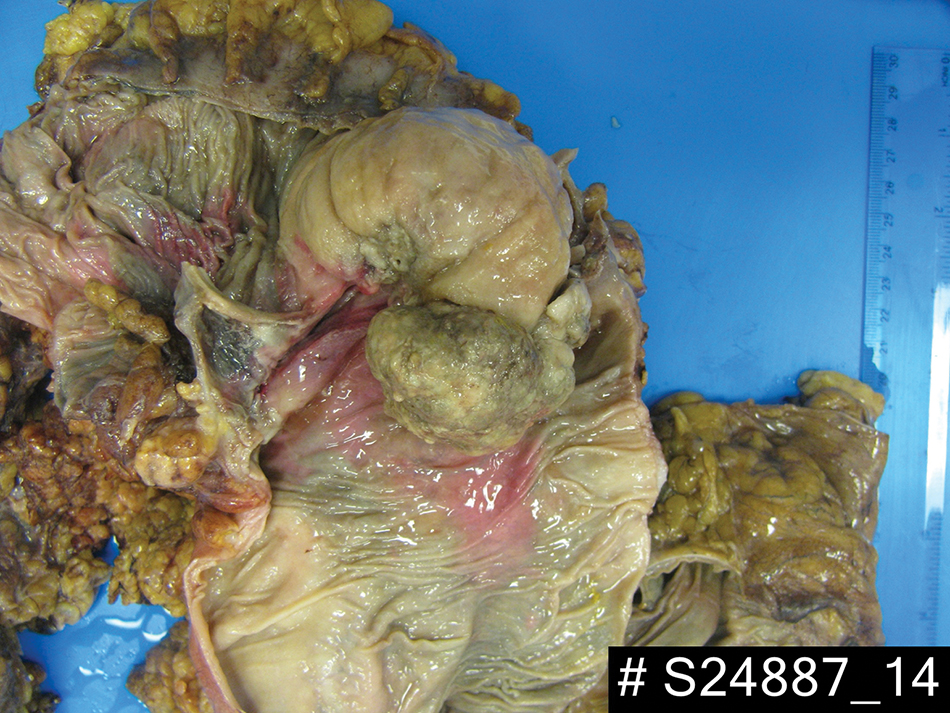
Figure 3. Pathology specimen(click to enlarge)
Case report
We report a case of colonic metastases from a cutaneous malignant melanoma in a 56-year-old man. The man had a history of malignant melanoma excised from the left calf three years previously, with left groin dissection. Two out of nine lymph nodes were positive; he had undergone a right breast lumpectomy for melanoma metastasis two years previously.
Investigation
FBC and biochemical profile were normal. Colonoscopy showed a tumour at 90cm. Multiple biopsies were taken and revealed metastatic malignant melanoma. Subsequent CT-TAP showed intussusception of distal transverse colon.
There was no evidence of obvious metastases elsewhere in the thorax, abdomen or pelvis.
Following a multidisciplinary team discussion he was taken to the theatre and an extended right haemicolectomy and omentectomy were performed. Because of bleeding from the spleen a splenectomy was performed.
The patient subsequently made an uneventful recovery. Histology confirmed metastatic malignant melanoma causing large bowel intussusception.
Discussion
The common sites for GIT metastases are the small bowel, stomach and the large bowel.
Some 1-3% of all malignant tumours of the GIT are secondary to metastatic malignant melanoma.
Symptoms are usually nonspecific, abdominal pain, anaemia, weakness, fatigue and bleeding, which is why the diagnosis is usually late and the prognosis is poor.
Approximately 30% require urgent surgery due to acute abdomen, secondary to bleeding, perforation, intussusceptions and bowel obstruction.
The diagnosis of metastatic malignant melanoma is pathologically confirmed at:
Surgical exploration in 80%
Endoscopy in 15%
Percutaneous biopsies in 5%.
Complete surgical resection remains the treatment of choice, although incomplete resection is still effective in palliation because more than 90% of patients are relieved of symptoms.
Alternatives to surgery
Alternative therapies to surgical resection of colon melanoma metastases include chemotherapy, biochemotherapy and radiation.
The effectiveness of adjuvant therapy including radiation, chemotherapy and immunotherapy used for residual disease or nodal metastases following surgical resection is still controversial. Complete resection and the absence of extra abdominal metastases at the time of operation are the most important prognostic factor; colonic metastases indicate late stage disease with poor prognosis, five-year survival following surgery is only 7%.
Conclusion
Patients with melanoma should have meticulous follow up, detailed history and rapid evaluation of any vague and unclear abdominal signs and symptoms and should be screened for GIT spread.
Currently, dual modality PET-CT is the most accurate in detecting and staging melanoma metastases. Colonoscopy has the greatest diagnostic value with high sensitivity and specificity for tissue biopsy.
 Figure 1. Colonic metastases from malignant melanoma(click to enlarge)
Figure 1. Colonic metastases from malignant melanoma(click to enlarge)