Choosing appropriate contraception is an important aspect of sexual health, write Dr Humera Khan, Dr Nikhil Purandare and Dr Maeve Eogan
Dr Humera K Khan, Registrar in Obstetrics and Gynaecology, Dept. of Obstetrics and Gynaecology, the Rotunda Hospital, Dublin, Dr Nikhil C Purandare, Specialist Registrar in Obstetrics and Gynaecology, Dept. of Obstetrics and Gynaecology, the Rotunda Hospital, Dublin and Dr Maeve Eogan, Consultant in Obstetrics and Gynaecology, Dept of Obstetrics and Gynaecology, the Rotunda Hospital, Dublin
In general, most GPs and practice nurses are well informed about contraceptive options but some women are referred to hospital for contraceptive advice, particularly those with significant comorbidities.
Barrier methods such as male and female condoms are proven methods of protection against sexually transmitted infections (STIs); they are commonly used and are cost-effective.1,2
Occlusive caps, diaphragms, vaginal sponges and spermicides are less popular because of slightly higher failure rates and inconvenience when compared to other contraceptive options. No barrier method is complete without spermicidal gel or cream, which make it more expensive and/or allergenic for some people.
The vaginal ring is relatively non-invasive, moderately long-acting and effective (similar or slightly better than the pill), and easy to use. Proven benefits of the vaginal ring include better cycle control and sexual satisfaction with a failure rate similar to the combined oral contraceptive (COC) pill, with no effect on efficacy due to diarrhoea or vomiting or risk of missing the dose.1,3,4
Hormonal contraception is almost 100% reliable if taken regularly and properly, it also frequently has the added benefit of a positive impact on cycle control.1 It is recommended that women aged more than 35 years who smoke more than 15 cigarettes a day avoid combined preparations.1 Non-oestrogen-containing methods like progesterone-only preparations, barrier methods or surgical methods may be safer options for these women.5
Women over the age of 40 who do not smoke and have no other comorbidities can use combined preparations until menopause.6 Women taking liver enzyme-inducing drugs like anti-epileptics and tuberculosis drugs (rifampicin) may not be suitable candidates for the use of hormonal contraceptives, as these drugs reduce the efficacy of such contraceptives by increasing their metabolism.7
WHO medical eligibility criteria (WHOMEC) and UK medical eligibility criteria (UKMEC) now advise no restriction on antibiotic use and hormonal contraception, ie. no extra precautions are now recommended provided the antibiotic is not an enzyme inducer.1,7,8
There are two different types of contraceptive intrauterine devices (IUDs): copper IUD (Cu-IUD and levonorgestrel-releasing intrauterine system (LNG-IUS).
The mode of action for Cu-IUD is primarily to prevent fertilisation for up to 10 years and for LNG-IUS to prevent implantation for up to five years. Both are completely reversible procedures. The failure rate for Cu-IUD is less than 2% and less than 1% for LNG-IUS.1
After insertion over the age of 40 years a Cu-IUD should be left in situ for one to two years after menopause, depending on age of menopause, while the LNG-IUS can be retained until menopause is confirmed or until contraception is no longer required if inserted over the age of 45.9
Risks and complications of IUDs
• Uterine perforation at the time of insertion: overall risk is up to 2/1,000 insertions9
• Expulsion of IUD is reported to occur in one in 20 women, particularly within three months of insertion9
• Ectopic pregnancy risk is lower when compared to non-contraceptive users. With Cu-IUD, risk is 0.02/100 women years (WY) as compared to non-users, which is 0.3-0.5/100 WY9
• Pelvic infection risk is more common in the first 20 days of insertion, when there is a sixfold increase in the risk but, thereafter, risk is the same as for non-users9
• Bleeding and pain are common reasons for discontinuation. These symptoms usually settle within six to 12 months of insertion9
• Lost threads can be retrieved by Spencer Wells forceps or thread retriever; until then, effective contraception should be advised. Arrange ultrasound (US) if thread retrieval is unsuccessful. If IUD is not located on US, then a plain x-ray should be arranged to exclude an extra-uterine location of IUD
• Pregnancy with an IUD in situ is associated with an increased risk of second-trimester miscarriage, preterm delivery, and infection if the IUD is left in situ. If it is removed, there is a small risk of miscarriage. If pregnancy is confirmed and threads are visible then it should be removed up to 12 weeks gestation.9
(click to enlarge)
Vasectomy and tubal occlusion
Vasectomy can be performed in primary care or specialist clinics. Female sterilisation is generally performed in hospital; there are two main techniques: laparoscopic tubal ligation or hysteroscopic sterilisation.
Hysteroscopic tubal occlusion (Essure) may be a safer surgical sterilisation procedure for obese women because it can be done without general anesthesia and does not require entrance into the abdominal cavity, but few centres currently perform this technique in this country.10,11
Contraceptive use in high-risk women
The majority of women using contraceptives are medically fit and can use any method safely. However, some women have certain medical conditions that make the choice of contraceptive difficult.
The efficacy of certain contraceptives may be reduced due to a concurrent medical condition or its treatment and indeed some contraceptives may exacerbate or complicate the condition.
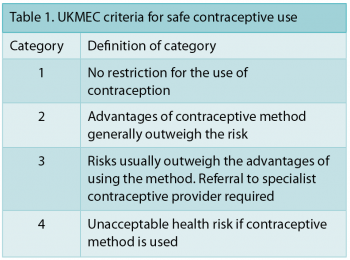
Safe contraceptive use by women with certain medical conditions or by those who are using certain drugs can be achieved by consulting WHOMEC and UKMEC as described in Table 1.12 Medical conditions (UKMEC 3 and 4) often require hospital referral for contraceptive advice.
Contraceptive options in certain medical conditions are discussed below but this list is by no means exhaustive and hospital referral or specialist advice may be required in the context of other clinical issues.
Medical conditions and risks
Diabetes
In non-vascular disease, the COC has only limited effect on insulin requirement and no effect on long-term diabetic control or progression to diabetic complications. The barrier method and Cu-IUD can be used without restriction.
COC pills, patches and rings, progestogen pills, implants, injectables and LNG-IUS, sterilisation should be undertaken with caution.13
Vascular disease or diabetes for more than 20 years is WHO 3/4, ie. choice of contraception will depend on the severity of disease. LNG-IUS, progestogen pills and implants can generally be used while the risks with progestogen injectables usually outweigh the advantages. COC pills, patches and rings should not be used.13
Epilepsy
Women who have a history of epilepsy but are not on any medication, or women who are on anticonvulsants which are not liver enzyme inducers like sodium valproate, gabapentin, vigabatrin and levetiracetum, can use any method of contraception. Sterilisation should be undertaken with caution when seizure control is adequate.13
Women using liver enzyme-inducing anticonvulsants like phenytoin, primidone, barbiturates, carbamazepine, topiramate and oxcarbazepine, can use natural methods, barrier methods, IUDs and progestogen injectables without restriction. COC pills, patches and rings and progestogen-only pills (POPs) and implants should not be used. If COCs are to be used, dose adjustment will be needed but should generally not be used.13
Migraine
Women with migraine without aura can use natural methods, barrier methods and Cu-IUD. Progestogen pills, injectables, implants and LNG-IUS should be used with caution. COC pills, implants and rings can be initiated but should not be used long term as risks outweigh benefits.13
In migraine with aura natural methods, barrier methods and Cu-IUD can be used without restriction. POPs, implants and injectables and LNG-IUS can be used with caution while COC pills, patches, and rings should not be used.13
Hypertension
There is a slight increase in blood pressure within normotensive range in women taking COC pills. With modern low doses, fewer than 1% will become hypertensive; the rate increases with age and duration of use.
Essential hypertension is WHOMEC 3, ie. if an acceptable effective alternative is available, then it is better not to use COC. Natural methods, barrier methods, progestogen pills and implants, IUDs and IUS can be used without restriction. Sterilisation should only be done after blood pressure control has been achieved.13
Cardiovascular disease
Women with cardiovascular disease who are older, obese, diabetic, hypertensive or those who smoke can use natural methods, the barrier method or Cu-IUD without restriction. They can use POPs, implants, LNG-IUS and sterilisation with caution. Progestogen injectables, COC pills, patches and rings should generally not be used.6,13,14
Smoking
Women aged 35 years or more, who smoke 15 or more cigarettes per day, can use natural methods, barrier methods, progestogen pills, injectables and implants, Cu-IUD, LNG-IUS and sterilisation. COC pills, implants and rings should not be used as smoking increases the risk of myocardial infarction.6,13,14
Venous thromboembolism (VTE)
Women with thromboembolism can use natural methods, barrier methods and Cu-IUDs. POPs, implants, injectables and LNG-IUS can generally be used. COC pills, patches and rings should not be used. The risk of VTE is 5/100,000 WY, in a healthy, non-pregnant woman who is not on any contraceptive pill. This risk increased to 15/100,000 WY if they are on second-generation pills and again increased to 25/100,000 WY if on third-generation pills. Pregnancy increases this risk to 60/100,000 WY.
Women on the combined pill who are homozygous for the factor V Leiden mutation have a 35-fold risk of developing VTE as compared to non-pill users.13,14,15
Obesity
Women with body mass index (BMI) of > 35 can use natural methods, barrier methods, progestogen pills (according to the Faculty of Family Planning and Reproductive Health Care [FFPRHC], POPs may be less effective in women weighing more than 70kg, desogestrel pill could be a better choice), injectables, implants (consider earlier replacement of implant in heavier women), IUD and IUS without any restriction. Sterilisation should be done with caution as risks of operative difficulties and post-operative complications including infection are high. COC pills, implants and rings should generally not be used.13,16,17
Pelvic inflammatory disease and sexually transmitted infections
All methods can be used if there is no current risk of STI. In women with current pelvic inflammatory disease (PID) or STI, all methods can be used except for IUD and IUS. Women with signs and symptoms of PID, who also have an IUD or IUS in situ, need appropriate antibiotic cover.
Some data suggest that there is no need to remove the device immediately but that it should be removed if symptoms do not improve after 72 hours of treatment.9,14 Nevertheless, in our experience an IUD is frequently removed immediately a diagnosis of PID is considered, particularly if it occurs soon after insertion of same.
Breast cancer
Risk of breast cancer is very small under the age of 35. The risk of breast cancer in a young woman using COC pill is 11/1,000 as compared to 10/1,000 in non-pill users. There is no increased risk after the discontinuation of pill for 10 years.1 The Society of Family Planning recommends that young women with breast cancer should avoid COCs because of the increased risk of VTE. The Cu-IUD could be the first choice in these cases as it is hormone-free and reliable. For women on tamoxifen, the LNG-IUS could be the better choice as it decreases endometrial proliferation. Progestogen injectables should best be avoided in women who develop osteopenia or osteoporosis after chemotherapy as they are associated with a further slight loss of bone mineral density.13,18
Liver cancer
There is relative increase in benign adenoma or hamartoma with the use of COC. COCs should not be used with a past history of tumour but other hormonal contraception can be used with caution.1 There is some weak evidence that low-dose COC or progesterone-only contraception in benign liver disease does not influence the resolution or progression of the disease.19
Conclusion
This article aims to assist with choice regarding contraceptive use in patients with specific medical conditions.
Nevertheless, it is important to remember that in many cases the risk of pregnancy may outweigh the risk of specific contraceptives, and therefore each case must be considered individually in the context of patient preference and the best available evidence before making a final decision on contraceptive choice.
 (click to enlarge)
(click to enlarge)