Contraception, when used regularly and consistently, can prevent unplanned pregnancy. The latest research on crisis pregnancy in Ireland shows that the most common reason for not using contraception in teenagers is that they were not prepared for or had unplanned sex.1
Statistics show that those in the 18-26 year age group, who repeatedly have unprotected intercourse, have a 50% possibility of pregnancy.2 Psychological stress associated with unplanned pregnancy and young age may lead to relationship problems, childcare and financial difficulties.
Counselling
The doctor should maintain professionalism and communication skills during consultation while dealing with young women. The consultation should be very sensitive with a friendly manner so that the patients feel comfortable and able to express their wishes. The doctor should try to build confidence in them and alleviate their fear about confidentiality. Counselling involves detailed discussion of various methods available, providing clear and non-judgemental information, and outlining the benefits and risks of each method. During counselling it is important to highlight the issue that hormonal contraception does not protect against sexually transmitted infections (STIs). Women on hormonal contraception should be clearly informed about STIs and use of a barrier method (male/female condom) to reduce the risk for STIs.3,4 It has been revealed in the ISSHR that the younger the age when having sex for the first time (before age 17) is associated with unintended pregnancy and acquiring STIs.5
Different contraceptive methods
Natural methods
Educating teenagers about natural family planning methods may help them to take precautions or avoid sex altogether to prevent pregnancy happening. The first day of a period is calculated as day one. Day one to seven and day 21 to the rest of the cycle is calculated as the ‘safe period’.
Hormonal contraceptive methods
These may include:
‘The pill’: combined oral contraceptive pill (oestrogen and progestogen)
The progestogen-only pill (POP; or mini-pill)
Injectable hormones: progestogen
Implant: progestogen
Patches
Vaginal rings
Coil: intrauterine contraceptive device (ICUD).
Barrier methods include the female condom and natural methods include the safe period method and abstinence.
Oral contraceptive pills
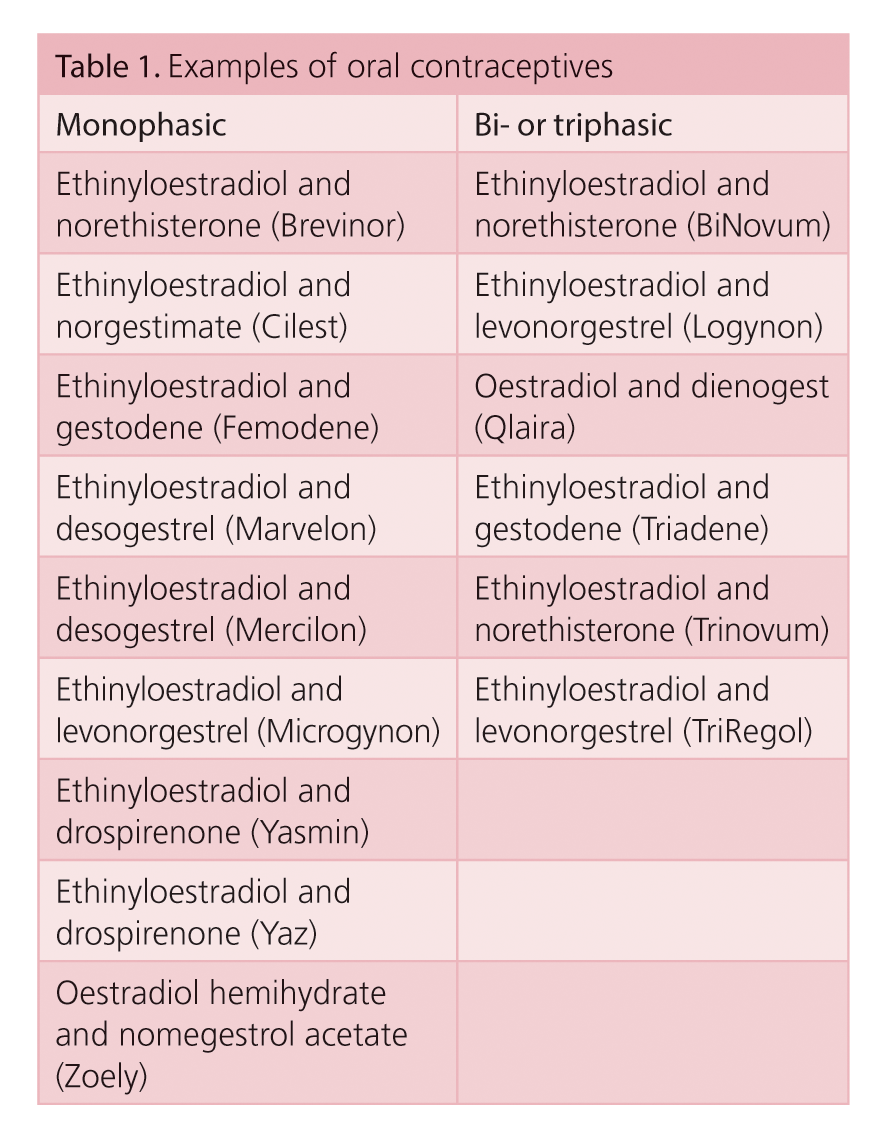
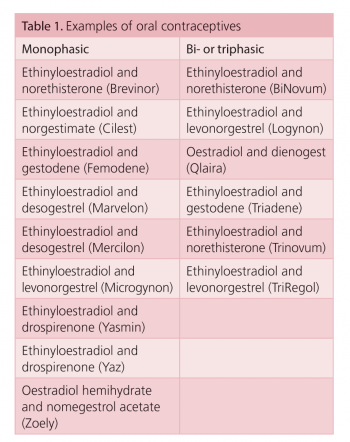
There is a wide range of oral contraceptives on the market (see Table 1 for examples).
Combined pills contain a combination of oestrogen and progestogen either in fixed dose in every tablet (monophasic) or different levels of hormone at different times of the month (biphasic/triphasic). Co-cyprindiol (Dianette) is prescribed for severe acne vulgaris and is also licensed as a contraceptive, but only in this group requiring treatment for androgen-dependent acne. The mechanism of action is by interfering with gonadotrophin-releasing hormone, preventing ovulation and also modifying the endometrium.
(click to enlarge)
Advantages
The pill is the most effective method of reversible contraception. It has non-hormonal benefits such as improving dysmenorrhoea or heavy periods, regulating the cycles and also premenstrual symptoms. It lowers the risk of developing ovarian cysts and is protective against ovarian and endometrial cancer, and reduces the severity of endometriosis.
Side-effects
Side-effects vary from minor to life-threatening complications. There may be some nausea, vomiting and breast tenderness. Young women often blame the pill on associated weight gain. They should be warned to watch their weight while on the pill.
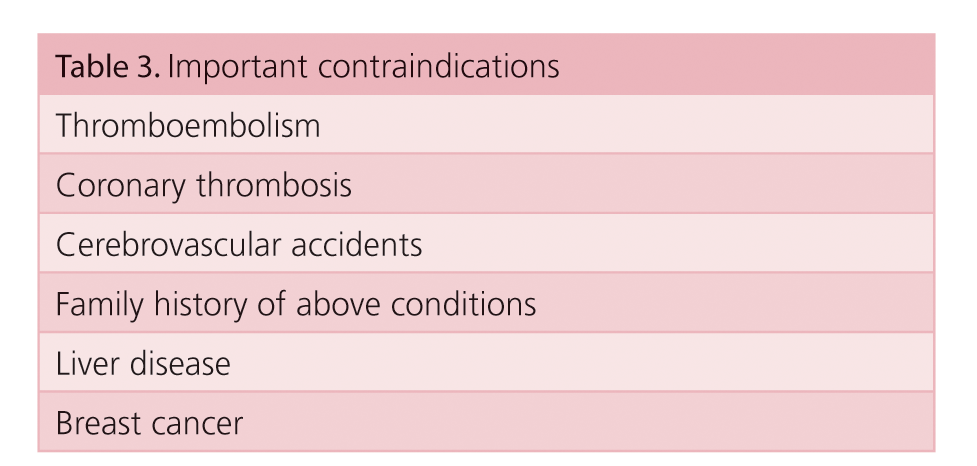
There may be breakthrough bleeding, which is possible in the first two cycles and may require a bigger dose of oestrogen if it persists. Thromboembolism may occur and is associated with high oestrogen dosage.
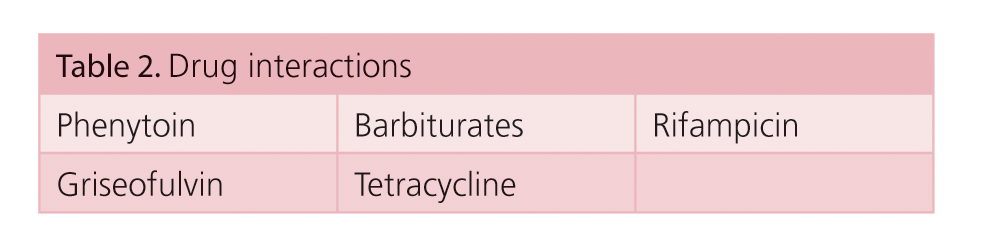
Migraine and depression may occur and advice should be given to stop the pill. The pill can interact with some drugs (see Table 2) and consider a stronger pill.
Prior to prescribing the pill, a careful personal and family history should be taken. Examination of blood pressure, weight, auscultation of the heart, breast and pelvic examination should be performed.
Patients should be advised to take a missed pill as soon as it is realised. Within 12 hours of missed period it is safe to continue. The patient needs to take additional protection for the remaining cycle after 12 hours of delay. The pill may not be effective when diarrhoea or vomiting occurs and additional protection is recommended for the remaining cycle. The female condom is not widely available and it is more expensive.
(click to enlarge)
Injectable hormonal contraception
The most popular progesterone, Depo-Provera, involves injection every 12 weeks. Depo-Provera inhibits ovulation, altering the tubal motility and changing the cervical mucous. The benefit of Depo-Provera is that it is a highly effective contraception, improves menorrhagia, irregular cycles, endometriosis, dysmenorrhoea and protects against ovarian cysts and endometrial cancer.
Disadvantages
A risk of weight gain
Depression
Loss of bone density in long-term users
May delay fertility in some women.
Implantable contraception
Implantable contraception (Implanon or Nexplanon) consists of a small, flexible plastic tube containing the progestogen and needs insertion by the doctor under the skin of the upper arm. It lasts for three years.
Nexplanon, a new implant, is similar to Implanon. Nexplanon is designed to reduce risk of insertion errors and is (radio-opaque) visible on x-ray or CT scan and MRI.6
Contraceptive patches
Evra is an effective combined contraception with a standard oestrogen and the progestogen called norelgestromin. The side-effects and mechanism of action are the same as the pill. The main advantage of the patch is that it needs only to be changed weekly.
The progestogen-only pill
The POP is not as popular as the combined pill and its satisfactory contraception depends on compliance, which is poor in young ages. Disadvantages of the POP are that it has to be taken continuously without a break, and may not control the cycle well like the combined pill.
The various kinds of mini-pills include:
Group 1: Micronor, Noriday – contain norethisterone
Group 2: Femulen – contains ethynodiol dictate
Group 3: Norgeston – contains levonorgestrel
Group 4: Creosote – contains desogestrel.
The vaginal contraceptive ring (NuvaRing)
This is a flexible plastic ring containing both oestrogen and progestin hormones and placed in the vagina for three weeks. During the fourth week, menstruation occurs and a new ring is inserted on day eight. The pros and cons of the ring are similar to the combined pill. It will not interfere with intercourse and is easy to use.
Intrauterine contraceptive device (IUCD)
The IUCDs include the Mirena coil (levonorgestrel), and the copper IUCD (Nova T). The two devices work differently. The copper device releases copper locally and prevents implantation and interferes with sperm motility. The levonorgestrel is locally released which thickens the cervical mucous and thins out the endometrium.
The IUCD is not an ideal option in young women who never had a pregnancy before. The risk of pelvic inflammatory disease may be increased during the first month after an IUCD insertion. After the first month, the risk of pelvic inflammatory disease (PID) is dependent on the exposure to STIs. Younger women should be carefully counselled before the IUCD insertion and backed up with an information leaflet. A study on IUCD-associated complications in younger women under 18 years of age shows that the complications are higher and recommends careful counselling prior to IUCD insertion.7 The IUCD should be inserted under meticulous asepsis and prior chlamydia screening is recommended.
(click to enlarge)
Conclusion
All young women should receive unbiased advice on all contraception. Improving access to all methods of contraception in general practice and family planning clinics may help young women to avoid unwanted pregnancies and STIs.
References
The Irish Study of Sexual Health and Relationships (ISSHR) 2006
Westhoff C. Emergency contraception. N Engl J Med 2003; 346: 1830-1835
Condom fact sheet in brief. Available at http://www.cdc.gov/condomeffectiveness/docs/Condom_fact_Sheet_in_brief.pdf. CDC. Sexually transmitted diseases treatment guidelines, 2006.
MMWR 2006; 55(RR No. 11)
Layte et al. (2006). The Irish Sexual Health and Relationships. Crisis Pregnancy and Department of Health and Children Report. Dublin.
Nexaplanon, Faculty of Sexual and Reproductive Healthcare Clinical Effectiveness Unit, CEU Statement (September 2010)
Rasheed SM, Abdelmonem AM. Complications among adolescents using copper intrauterine contraceptive devices. Int J Gynaecol Obstet 2011; 115(3): 269-272
 (click to enlarge)
(click to enlarge)